8dcc38ad80bf32c2aa892db9d3d02300.ppt
- Количество слайдов: 193



WORKFLOW-2007



Objections to Flight vs Digital • I am not a flyer • It weighs to much • I can crash and burn • I could never learn those controls • It will get in the way of my walking • I am not a computer type person • It costs to much • I can crash and burn • I could never type • It will get in the way of my patients

Process • Not all will be happy-10 -15% love island will not move • It will be painful at times • We are all in this together • -Basic computer skills-typing – 15 dollars for typing program • Failure and non-participation is not optional • We have clear goals and excellent technical support

Biggest Obstacle to Speed and adapting digital methods It Requires a Paradigm shift

4 FACTORS THE JEDI INCIRCLE ACCESS FOR PATIENTS INCLUDES SATISFACTION SENSE OF BEING CARED DECREASED COSTS HAPPIER PROVIDERS IMPROVED QUALTITY OF CARE

WE NEED TO KNOW THE ENEMY Anytime you see paper, it is a sign of inefficiency

PAPER • MANUAL LABOR-$$$$$ • AUTOMATED LABOR • PRIMARY CARE LOW MARGIN • DO WE HAVE A MARGIN FOR OUR MISSION?

Cost of Doing Nothing Paper Cost Time Compliments Dan Russler, Mc. Kesson

Cost of Parallel Systems – Paper and EMR Paper EMR Cost Time Compliments Dan Russler, Mc. Kesson

Do you feel like a peasant? “We are at the mercy of Chevera… Government, Insurance companies, Regulators, Politicians, EMR

Does this sound like the doctor’s lounge?



Going to the Mountains

Magnificent 7 Basic Concepts of Workflow

The Magnificent 7 1. 2. 3. 4. 5. 6. 7. Computers don’t improve anything Productivity is how you use the computer Deep change hurts - Kakushin Continuous improvement helps - Kaizen Workflow is hard work - Keep at it Empower the Patient – Ease the burden Finish it – Enjoy it

Concept 1 - Computers don’t improve anything • Understand the Productivity Paradox • Automation may not fix bottle necks • Your EMR is not the gold mine -YOU are

y


If you have a mess and computerize it You end up with a computerized mess

Concept 2 Productivity is how the computer is used it is the same all over


Viewers • Paper in an electronic environment • Chart can be in several places • Productivity none • Minimal Interaction

Basic Users • • • Interaction is limited Dictation is used Ordering Past medication No large productivity gains

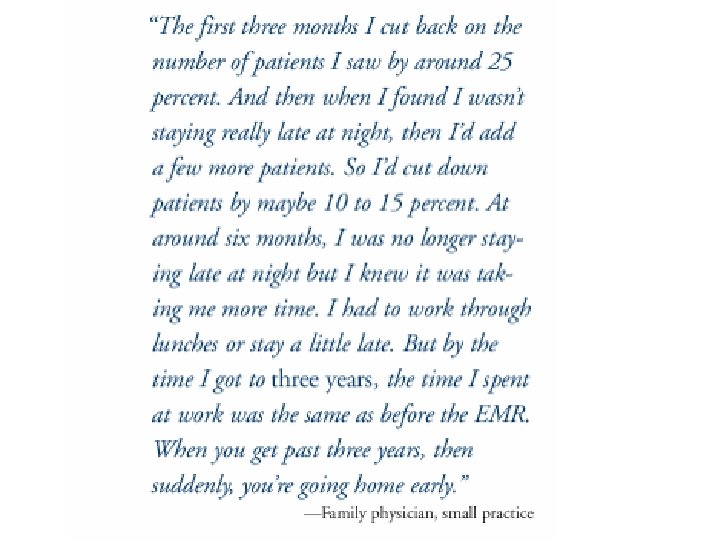
Strivers • Use Templates to enter information • Early in program first 1 -2 years • More efficient • Replacing transcription but spending time on machine

Arrivers • A lot of time invested and now not needed • Extremely good at their systems • Reaping productivity gains

System Changers • Maximum Productivity • Incorporate addons and workflow changes • Bend it to their will

Concept 3 Workflow change depends on deep change - Kakushin 革新

Kakushin A Deep Change revolutionary change or radical improvement Everything will be different Think in the Future


Mechanical Swiss Watch

Kakushin = 革新 which means innovation You make a large investment in a new direction Some people revolutionary change Transition Efficiency

Luxury Auto • Mercedes Benz Quality investment value sturdy • BMW Style, handling, functional • Audi Style, space, affordable • Volvo Safe, Reliable, Quality • Jaguar Attractive • Toyota cheap dependable

Bottom Line • • • Status and Prestige High Quality Resale Value Performance Safety

Build the Car but different • Great handling but a pleasant ride • Fast and smooth but a low fuel consumption • Super quiet but light • Elegant styling but aerodynamic • Warm but functional • Great Stability and yet low friction

First Year • Sold 2. 7 times more Lexus the Mercedes Benz the leader

EMR • Improve Quality but decrease costs • Improve Documentation but have more time with patients • Improve access for patients but leave for home at 5 • Increase R and D but improve margins

Concept 4 Continuous improvement Kaizen 改善

Kaizen • Incremental continuous quality improvement • You get a little better each day • Limited by technology • Significant Limitation

The Toyota Way. Measure Everything

Process map patient care

Time- from Drucker’s The Effective Executive The Supply of Time is totally inelastic. No matter how high the demand, the supply will never go up. There is no price for it and no marginal utility curve for it. Moreover, time is totally perishable and can not be stored. Yesterday’s time is gone forever and will never come back. Time is, therefore, is always in short supply. Time is totally irreplaceable… There is no substitute for TIME
……. . NOT")
The Toyota Way Look for what is valuable to the customer (patient)……. . NOT what you may value

Waste • Not safe 50000 -100000 deaths due to errors • 42% respondents experience poor or inefficient care • 45% recommended care not given (not insurance related) • ¾ of US population wants change • 47 million uninsured

Workflow to find waste • Overproduction • “Seeing someone • Waiting who you should nothospital rounds • Patient Staff • Unnecessary transport • Over processing or incorrect processing • Movement back and forth • Prescription in pt with allergy

Workflow to find waste • Excess inventory • Prescription refills • Unnecessary movement • Clickitis • Defects • Pt left without needed shot • I am the boss • Unused employee creativity

Patient Perspective Patient Arrives Start Checks In and Waits Room Nurse Wait Doctor sees Gets Tests Gets Rx Waits For Does tests Plan For Rx Done

Workflow Digital and Not Digital Concept 5 Workflow You can not go Back-Lower the ODDS


Let’s Lower the Odds Let’s Go to the Office….

First Step – Patient comes to Clinic


Patient Value to See You Decides to come Phone Call 9 pm Give Information Remember Get in Car Go to Office 68 minutes for 6 minute office visit

Did they need to come? To pay a bill Pick up something
 • Low margin")
Physician View of Patient (who did not need to see me) • Low margin revenue – Exchange of data – Rechecks – Patient who does not need to be there – Could someone else do it? • Non-visit care tomorrow (e-Visits) • Work smarter – not harder

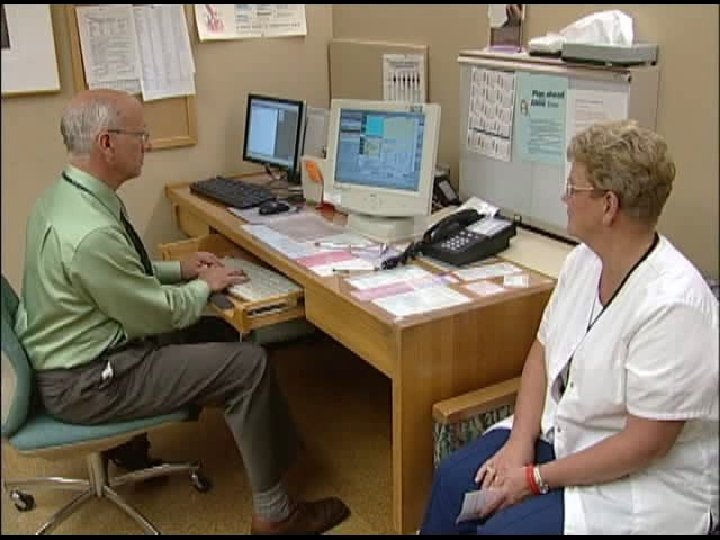
Patient comes to a receptionist Think about your office


Waste? • Efficient • Paper there Did we need it? How did it get there? • Looked in computer Phoned

WASTE

Patient Enters the Clinic

VALUE Pt coming to Office Patient Registering WASTE

Lobby Waiting • 19/20 were waiting one filling form

VALUE Pt coming to Office Patient Registering Patient in lobby WASTE


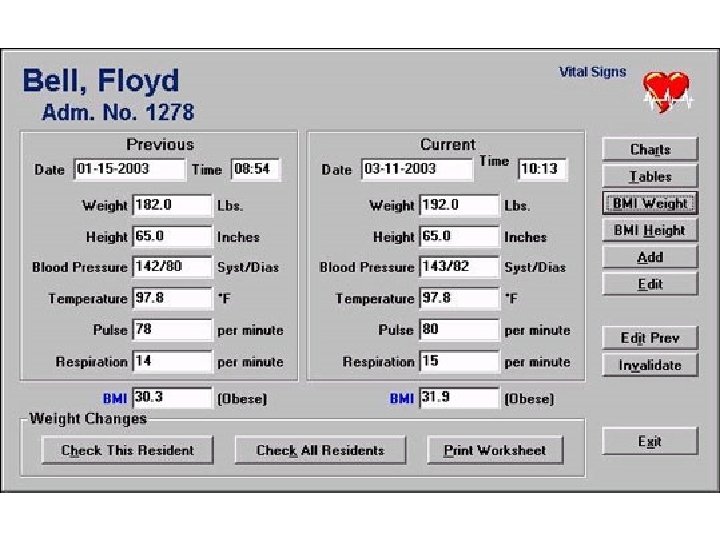
Vital Signs

Vital Signs WASTE Accurate? Paper? Time to Log in? VALUE BP/Pulse/Weight 60 seconds

VALUE VS Pt coming to Office Patient Registering Patient in lobby WASTE


Vital Signs pulse BP • . . Movies 2006MVI_2995. AVI



Patient waits for doctor

VS Pt coming to Office Patient Registering Patient in lobby Waiting for Doctor

Doctor needs to know you are ready

NOW THE DOCTOR ARRIVES

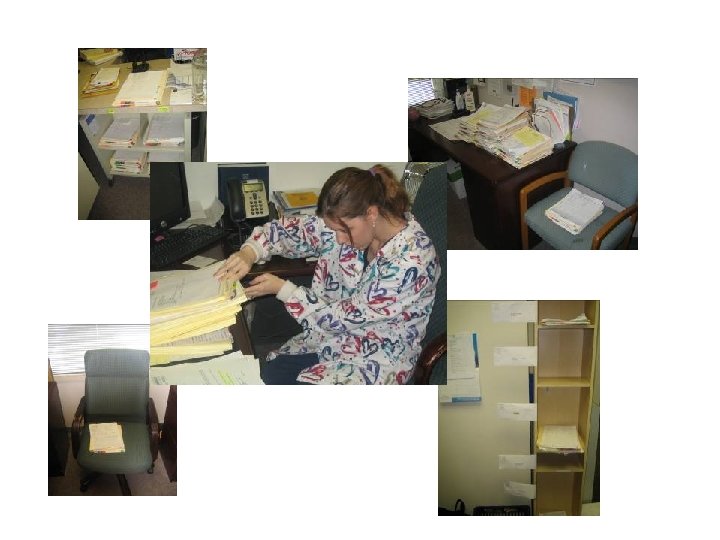
Doctor does the writing Doctor does the data entry

MD Documenting – IS IT WASTE OR IS IT VALUE Hand Writing Typing Dictatin g Editing 30 words per minute 60 words per minute 180 words per minute 7200 words per minute $$$$$$ $$$$$$ $

Options for Data Entry to EMR 1. 2. 3. 4. 5. 6. Handwriting recognition Typing Dictation Voice recognition Templates Patient entered data with editing

1. Doctor using Handwriting Recognition Slow, but seems great until have more than 6 words or misrecognition occurs

EMR and 15 Minute Office Visit Doctor Handwriting Checkout Physician Documentation Check-in Vitals Doctor for Data Entry Handwriting or Handwriting Recognition 1 2 Escort 5 12 4 Physician Exam = $32 1 Escort Nursing Documentation Making Money Wasting Money Spent Graphic derived from Dan Russler, MD, Mc. Kesson,

Doctor Does the Data Entry

Productivity Drop with EMR Time of Office Visit Kaiser Northwest, Portland, OR

Revenue Drop after EHR Carilion Health Care – Roanoke, VA

Where did they put the Computers?

EMR and the 15 Minute OV Doctor Typing Using the Doctor for Data Entry Checkout Check-in Vitals 3 1 2 Escort 4 12 Physician Exam Nursing Documentation Making Money Wasting Money Spent 8 1 2 = $42 Escort

We could have nursing do this What would that look like?

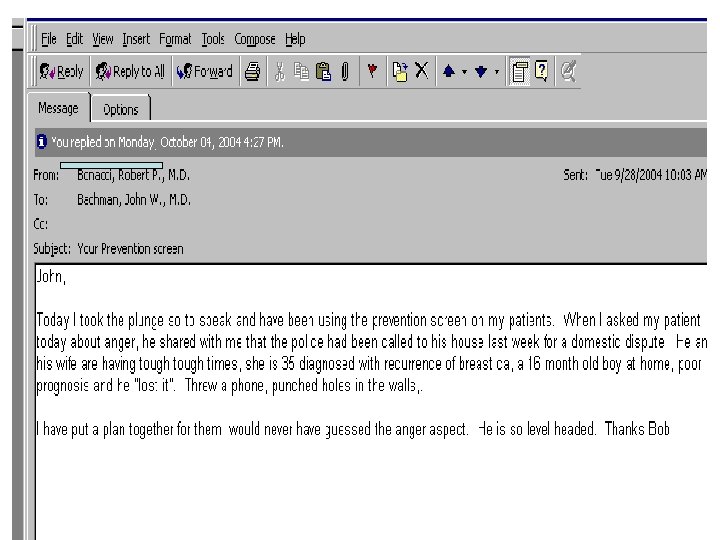
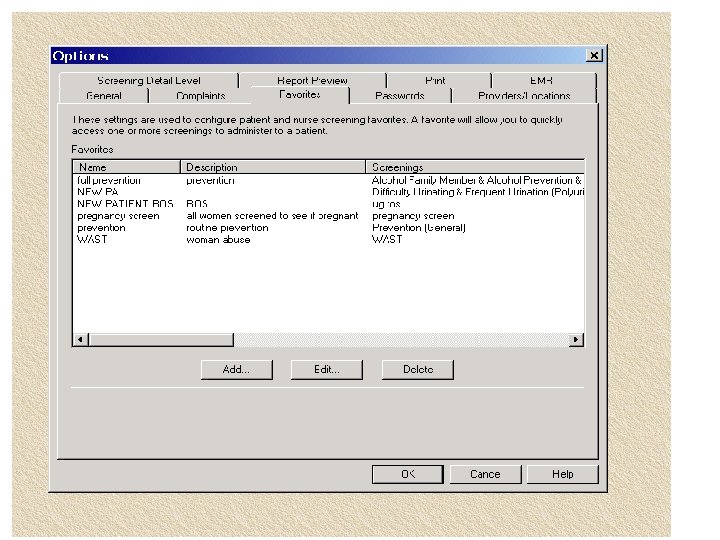
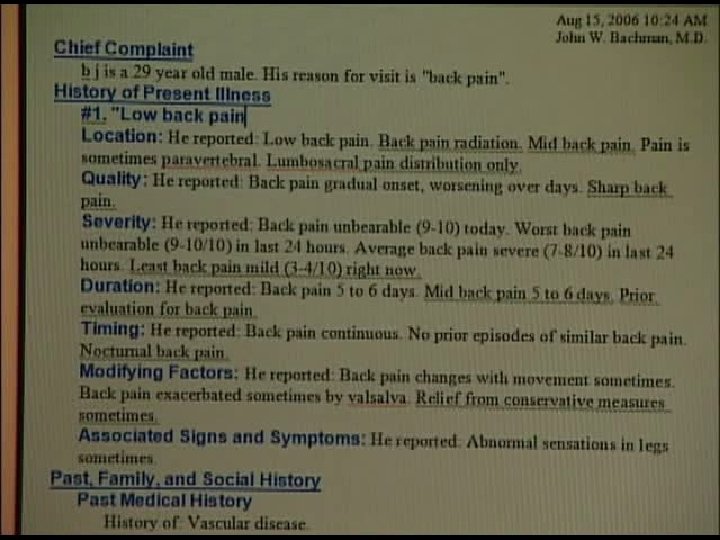
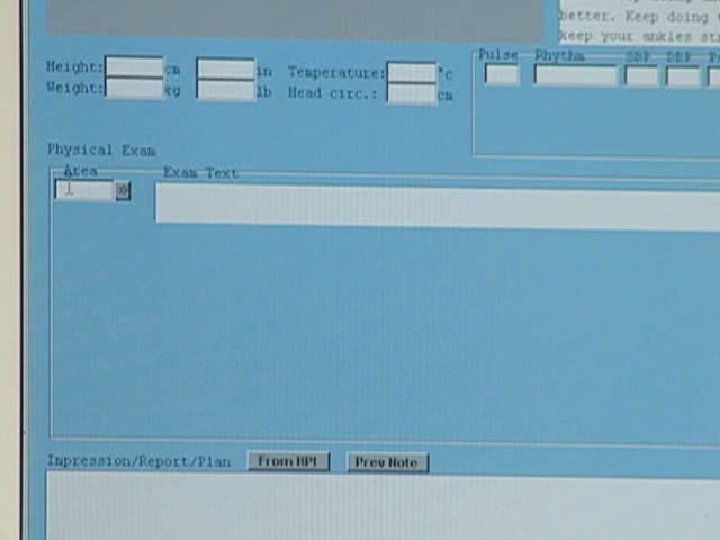
Data Entry into a Field-Prevention

PREVENTION REVIEW This review was done when the adult was 55 years old on Thursday, October 14, 2004. We have discussed the following topics which are important for all people in your age group: cholesterols every five years (see past medical history for your value), smoking habits (can be found in past medical history), alcohol use, abstinence, and being in a car with a driver who has been drinking, recreational drugs, aspirin should be taken daily , sexual practices, Prostate check yearly: last exam 2004 and offered counseling. The following should be done yearly: height, weight, and blood pressure: done this year Injury prevention is as follows: seatbelts: yes Smoke detectors: yes Bicycle and motorcycle helmet does not bike Guns and violence: no gun in home Other risk factors reviewed: passive smoke: not at risk Exposure to tuberculosis: yes-(you are at risk and need a TUBERCULIN TEST YEARLY) Sunscreens: no-(you should WEAR SUNSCREENS 15 OR ABOVE) Radiation to neck no Have a family history of colon cancer, familial polyposis: no Colonoscopy or alternative examination recommended after age 50 colonoscopy 2004 Risk for back problems: not at risk Brushing teeth and dental care: yes Exposure to loud noises: not exposed You are at risk for diabetes: no risk Your risk for cancer is related to these relatives: none. You have had a divorce in your family or separation, felt sad or are grieving: no You are angry or are frequently angry: YES Your shots are up to date: yes and can be found in past medical history. We recommend all families know CPR. REVIEW OF SYSTEMS:

The EMR and the 12 Minute Office Visit Nurse for Documentation Using the Doctor for Data Entry 1 4 2 Checkout Physician Dictating Check-in Vitals 3 12 Physician Exam Escort = $42 1 Escort Nursing Documentation Nurse for Data Entry 18% Reduction Labor Cost Physician Checkout Check-in Nursing Documentation Vitals Documentation 1 2 Escort 12 12 Physician Exam 2 1 Escort = $32

We can dictate

EMR and the 15 Minute Office Visit Doctor Dictating Doctor for Data Entry Dictation Physician Dictation Check-in Vitals 3 1 2 4 12 Escort Checkout 1 2 1 3 Wasting Money Spent = $38 Escort Physician Exam Nursing Documentation 4 Transcription cost Staff management of dictation Making Money 2 ? Decreased patient safety & satisfaction 10 Inability to answer problems Poor referral management Insurance rejection issues

Cost Comparison of EHR Data-Entry Workflows • Physician 1 2 6 • Nurse 1 2 12 • Patient 12 12 1 2 3 1 10 12 4 4 = $42 1 = $37 1 = $29 Where is the WASTE? Where is the VALUE?

What are we doing in the exam room? WASTE vs VALUE 1. 2. 3. 4. History Physical Exam Plan Write Prescriptions


Who is the owner of a person’s health? Who is the customer?

Instructions • 40% lost in minute • 80% lost in 30 minutes • Incorrectly remembered » J Royal Soc Med 2003 96: 219 -222

Information 71% of time patients are given nothing following their visit 68% of patients of Mayo Internists did not report what physician thought was a problem 54% a major problem

Concept 6 Empower the Patient



You are at the office • A partner’s patient who has hypertension comes to see you because in the last ten days she has noted that her blood pressure is elevated from its baseline. • Meds Lisinopril 20 mg daily • BP 152/93
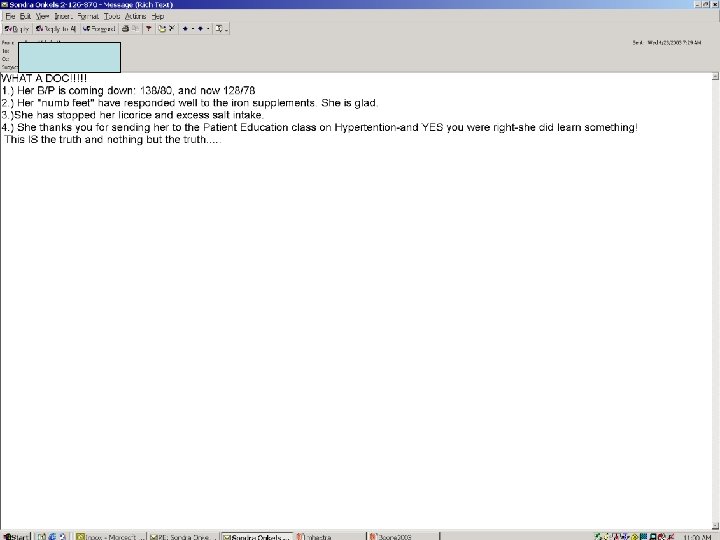

What did we learn? • We can not judge quality of care by reviewing a chart! • Inputs are important • Computerized history provided more information that was critical to this case, and was valuable to the clinician

Vendors • The literature has been around forty years • Without an EMR not all that practical • Names are in the handout-None are here except one
 • Software program you buy 50 dollars a month from")
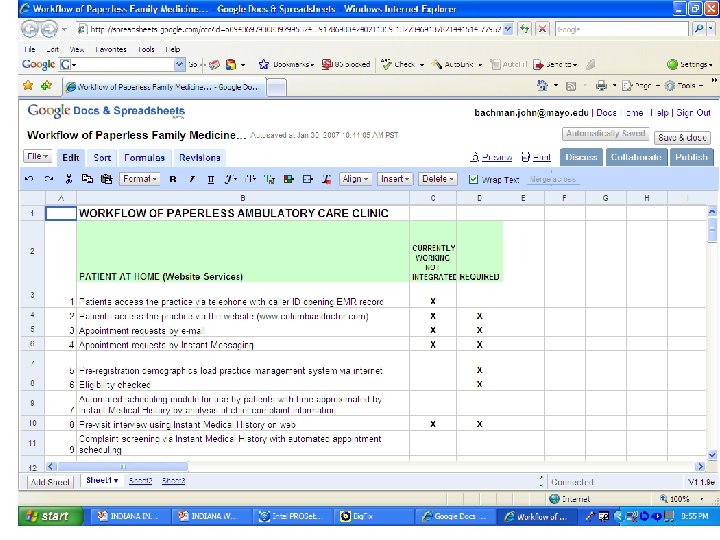
Instant Medical History (IMH) • Software program you buy 50 dollars a month from Primetime Practice • 75000 questions • Install into a computer • Tool on e-mail/internet for patients to use. Medfusion AAFPs portal • 45 EMRs have as the interface to patient-This is huge www. medicalhistory. com

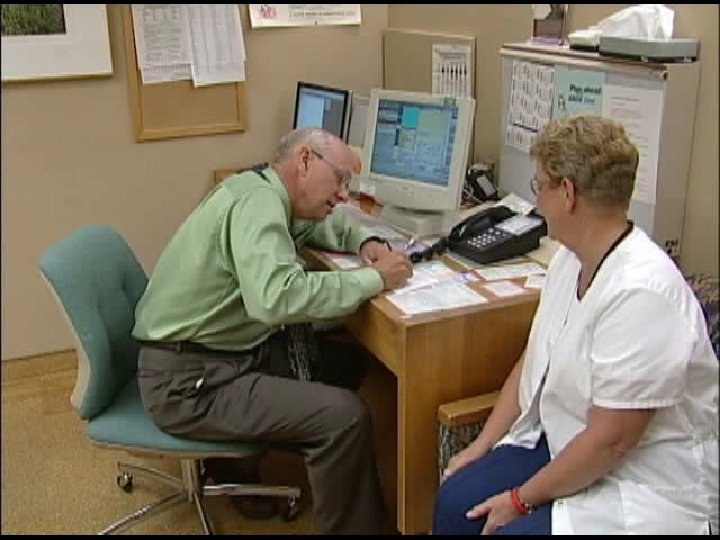
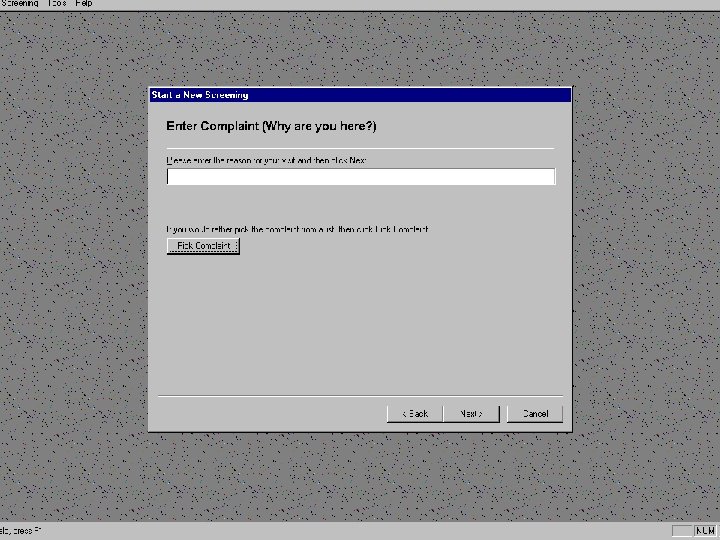
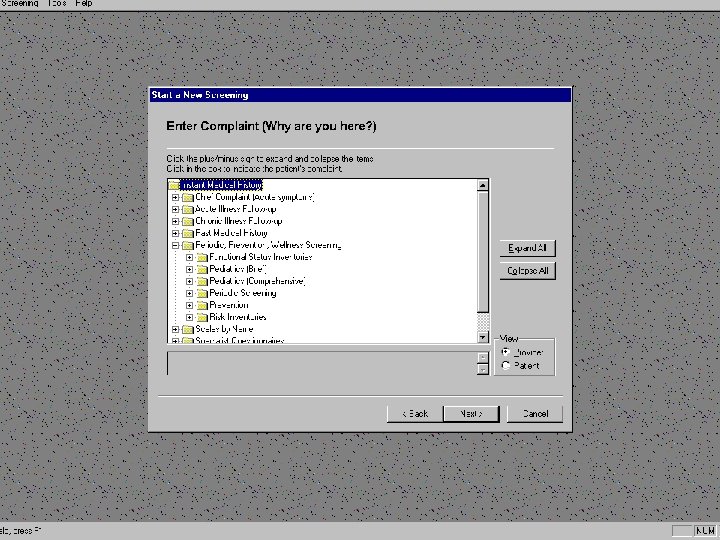
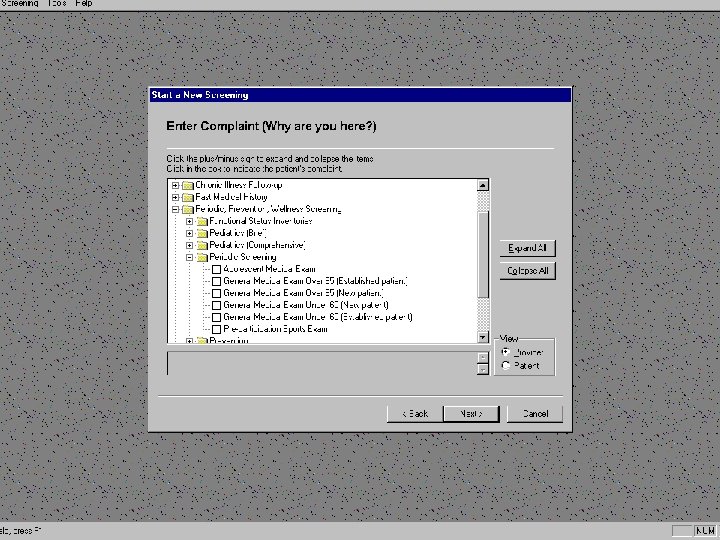
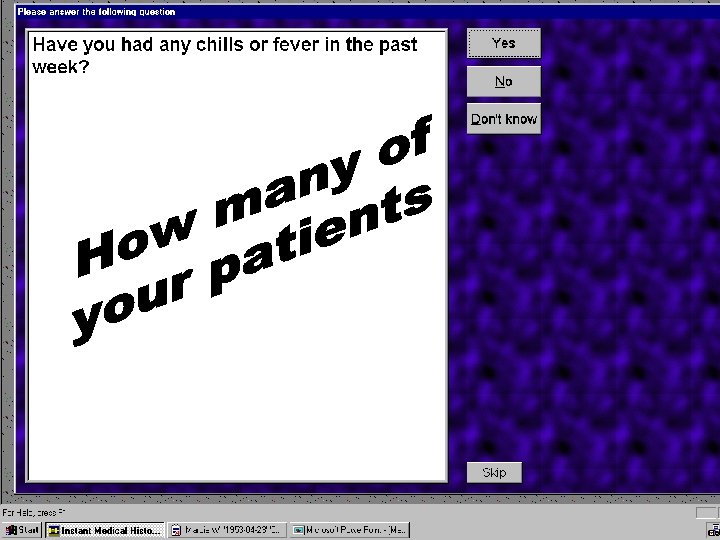
How does it work?

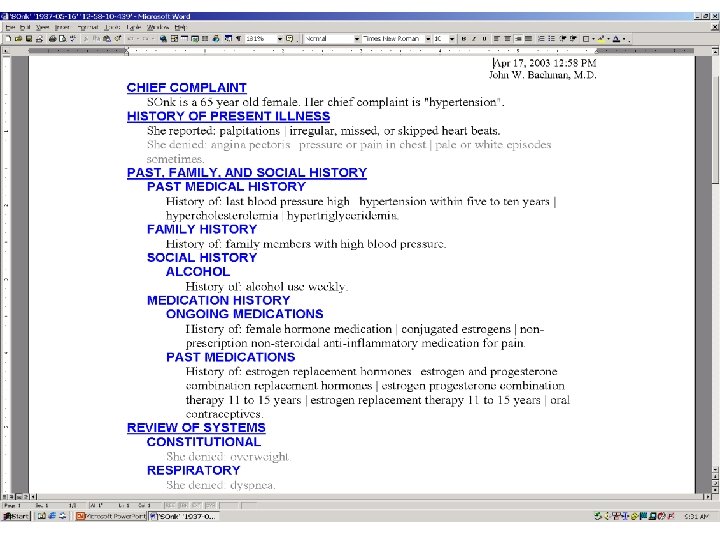
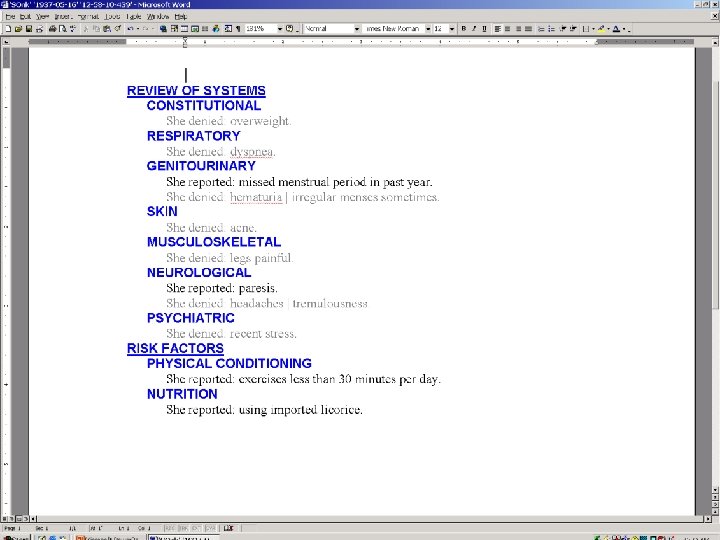
Patient Doing History

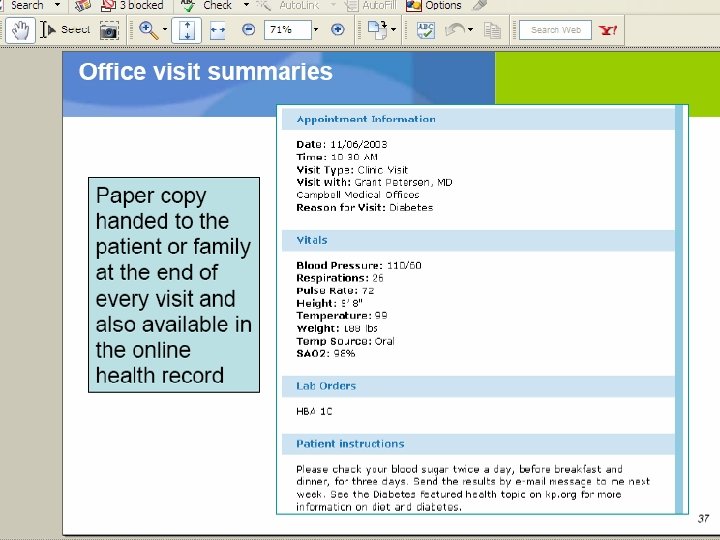
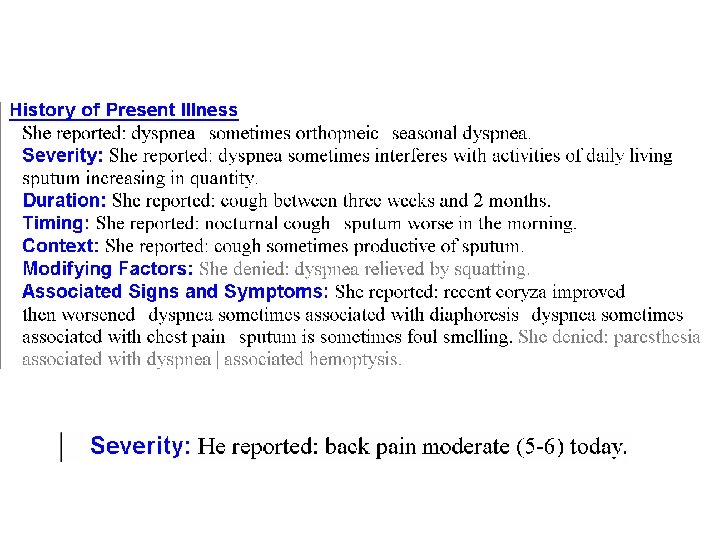
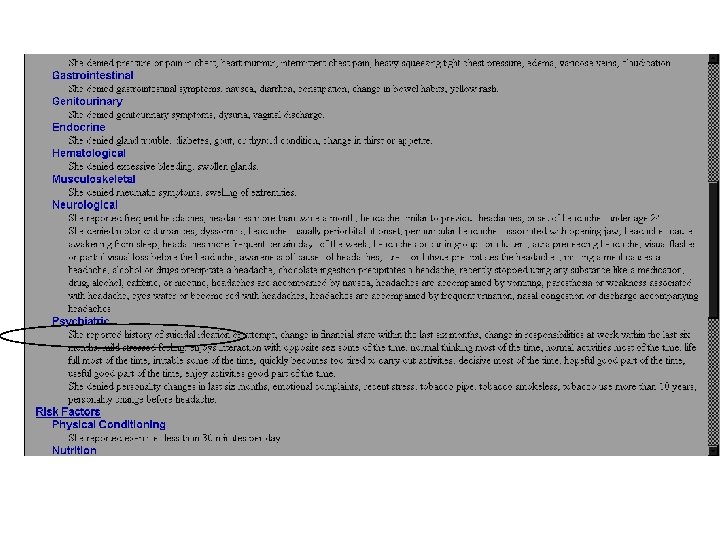
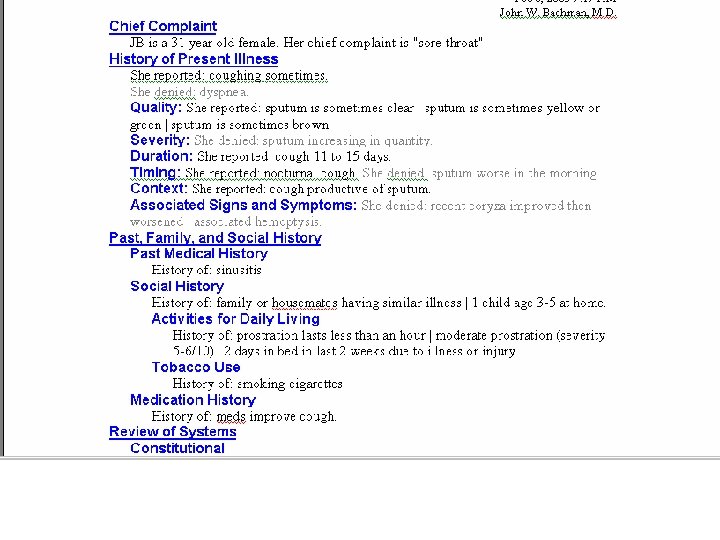
OUTPUT IS GIVEN TO YOU • Given to you on paper • Given to you in electronic form like into Word • Directly into an EMR

ADVANTAGES Collects more data then a clinician and organizes it into a readable form

Patient is better organized Patients can do this

Patient collects information that the clinician misses • 40% of time provided useful information not typically elicited • Essential Questions missed • Pilot’s Checklist
 Deaths")
How dangerous is health care? Note: both dimensions are logarithmic scales DANGEROUS (>1/1000) Deaths per year Health Care REGULATED ULTRA-SAFE (<1/100 K) Driving 10, 000 100 Mountain Climbing 10 Bungee Jumping 10 Scheduled Airlines Chartered Flights European Railroads Nuclear Power Manufacturing 10, 000 Number of encounters per death 100, 000 1, 000 10, 000

Socially Sensitive

Highly Adaptable SARS

Documentation • Most Clinicians do E 4 work 55904 • Most Clinicians Code E 3 work 55903 • Most Clinicians document E 2 work. 55902

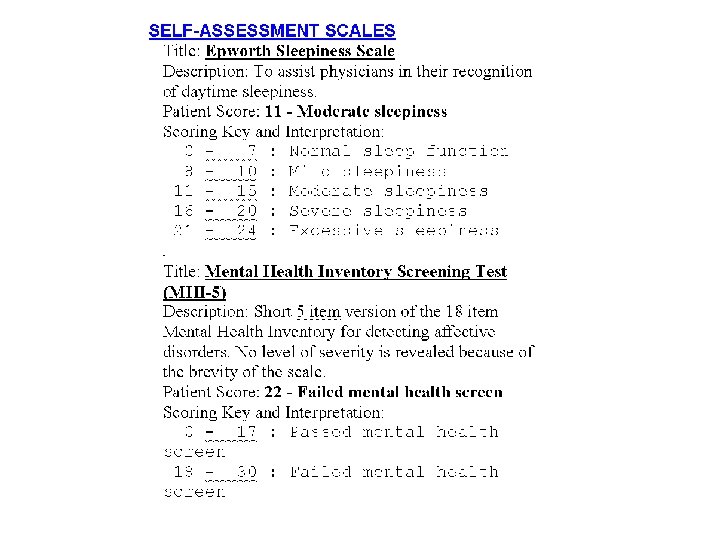
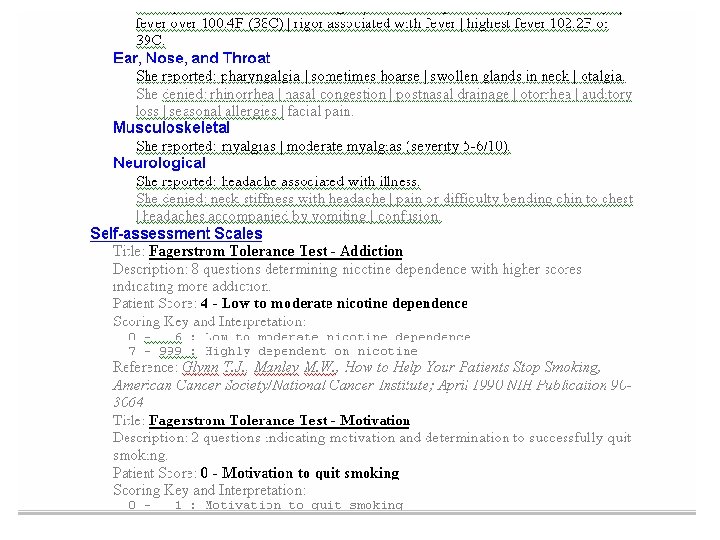
Others • • • Patient controls interview-length of time Doctor only deals with positives Research Multimedia High patient acceptance Scales

Scales • • Zung Depression Rahe Stress Scale Urology Scales Wast Conners Anxiety Pain impairment Patient Education Needs

Tough Diagnosis

Time of a Routine Office Visit Plan Subj. Obj. Pat Ed

Future Time of a Routine Office Visit Subj. Plan Obj. Pt. Ed

Complete Physical Subj Extra Time Obj Plan Subj Obj

Jane Doe Chief Complaint Sore throat VS stable Sore throat 3 days duration

Lets look at history 80/20 Rule 20% of your questions get you 80% of the content Negatives are time intensive Analogy Mining for Diamonds!

Mining-Topsoil sand it is easy Open ended questions Listening 2 minutes

What are the results of All this labor

It is like Mining Yes/No questioning-tailings

You can use a machine to Do the hard time consuming Work

You are in control You will trust the work done Check out a few things


A Clinic Story They see it and own it • History was done on 5 page paper form, then translated into EMR • Patients often forgot to bring form • Office staff could see pt. on same or next day basis • “Insurance problems” was common barrier to early. OB care

A Clinic Story PLAN: Change workflow, add IMH Call for Visit Wait 1 -2 Weeks Come in Today or Tomorrow for Intake Send History Form in Mail Initial New OB Visit Insurance Forms Video MD Visit History reviewed (or re-collected if pt. forgot questionnaire) Exam Prenatal Labs ordered, pt. sent to lab Rx Vitamins Plan/Discussion Intake Visit IMH Rx Vitamins Insurance Forms Video Prenatal Labs drawn in office MD Visit – 1 -2 wks later History reviewed Exam Plan/Discussion

A Clinic Story RESULTS in FPC PRE: NO Show rate: 40% MD Time: 1 hr/pt Indicators: missing POST: 11% 45 min/ pt all met

You have the Subjective Portion • Answers to a series of yes and no questions • Minor alterations • Documentation has improved • Quality has improved– Pilot check list – More complete inventory – ATMs and electronic tickets • Computer has had structured data entry



Impression and Plan • Using the Internet for plan if you do not have a template


Concept 7 – Finish IT, Enjoy IT Go home at 5 PM with work done!

Go get em


References • Bush Roger W Reducing Waste in US Health Care Systems JAMA 2007 297 871 -874.
8dcc38ad80bf32c2aa892db9d3d02300.ppt