

76b806e47d890baa4ab0d8db8bb858ec.ppt
- Количество слайдов: 34
 www. oasis-open. org Future of EDXL Standards Presented by: Kevin Mc. Ginnis, Program Advisor, National Association of State EMS Officials (NASEMSO) & PSG Co-Chair John Donahue, Chief of Regional Programs and Emergency Operations, Maryland Institute for EMS Systems (MIEMSS) Jeff Sexton, Tennessee Department of Health, Office of Information Technology Services, Preparedness and Response Systems, HITSP Dr. Greg Mears, Medical Director & UNC Chapel Hill EMS, HITSP Capt. F. Christy Music, Program Director, Health & Medical Defense Support of Civil Authorities OASD (HD&ASA), Department of Defense Timothy Grapes (moderator), VP, Evolution Technologies, OASIS EM TC Voting Member , NIEM EM Domain Support
www. oasis-open. org Future of EDXL Standards Presented by: Kevin Mc. Ginnis, Program Advisor, National Association of State EMS Officials (NASEMSO) & PSG Co-Chair John Donahue, Chief of Regional Programs and Emergency Operations, Maryland Institute for EMS Systems (MIEMSS) Jeff Sexton, Tennessee Department of Health, Office of Information Technology Services, Preparedness and Response Systems, HITSP Dr. Greg Mears, Medical Director & UNC Chapel Hill EMS, HITSP Capt. F. Christy Music, Program Director, Health & Medical Defense Support of Civil Authorities OASD (HD&ASA), Department of Defense Timothy Grapes (moderator), VP, Evolution Technologies, OASIS EM TC Voting Member , NIEM EM Domain Support
 > Isn’t proliferation of one-off system interfaces and proprietary solutions just paving over the cow path? You bet it is. Fact is, there’s no lone system or solution to interoperability. >> You’ll always have your own systems and they’ll be different - requiring data sharing across systems using common protocols. >>> Cross-profession collaboration, open systems and interfaces, and standards-based exchanges are the easy-to-implement, lowcost solution across local, state and federal lines. These panelists don’t believe in paving the same old cow path…
> Isn’t proliferation of one-off system interfaces and proprietary solutions just paving over the cow path? You bet it is. Fact is, there’s no lone system or solution to interoperability. >> You’ll always have your own systems and they’ll be different - requiring data sharing across systems using common protocols. >>> Cross-profession collaboration, open systems and interfaces, and standards-based exchanges are the easy-to-implement, lowcost solution across local, state and federal lines. These panelists don’t believe in paving the same old cow path…
 The Emergency / Disaster Interoperability Challenge n n n Responders often cannot talk within their own agencies—let alone other agencies — or across cities, counties, and states. Ineffective communications risk the lives of responders in the field, and for those awaiting help. There is no one “Silver Bullet” to solve interoperability challenges. The interoperability landscape consists of 60, 000 state and local public safety agencies, Federal agencies and other stakeholders. 60, 000 agencies means 60, 000 different sets of procurement regulations, budgets and equipment lifecycles — CANNOT MANDATE The challenge is to provide ALL stakeholders (Federal, state and local), with the right mix of policies, tools, methodologies and guidance Payload routing
The Emergency / Disaster Interoperability Challenge n n n Responders often cannot talk within their own agencies—let alone other agencies — or across cities, counties, and states. Ineffective communications risk the lives of responders in the field, and for those awaiting help. There is no one “Silver Bullet” to solve interoperability challenges. The interoperability landscape consists of 60, 000 state and local public safety agencies, Federal agencies and other stakeholders. 60, 000 agencies means 60, 000 different sets of procurement regulations, budgets and equipment lifecycles — CANNOT MANDATE The challenge is to provide ALL stakeholders (Federal, state and local), with the right mix of policies, tools, methodologies and guidance Payload routing
 EDXL Current and Future n n n You’ve heard about existing OASIS EDXL standards today – Capability exists to support Alerts and warnings, seamless Routing of information, Hospital availability to know where to route patients, and to request, commit, track, status and return Resources. The DE and CAP standards are available through NIEM adaptors today, followed by the other EDXL standards. Moving forward, practitioners have prioritized other standards under development. In particular for Situation Reporting about any incident and its response (Sit. Reps - in OASIS), to track patients (TEP), and expansion of TEP to track all victims of any scale incident (TEV).
EDXL Current and Future n n n You’ve heard about existing OASIS EDXL standards today – Capability exists to support Alerts and warnings, seamless Routing of information, Hospital availability to know where to route patients, and to request, commit, track, status and return Resources. The DE and CAP standards are available through NIEM adaptors today, followed by the other EDXL standards. Moving forward, practitioners have prioritized other standards under development. In particular for Situation Reporting about any incident and its response (Sit. Reps - in OASIS), to track patients (TEP), and expansion of TEP to track all victims of any scale incident (TEV).
 EDXL-Sit. Reps standardizes incident operational picture — information about the") EDXL-Situation Reporting (Sit. Reps) EDXL-Sit. Reps standardizes incident operational picture — information about the situation and cross agency/jurisdiction response — between responders, government officials, coordinating entities and the public.
EDXL-Situation Reporting (Sit. Reps) EDXL-Sit. Reps standardizes incident operational picture — information about the situation and cross agency/jurisdiction response — between responders, government officials, coordinating entities and the public.
 6
6
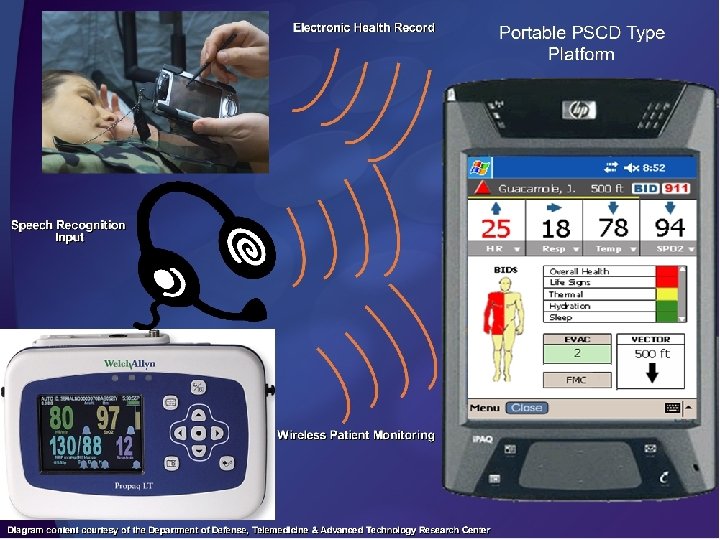
 http: //wam. umd. edu/~mvandani/pda/lowfi 3. html
http: //wam. umd. edu/~mvandani/pda/lowfi 3. html
 10
10
 Mass Casualty Branch Treatment Unit Coordinator Incident Site Priority Red Patients Priority Yellow Patients Morgue Priority Green Patients North Hospital South Hospital Transportation Group Supervisor East Hospital Transport Unit Staging West Hospital Disposition and Medical Communications
Mass Casualty Branch Treatment Unit Coordinator Incident Site Priority Red Patients Priority Yellow Patients Morgue Priority Green Patients North Hospital South Hospital Transportation Group Supervisor East Hospital Transport Unit Staging West Hospital Disposition and Medical Communications
 Treatment Unit Coordinator Incident Site Priority Red Patients Priority Yellow Patients Morgue Priority Green Patients North Hospital South Hospital Transportation Group Supervisor East Hospital Transport Unit Staging West Hospital Disposition and Medical Communications
Treatment Unit Coordinator Incident Site Priority Red Patients Priority Yellow Patients Morgue Priority Green Patients North Hospital South Hospital Transportation Group Supervisor East Hospital Transport Unit Staging West Hospital Disposition and Medical Communications
 Allegany Garrett Cecil Washington Carroll Frederick Harford Baltimore Howard Baltimore City Montgomery Anne Arundel Prince George’s Charl es Kent Queen Anne’s Talbot Calve rt Caroline Dorchester Wicomico St. Mary’s Somerset HAv. BED TRAC 2 ES JPTA Worcester
Allegany Garrett Cecil Washington Carroll Frederick Harford Baltimore Howard Baltimore City Montgomery Anne Arundel Prince George’s Charl es Kent Queen Anne’s Talbot Calve rt Caroline Dorchester Wicomico St. Mary’s Somerset HAv. BED TRAC 2 ES JPTA Worcester
 TEMARR Tennessee Emergency Medical, Awareness, Response and Resources Systems, Governance, Policies and Technologies n n n n Healthcare Beds, Services and Staffing EMS Demographics and Patient Reports Antiviral and Vaccine Distribution Mass Clinic Programs Mass Causality/Victim Management Volunteer Management and Credentialing Alerting and Notification TEMARR
TEMARR Tennessee Emergency Medical, Awareness, Response and Resources Systems, Governance, Policies and Technologies n n n n Healthcare Beds, Services and Staffing EMS Demographics and Patient Reports Antiviral and Vaccine Distribution Mass Clinic Programs Mass Causality/Victim Management Volunteer Management and Credentialing Alerting and Notification TEMARR
 TEMARR n Office of the National Coordinator for Health l Health Information Technology Standards Panel (HITSP) n n n NEMSIS HL 7 DHS and FEMA - Grants and Programs l n Emergency Responder-Electronic Health Record Remote Monitoring CRI, UASI CDC/HHS - Grants and Programs l l Disease Surveillance Situational Reporting National Activities
TEMARR n Office of the National Coordinator for Health l Health Information Technology Standards Panel (HITSP) n n n NEMSIS HL 7 DHS and FEMA - Grants and Programs l n Emergency Responder-Electronic Health Record Remote Monitoring CRI, UASI CDC/HHS - Grants and Programs l l Disease Surveillance Situational Reporting National Activities
 TEMARR n 3 of 5 MSAs Have Patient Tracking Systems l n Heavy Investment The rest of TN without TN TEP and TEV
TEMARR n 3 of 5 MSAs Have Patient Tracking Systems l n Heavy Investment The rest of TN without TN TEP and TEV
 Placeholder: DR. Greg Mears Payload routing
Placeholder: DR. Greg Mears Payload routing
 NEMSIS Brief Overview of NEMSIS n n 2001 Funded by the National Highway Traffic Safety Administration NEMSIS is a standardized approach to EMS patient care data collection and reporting, including: l l A uniform dataset - Data Dictionary XML Schema to ensure portability of data
NEMSIS Brief Overview of NEMSIS n n 2001 Funded by the National Highway Traffic Safety Administration NEMSIS is a standardized approach to EMS patient care data collection and reporting, including: l l A uniform dataset - Data Dictionary XML Schema to ensure portability of data
 NEMSIS
NEMSIS
 NEMSIS Need for NEMSIS n n n EMS Education Standards EMS Performance Measures EMS System Evaluation & Outcomes EMS Research EMS Reimbursement Filling Gaps in Electronic Health Record l Version 3 will be HL 7 based
NEMSIS Need for NEMSIS n n n EMS Education Standards EMS Performance Measures EMS System Evaluation & Outcomes EMS Research EMS Reimbursement Filling Gaps in Electronic Health Record l Version 3 will be HL 7 based
 NEMSIS Dispatch Incident Linkage Medical Device Patient NHTSA 2. 0 Domestic Terrorism Trauma Cardiac Arrest Outcomes Quality Management System Personnel
NEMSIS Dispatch Incident Linkage Medical Device Patient NHTSA 2. 0 Domestic Terrorism Trauma Cardiac Arrest Outcomes Quality Management System Personnel
 www. NEMSIS. org National State Local System NEMSIS
www. NEMSIS. org National State Local System NEMSIS
 National General Population Evacuee and Patient Movement, Regulating and Tracking System Ms. F. Christy Music Program Director, Health and Medical Defense Support of Civil Authorities Office of the Assistant Secretary of Defense (Homeland Defense & Americas’ Security Affairs) October 2009 24
National General Population Evacuee and Patient Movement, Regulating and Tracking System Ms. F. Christy Music Program Director, Health and Medical Defense Support of Civil Authorities Office of the Assistant Secretary of Defense (Homeland Defense & Americas’ Security Affairs) October 2009 24
 Create a National General Population Evacuee & Patient Movement, Regulating, Tracking System Purpose: Build upon existing information systems (military, federal, State, tribal, local, commercial, etc. ) and develop a National General Population and Patient Movement, Regulating and Tracking information system that is interoperable and shares data for mass disaster response and optionally, for routine use. Goal: Federal Sector (Do. D, HHS, DHS, FEMA, DOJ, DOT, etc. ) provide a national system for all jurisdictions’ use. Goal: Use a central IT platform or other technology (inter-operability) to share near real-time data among existing systems and support operational functions of tracking, regulating and movement. Recognized by White House Officials: 2008 Definitions: National, Tracking (Locating), Regulating, Movement 25
Create a National General Population Evacuee & Patient Movement, Regulating, Tracking System Purpose: Build upon existing information systems (military, federal, State, tribal, local, commercial, etc. ) and develop a National General Population and Patient Movement, Regulating and Tracking information system that is interoperable and shares data for mass disaster response and optionally, for routine use. Goal: Federal Sector (Do. D, HHS, DHS, FEMA, DOJ, DOT, etc. ) provide a national system for all jurisdictions’ use. Goal: Use a central IT platform or other technology (inter-operability) to share near real-time data among existing systems and support operational functions of tracking, regulating and movement. Recognized by White House Officials: 2008 Definitions: National, Tracking (Locating), Regulating, Movement 25
 and requested FEMA (via NDMS) funds") National Initiative History Proposed by Do. D (2004) and requested FEMA (via NDMS) funds Noted as DHS Priority (2004) Secretary Ridge’s Homeland Security Interagency Security Planning Effort Included patient mobilization planning for catastrophic events as a long-term initiative and a high-priority (Reference: Secretary, DHS letter to Secretary, Do. D, September 22, 2004). FEMA / HHS funded; Focus: Tracking recommendations, city-based scenario studies, Mass Evacuation Transportation Model, 2005 -2008 AHRQ Project Officer: Dr. Sally Phillips/ Do. D Project Officer: Ms. Christy Music Key Staff: Abt Associates, Mass General Hospital, Brigham and Women’s Hospital National Advisory Board: HSC, Do. D, AHRQ, HHS, DOT, VA, other 26 federal agencies, State (NY and CA), city (New York, Los Angeles) and private
National Initiative History Proposed by Do. D (2004) and requested FEMA (via NDMS) funds Noted as DHS Priority (2004) Secretary Ridge’s Homeland Security Interagency Security Planning Effort Included patient mobilization planning for catastrophic events as a long-term initiative and a high-priority (Reference: Secretary, DHS letter to Secretary, Do. D, September 22, 2004). FEMA / HHS funded; Focus: Tracking recommendations, city-based scenario studies, Mass Evacuation Transportation Model, 2005 -2008 AHRQ Project Officer: Dr. Sally Phillips/ Do. D Project Officer: Ms. Christy Music Key Staff: Abt Associates, Mass General Hospital, Brigham and Women’s Hospital National Advisory Board: HSC, Do. D, AHRQ, HHS, DOT, VA, other 26 federal agencies, State (NY and CA), city (New York, Los Angeles) and private
 National Initiative AHRQ Webcast: February 9, 2009 Final Report Released") National Initiative History (continued) National Initiative AHRQ Webcast: February 9, 2009 Final Report Released by AHRQ: February 24, 2009: “Recommendations for a National Mass Patient and Evacuee Movement, Regulating, and Tracking System” Report is located at http: //www. ahrq. gov/prep 27
National Initiative History (continued) National Initiative AHRQ Webcast: February 9, 2009 Final Report Released by AHRQ: February 24, 2009: “Recommendations for a National Mass Patient and Evacuee Movement, Regulating, and Tracking System” Report is located at http: //www. ahrq. gov/prep 27
 Focus on Multi-Jurisdictional Incidents and Operational Functions Incident Area Evacuee Gathering Points Incident Site Casualty Collection Points Hospitals Shelters Hospitals Out-of-State Receiving Areas Shelters Airfields In-State Receiving Areas 28
Focus on Multi-Jurisdictional Incidents and Operational Functions Incident Area Evacuee Gathering Points Incident Site Casualty Collection Points Hospitals Shelters Hospitals Out-of-State Receiving Areas Shelters Airfields In-State Receiving Areas 28
 Sample Questions the System Could Answer The Public: Where is my loved one? I will register to tell my family where I am. Incident Commanders: How many victims are there? Where are they? Where are more response assets needed? Emergency Operations Centers: How many patients and general population evacuees exist? Where is there unused capacity? Will I need outside assistance? Federal Operations Centers: What federal transportation, medical and other assets, will be needed to supplement local and state assets to transport patients and general population evacuees? How many buses or planes are available? How many and what type of special needs general population evacuees, and medical special needs patients, need to be evacuated? Where are the available, staffed and equipped hospital beds with appropriate care for patients? Emergency Managers: Who exactly is coming on that plane of general population evacuees and/or patients? Who are the attendants? How many service animals/pets are there? Public Health Department / Relief Organizations: How many people are in 29 shelters and what are their specific needs?
Sample Questions the System Could Answer The Public: Where is my loved one? I will register to tell my family where I am. Incident Commanders: How many victims are there? Where are they? Where are more response assets needed? Emergency Operations Centers: How many patients and general population evacuees exist? Where is there unused capacity? Will I need outside assistance? Federal Operations Centers: What federal transportation, medical and other assets, will be needed to supplement local and state assets to transport patients and general population evacuees? How many buses or planes are available? How many and what type of special needs general population evacuees, and medical special needs patients, need to be evacuated? Where are the available, staffed and equipped hospital beds with appropriate care for patients? Emergency Managers: Who exactly is coming on that plane of general population evacuees and/or patients? Who are the attendants? How many service animals/pets are there? Public Health Department / Relief Organizations: How many people are in 29 shelters and what are their specific needs?
 National Mass Patient and Evacuee Movement, Regulating and Tracking Initiative National Advisory Board Recommendations: Must build on existing systems (federal, State, local, tribal, private industry) Must incorporate general population and patient evacuees Must track and give notice of general population members as they become patients Incorporate data and architectural standards Maintain HIPPA compliance, as well as other regulatory requirements Activated system – during major, multi-jurisdictional incident Optional routine use Begin with local, State and tribal entry, Federal entry last 30
National Mass Patient and Evacuee Movement, Regulating and Tracking Initiative National Advisory Board Recommendations: Must build on existing systems (federal, State, local, tribal, private industry) Must incorporate general population and patient evacuees Must track and give notice of general population members as they become patients Incorporate data and architectural standards Maintain HIPPA compliance, as well as other regulatory requirements Activated system – during major, multi-jurisdictional incident Optional routine use Begin with local, State and tribal entry, Federal entry last 30
 Data from") National Mass Patient and Evacuee Movement, Regulating and Tracking Initiative Recommendations (continued) Data from point of injury or first entry into the system, through intermediate locations, through final disposition – location and audit trail Track location & health status/ needs of any person encountering system Track at “touch points” (e. g. evacuation centers, overnight facilities, patient collection or staging areas, vehicle loading/unloading, hospitals, shelters, etc. ) Incorporate current or planned Feeder Tracking Systems Jurisdictional, commercial, and agency specific systems Incorporate Feeder Institutional Records Systems (“Check-In/Check Out” Systems) Facilities with mandatory reporting, common software platforms, within an agency (e. g. VA hospitals, Do. D Military Treatment Facilities, Indian Health, etc. ) Single facility (nursing home with “homegrown” system) 31
National Mass Patient and Evacuee Movement, Regulating and Tracking Initiative Recommendations (continued) Data from point of injury or first entry into the system, through intermediate locations, through final disposition – location and audit trail Track location & health status/ needs of any person encountering system Track at “touch points” (e. g. evacuation centers, overnight facilities, patient collection or staging areas, vehicle loading/unloading, hospitals, shelters, etc. ) Incorporate current or planned Feeder Tracking Systems Jurisdictional, commercial, and agency specific systems Incorporate Feeder Institutional Records Systems (“Check-In/Check Out” Systems) Facilities with mandatory reporting, common software platforms, within an agency (e. g. VA hospitals, Do. D Military Treatment Facilities, Indian Health, etc. ) Single facility (nursing home with “homegrown” system) 31
 Minimum data") National Mass Patient and Evacuee Movement, Regulating and Tracking Initiative Recommendations (continued) Minimum data elements to enter patient/general population evacuee data Unique identifier (a universal algorithm for assigning IDs would be ideal) Name, gender, DOB (if not available, substitute age range, race and notable physical characteristics to help identify the person) Health Status Red, yellow, or green triage color ICU, floor, or discharge ready/not Acutely ill, well with medical history (needing medical attention), healthy Last updated location (ID /name/ type), date, time Build system to accept more detailed demographic and medical information Build from person-level data, but accept aggregate (location-level) data 32
National Mass Patient and Evacuee Movement, Regulating and Tracking Initiative Recommendations (continued) Minimum data elements to enter patient/general population evacuee data Unique identifier (a universal algorithm for assigning IDs would be ideal) Name, gender, DOB (if not available, substitute age range, race and notable physical characteristics to help identify the person) Health Status Red, yellow, or green triage color ICU, floor, or discharge ready/not Acutely ill, well with medical history (needing medical attention), healthy Last updated location (ID /name/ type), date, time Build system to accept more detailed demographic and medical information Build from person-level data, but accept aggregate (location-level) data 32
 Include near") National Mass Patient and Evacuee Movement, Regulating and Tracking Initiative Recommendations (continued) Include near real-time regulating and movement data and functions – Match/ reserve available resources to requirements, release resources, track diverted resources Example: Reserve ACLS/ATLS ambulance/crew & ICU hospital bed with critical patient Example: Release bus and shelter beds after general population evacuees have left System accessible to emergency responders, planners, authorized users Eventually include public: web- based registration Free for public, local, State, tribal use – more coordinated, rapid response Use technology for easy use and interoperability (e. g. scan ID number, web-based, satellite transmission, drivers license, passport, central IT platform, open architecture, etc. ), and manual entry 33
National Mass Patient and Evacuee Movement, Regulating and Tracking Initiative Recommendations (continued) Include near real-time regulating and movement data and functions – Match/ reserve available resources to requirements, release resources, track diverted resources Example: Reserve ACLS/ATLS ambulance/crew & ICU hospital bed with critical patient Example: Release bus and shelter beds after general population evacuees have left System accessible to emergency responders, planners, authorized users Eventually include public: web- based registration Free for public, local, State, tribal use – more coordinated, rapid response Use technology for easy use and interoperability (e. g. scan ID number, web-based, satellite transmission, drivers license, passport, central IT platform, open architecture, etc. ), and manual entry 33
 Contact Information: F. Christy Music: francesca. music@osd. mil 703 697 -5839 Sally Phillips: Sally. Phillips@ahrq. hhs. gov 301 -427 -1571 34
Contact Information: F. Christy Music: francesca. music@osd. mil 703 697 -5839 Sally Phillips: Sally. Phillips@ahrq. hhs. gov 301 -427 -1571 34