21a0163f4fdf5bb5bc4e4e0890656b78.ppt
- Количество слайдов: 75



“What empiric antifungal antibiotic would you use for meningitis? ” UNC Wednesday Conference Case #1 Kees van Dam

HPI Ø 25 yo Caucasian female with history of severe Cystic Fibrosis underwent a double lung transplant on 1/10/07. Ø On 1/11/07 she underwent evacuation of a left sided hemothorax as well as takedown and revision of the left pulmonary artery anastomosis.

HPI Ø Post-operative course further complicated by episode of asystole after central line placement (sp) resuscitation. Ø Renal failure thought to be due to tacrolimus. Patient had been on CVVHD since 12307.

HPI Ø She was difficult to “wean” from ventilator but on 2/5/07 was successfully extubated. Ø She had been on TPN during this time. Ø She has required epogen for anemia and has had several blood transfusions, most recently on 2/8/07

HPI Ø During the night of the 9 th, an RN was drawing blood from the patient who appeared confused and asked RN what she was doing. Patient then began staring into space and gasping for breath. She was given narcan for possible dilaudid OD. She had twitching all over for a few hours. She was intubated. Neurology called, MRI of brain performed.
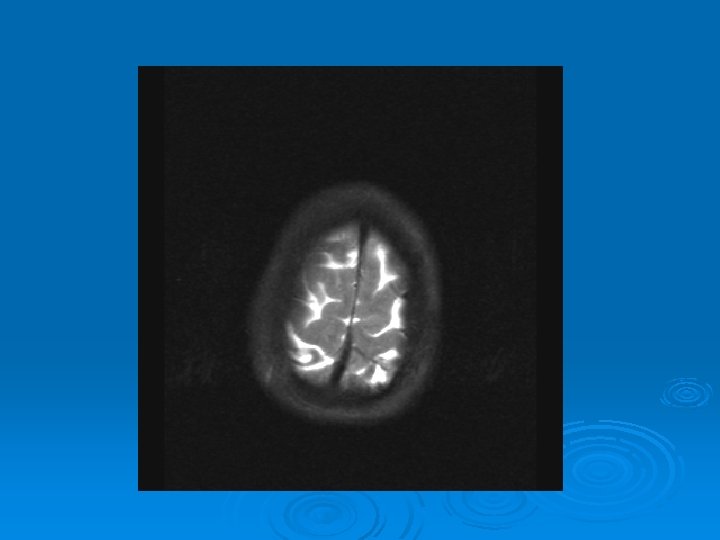
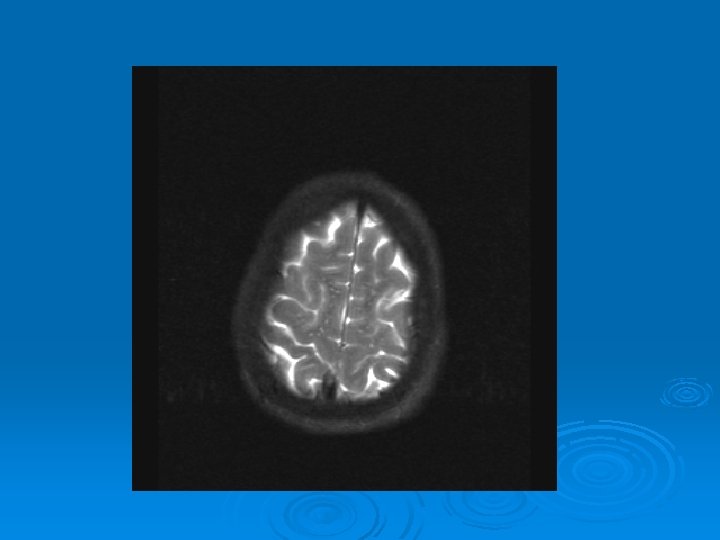
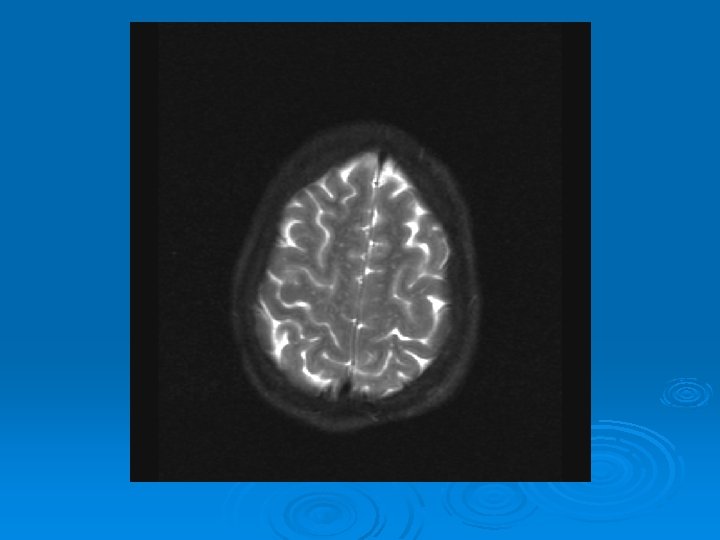
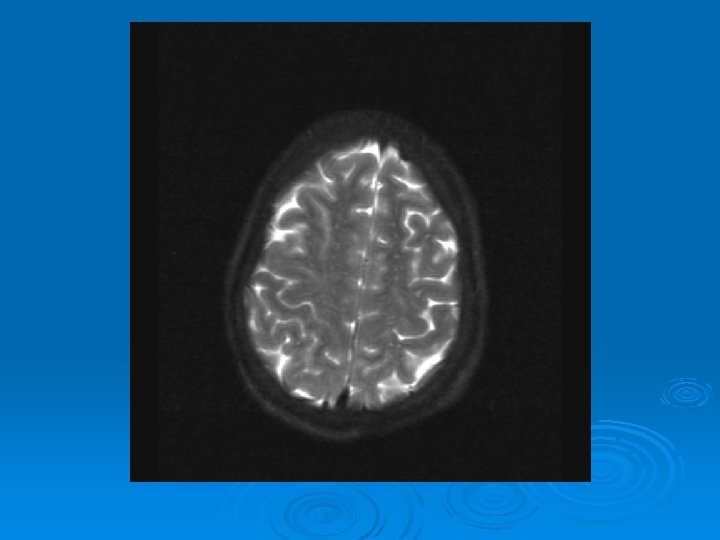
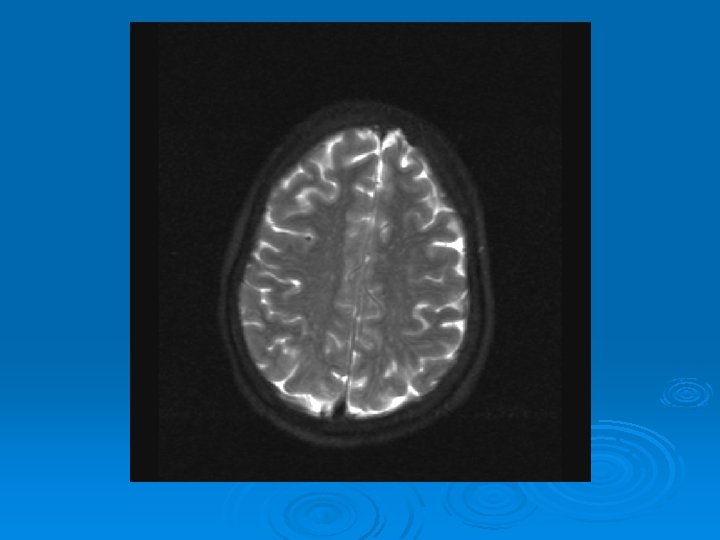
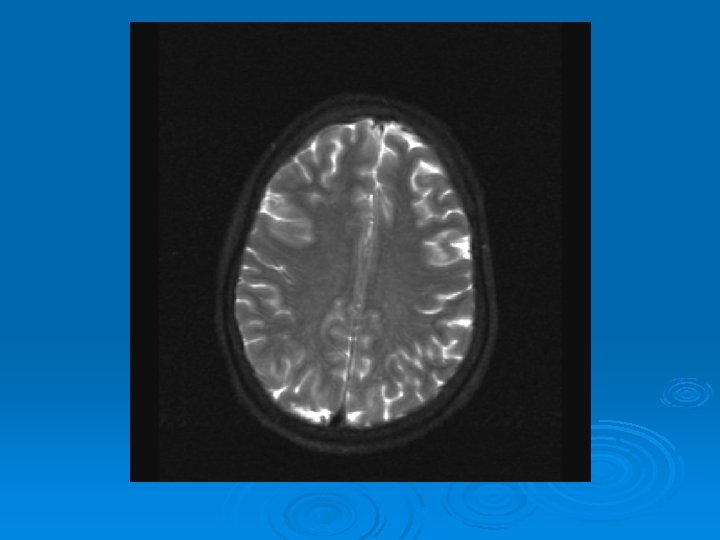
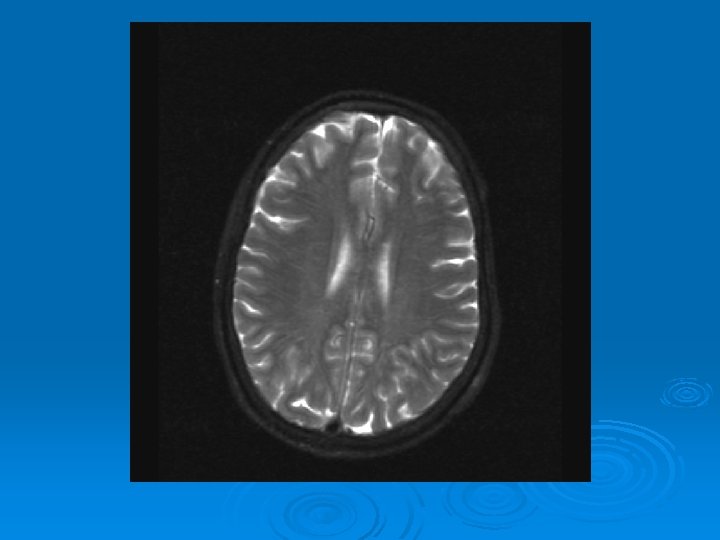
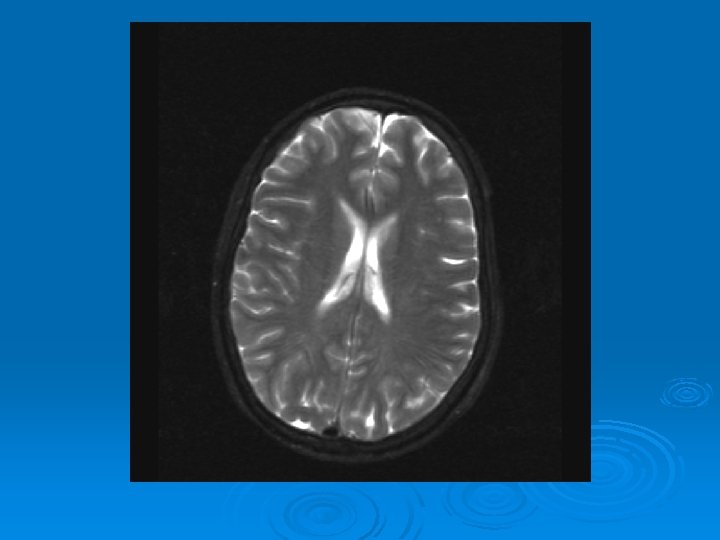
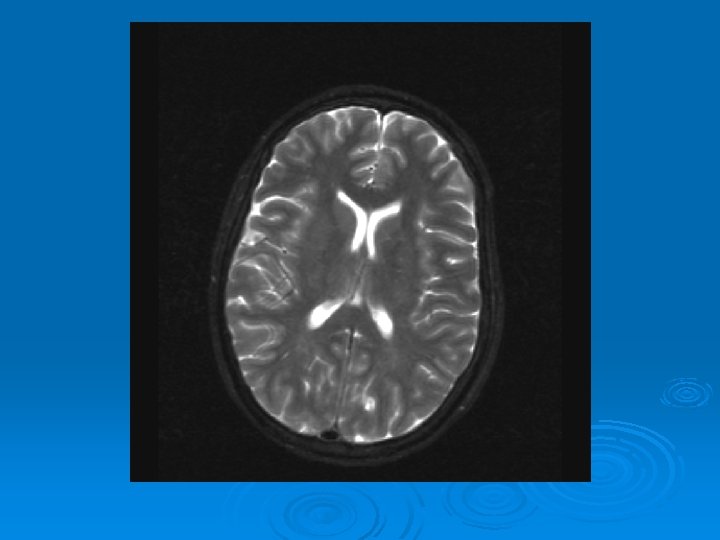
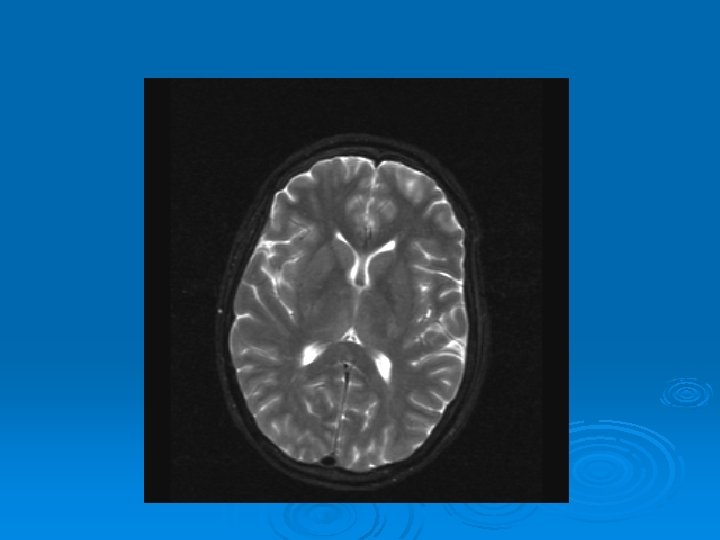
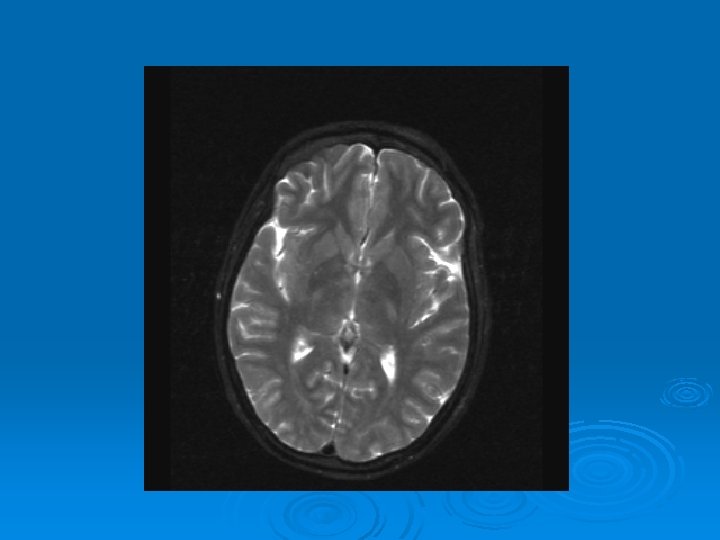
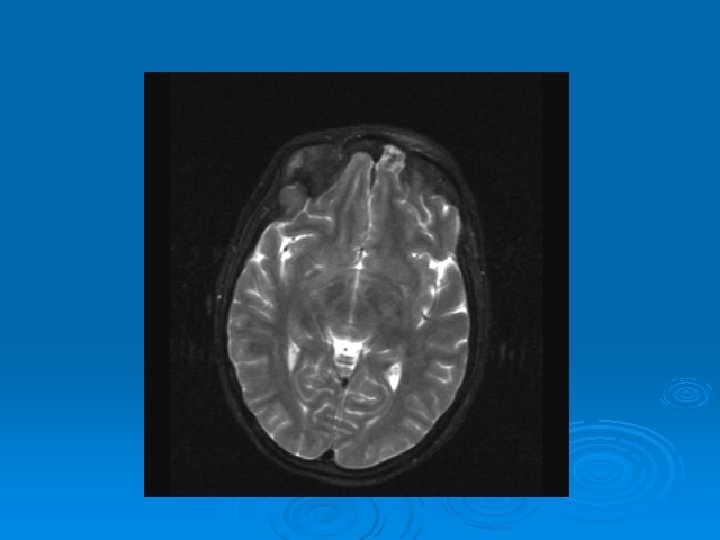

MRI: 2/9/2007 Ø 1. Leptomeningeal enhancement, most prominently seen over the posterior parietal and occipital lobes.

HPI Ø Critical Care Fellow on Transplant Service was preparing for LP and called ID Fellow on call with question “What empiric antifungals should we place this patient on after LP? ”

Past Medical History Ø Cystic fibrosis: Ø Severe pulmonary disease on 4 L via NC continuously Ø Portal gastropathy Ø Hepatic disease Ø Pancreatic insufficiency Ø H/O Multi-drug resistant pseudomonas. Ø Massive hemoptysis in 2005. Ø Hypertrophic pulmonary osteoarthropathy

Social History Ø She was living nearby in a temporary house with her father prior to transplant surgery. Had worked as social worker in the midwest. No etoh, no tobacco. Travel history unknown.

Family History Ø M: alive. Has mitral valve prolapse. F: alive. No pmhx. Sibs: older brother no pmhx. extended family members w/ CF

Medications: Antibiotics Tobramycin 160 mg IV X 1 on 01/25/07 Ø Fluconazole 50 IV QD started 01/23/07 02/04/07 Ø Ciprofloxacin 400 mg IV qhs 1/25/07 present Cefepime 1 g IV Q 12 H--> changed 2 grams iv q 12 --> Ø Vancomycin 1 gram IV 2/9/07 --> Ø Flagyl 500 mg q 6 2/9/07 --> Ø Acyclovir 250 mg iv qday 2/907 --> Ø Abelcet 300 mg iv qday 2/9/07 --> Ø Ø Nystatin swish Ø Chlorhexadine mouth care
 Ø Dopamine gtt Cyclosporine")
Other Medications: Ø Insulin gtt Dilaudid PCA Heparin gtt (off) Ø Dopamine gtt Cyclosporine 6 mg/hr (gtt started 01/21/07) Ø Ø Ø Methylprednisolone 10 mg/12. 5 mg I bid Azathioprine 100 mg IV qd Ø Nexium 40 mg QD Ø Epoetin 4000 units m/w/f Ø Bupivicane via thoracic epidural Ø Albuterol MDI q 6 Ø ADEK vitamins po bid Ø Ativan Ø TPN --stopped today

Allergies Ø AUGMENTIN Ø Keflex Ø Chloramphenicol Ø Azithromyicn

PE Ø Tmax 37. 5 maps 50 -80 , pulse in 80 s, rr 18 -20 pox 98 on 4 L until intubation Now on SIMV 100% 10/5 Tv 500 Ø Primary team exam: Ø General: “jerking” Ø HEENT: NC/AT, pupils ovoid, not reactive CV: RRR, NL no mgr Lung: good air mvt Ø Abd: soft, no bs Ext: 2+ LE edema, clubbing present Ø

Labs: Ø Ø Ø CO 2 22 BUN 26 H Creatinine 1. 6 H Albumin 1. 6 Bilirubin (total) 4. 7 Biliruin (direct) 4. 2 Ø Ø Ø AST 66 ALT 51 Alk P 671 GGT 314 Ø Ø Ø WBC 3. 2 HGB 8. 4 HCT 24. 7 Platelets 53 Ø Microbiology: Ø Ø 2/9/07: CVAD TEMP BLOOD pending 2/9/07: peripheral Blood pending Ø

CXR:

Labs: Ø LP: opening pressure 20 cm. H 20: CSF ANALYSIS tube #1 4 Ø YELLOW Ø Ø Ø RBC 76 35 TNC 15 20 Ø Neutrophils 11 % Lymphocytes 22 % Monocytes 67 % Protein 295 Ø Glucose 63

Labs: Ø CSF: Gram stain Ø 1+ PMN’s 2+ YEAST

Discussion

Micro: Ø Ø Ø CF BAL 1/31/07: right Probable Smooth Pseudomonas aeruginosa 3+ FURTHER I. D. BY CONSULTATION ONLY Ø Ø Probable Stenotrophomonas maltophilia 1+ FURTHER I. D. BY CONSULTATION ONLY Ø Ø 1/25/07 SPUTUM INDUCED Smooth Pseudomonas aeruginosa 2+ Ø Ø Ø Ø Ø TICARC/CLAVULAN R PIPER/TAZOBACT S IMIPENEM R CEFEPIME R CEFTAZIDIME R GENTAMICIN R TOBRAMYCIN I AMIKACIN R TRIMETH/SULFAMET R LEVOFLOXACIN R Ø Ø CF BAL 1/19/07: RLML: Probable coagulase-negative Staphylococcus coagulase-negative species 1+ Ø Ø 2 Probable Smooth Pseudomonas aeruginosa I. D. BY CONSULTATION ONLY Ø Ø CF ADULT BAL 2007 -01 -19 at 0820 Site: RLML Ø Probable Smooth Pseudomonas aeruginosa Ø <10, 000 ORGANISMS/ML Ø NOTE 1/19/07 BAL RLML had been sent for Ø VIRAL, AFB AND FUNGAL cultures and had failed to grow any organism other than candida. Ø Ø PNEUMOCYSTIS DF NEGATIVE CMV PCR, QUAL NEGATIVE
 1/10/07: Ø 1 Smooth Pseudomonas aeruginosa Ø 4+")
Micro: Ø CF TRACHEAL (PRE-TRANSPLANT LUNGS) 1/10/07: Ø 1 Smooth Pseudomonas aeruginosa Ø 4+ Ø Ø PIPERACILLIN MIC 8 S TICARC/CLAV MIC 64 S Ø MEROPENEM R Ø PIP/TAZO MIC 8 S Ø Ø IMIPENEM R IMIPENEM MIC 1 S Ø Ø CEFEPIME MIC 8 S CEFTAZIDIME MIC 2 S Ø Ø GENTAMICIN MIC 32 R TOBRAMYCIN MIC 32 R AMIKACIN R TRIMETH/SULFAMET R Ø Ø CIPROFLOXACIN R CIPROFLOXAC MIC 0. 25 S Ø LEVOFLOXACIN R Ø Ø Ø COLISTIN MIC 2 AMIKACIN MIC 4 S AZTREONAM MIC 16 I Ø Ø Ø Ø Ø 2 Mucoid Pseudomonas aeruginosa 4+ TICARC/CLAVULAN S PIPER/TAZOBACT S CEFTAZIDIME S GENTAMICIN R TOBRAMYCIN S TRIMETH/SULFAMET R CIPROFLOXACIN S LEVOFLOXACIN S 3 Stenotrophomonas maltophilia Ø Ø <1+ 3 COLONIES Ø Ø Ø TICARC/CLAV MIC 64 I CEFTAZIDIME MIC >=256 R TRIMETH/SULFAMET S LEVOFLOXACIN R MINOCYCLINE S

Course: Ø ID Abx recs: Ø ABELCET 5 MG/KG IV QD Ø FLUCYTOSINE 25 MG/KG QDAY WITH FLUCONAZOLE 400 MG IV X 1 5 MG/KG IV GANCYCLOVIR QOD Ø CONTINUE: Ø CEFEPIME 2 GRAMS IV Q 12 VANCOMYCIN 1 GRAM QDAY

Labs: CSF Ø Gram Stain: Yeast was error, there were no yeast visualizable on gram stain 2/9/07 Ø Fungal stain: no fungal elements Ø AFB stain: no organism Ø Crypto Ag: Negative 2/9/07 Ø Bacterial cultures: No growth

Course: Ø 3 PM, RN noticed anisocoria and L pupil non-reactive. Ø Neurology STAT dose mannitol and w/ dilantin. Ø Pt went for stat head Ct:
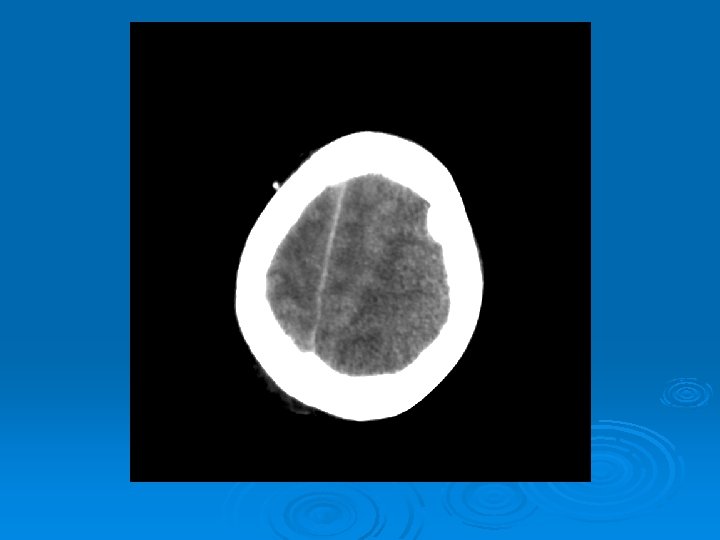
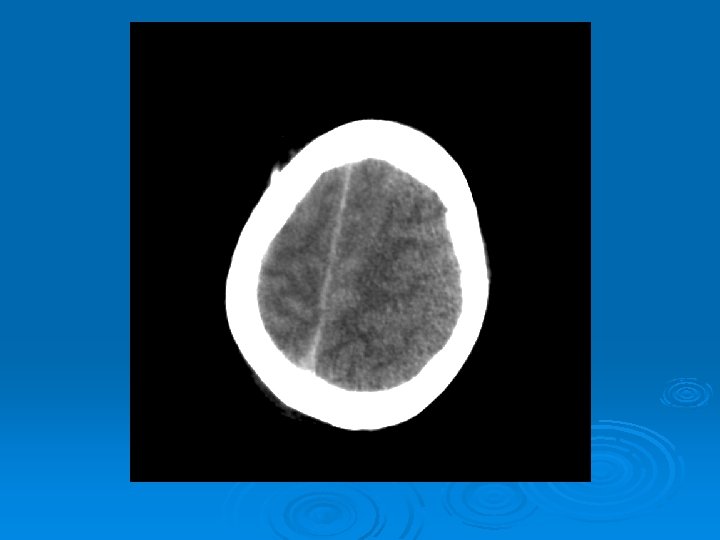
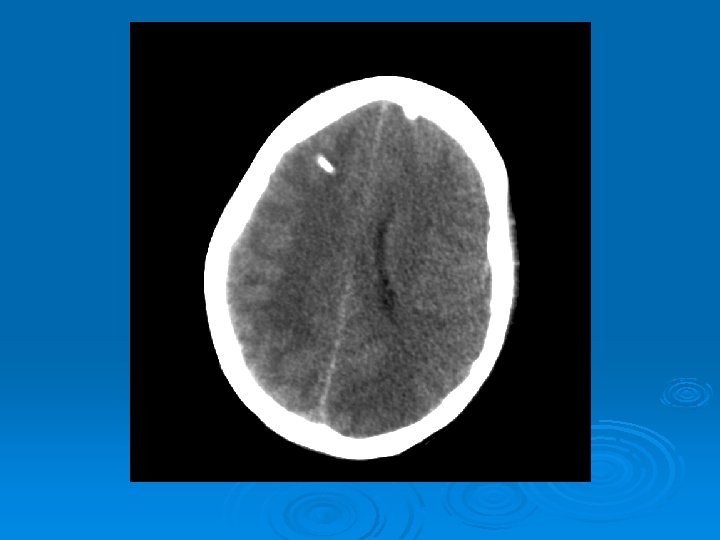
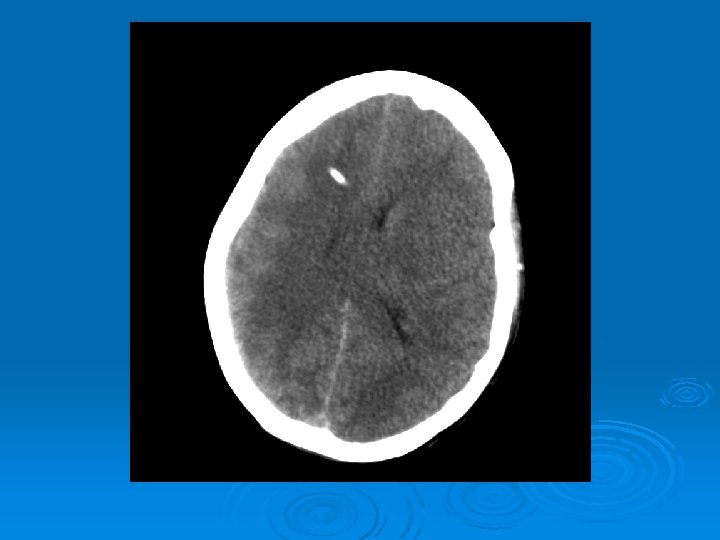
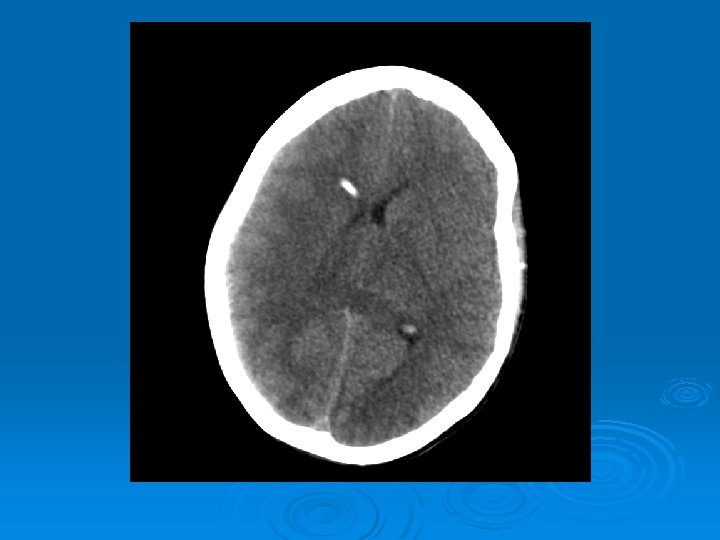
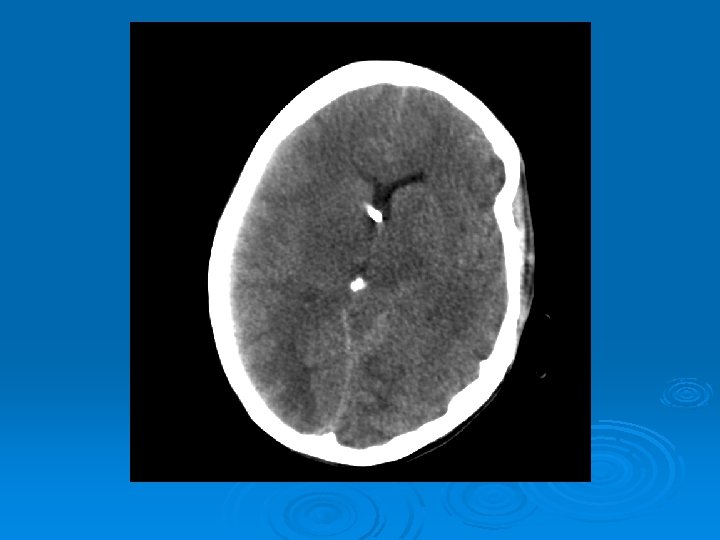
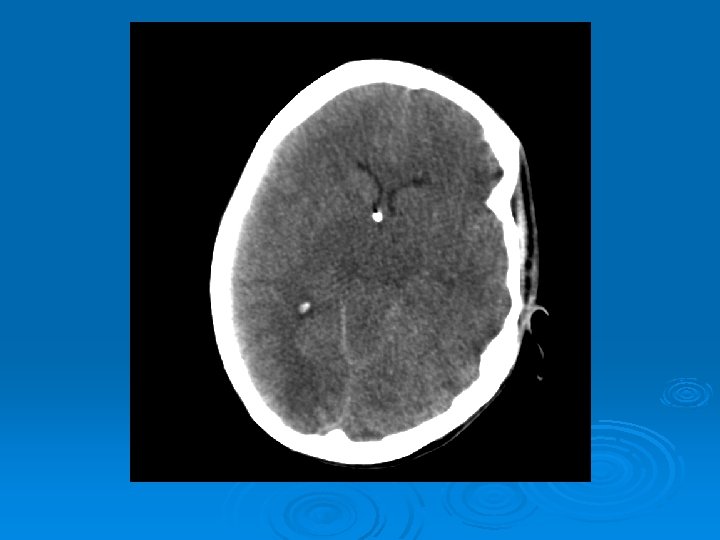
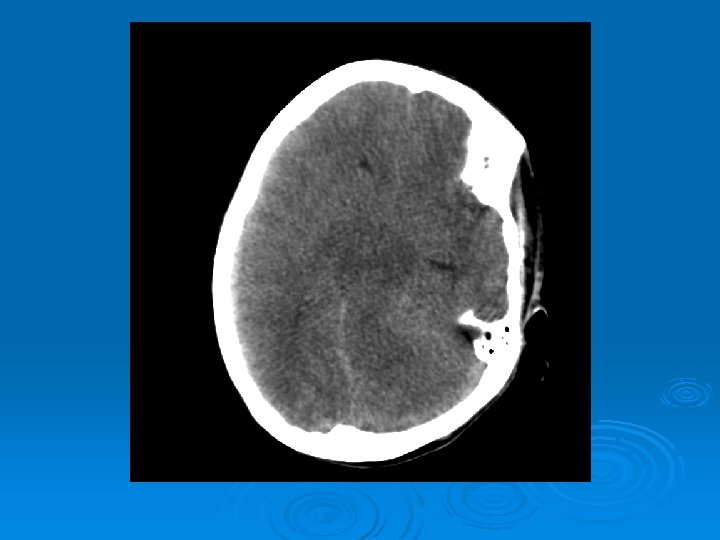
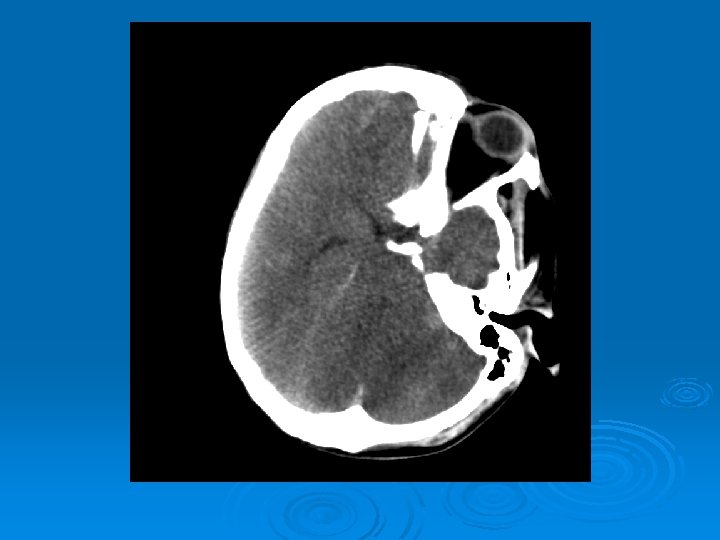
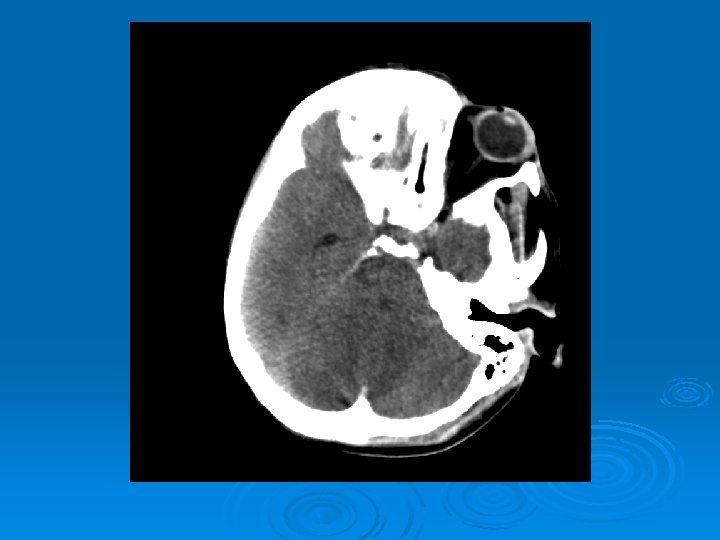

CT head 2/11/07 Ø A right frontal ventriculostomy catheter Ø Diffuse sulcal effacement with thickening of the cortex. Ø Loss of gray-white differentiation and hypodensity in the left parietooccipital region. Ø There is diffuse hypodensity of the cerebellum and brainstem. Ø Ø Ø The basilar cisterns are nearly completely effaced. Ø Impression: Ø Worsened diffuse cerebral edema The lateral ventricles are smaller

Course: Ø Neurosurgery saw pt: on exam she had lost cough, gag reflexes, corneal reflexes, she had flexed RUE, semipurposeful with bilateral extended LE. Ø Concern for herniation: placed Ø ICP 35 -40 10 th-11 th EVD

Course: 1/11/07 Ø off sedation x 1 hr Ø no EO, R 7 mm ovular and NR and L 8 mm ovular , NR no corneals Ø no cough Ø no gag Ø no motor response to central pain Ø no oculocephalic no oculovestibular (cold calorics)

Labs: CSF Ø Bacterial cultures: No growth Ø AFB: no growth Ø Fungal culture no growth Ø CSF: VDRL negative Ø Arbovirus Panel Serum : Negative EEE, WEE, St. Louis, Lacrosse, West Nile Virus

Labs: CSF HSV PCR : NEGATIVE Ø VZV PCR: NEGATIVE Ø HHV 6 PCR: NEGATIVE Ø Ø CMV PCR QUAL POSITIVE Ø Ø CMV VIRAL LOAD BLOOD: 140785 copies Ø EBV VIRAL LD, BLD UNDETECTABLE

Immunology: Ø Ø 1/16/07: TOXOPLASMA IGG NEGATIVE 1/16/07 TOXOPLSMA IGM AB NEGATIVE Ø Ø 1/12/07: CMV IGM NEGATIVE 1/12/07: CMV IGG POSITIVE Ø Ø Ø EBV SEROLOGIES 1/11/07: Ø 1/2007 HSV 1 and 1 Ig. G and Ig. M negative, prior test 2 years earlier positive for HSV Ig. G EBV VCAG IGG POSITIVE EBV VCAG IGM NEGATIVE EBV NUCLEAR IGG POSITIVE

CMV: B Herpes Virus Ø Cytomegalovirus: B herpes virus: Ø Isolated first from human salivary gland. Ø Largest virus that infects humans Ø Linear double stranded DNA encodes 230 nonoverlapping ORFs.

CMV Ø Transmitted by: blood, tissue exposure, perinatally, sexual contact, household occupational exposure. Ø Primary and Secondary Infection: Ø Like all other herpes viruses CMV can establish latent infection. Ø PMN’s, T lymphocytes, endothelial vascular tissue, renal epithelial cells, salivary glands, can harbor latent virus. Immunosuppression: HIV infection, immunosuppressive therapy (ex antilymphocyte antibody (OKT 3) infusion. Ø Illness, can lead to activation from latent state. Ø

CMV: Mononucleosis Ø CMV in healthy young adult can cause infectious mononucleosis syndrome (est 21%); fever, lymphadenopathy, lymphocytosis. Ø Typically “typhoidal” with predominance of fever, lack of sore-throat, enlarged exudative tonsils found in EBV mono. Ø No heterophile antibodies in blood. Low level LFT abnormalities. Jaundice rare Ø Rare complications: Insterstitial PNA, hepatitis, GB syndrome, Meningoencephalitis, myocarditis, TTPenia, hemolytic anemia, rashes Ø 60 -70% CMV seroprevalence in US cities, 100% in some parts of Africa.

CMV: HIV, AIDS pts. Ø HIV, AIDS: CMV most commone viral opportunistic infection (21 -44% of pts with AIDS in pre HAART): Ø CMV retinitis Ø CNS: Polyradiculopathy, Mononeuritis multiplex, painful neuropathy, Meningoencephalitis (see further) Ø GI: Esophagitis, Colitis, cholecystitis, acalculous cholecystitis.

CMV and transplant recipients Ø CMV infection can result in pneumonia, hepatitis, pancreatitis, and gastrointestinal side effects, among others, in the transplant recipient. See timeline for onset Fig. 26– 14 in: Sabiston. Textbook of Surgery: the Biological Basis of Modern Surgical Practice. 17 th ed. Book available online via the UNC-CH Libraries

CMV: After Organ Transplant Ø CMV infections typically occur within first 120 days post transplant when immunosuppression is greatest. Ø Antithymocyte infusions, cyclophoshamide, aztothioprine, steroids, cyclosporine Ø Degree of immunosuppression correlates with risk for infection with BMT > renal transplantation. Ø Symptomatic infection SOT: in 8% kidney, 29% liver, 25% heart, 50% kidney/pancreas, 22% small bowel, 39% heart-lung

CMV: After Organ Transplant Ø CMV: pneumonitis, hepatitis, esophagitis, colitis, GB, pancreatitis, epididymitis, retinitis, meningoencephaltis. Frequently occurs in transplanted organ. Ø Risk dependent on Serological status of Donor(D) and Recipient Ø Ø D+/R- (85%)> D+/R+ (69%> D-R+(58)> D-/R- Ø Primary infection from blood, transplanted organ, or more commonly reactivation.
 prophylaxis with acyclovir,")
CMV: Prophylaxis and Preemptive Rx Ø Prophylaxis: Universal, Selective (D+/R-, D-/R+) prophylaxis with acyclovir, valacyclovir, gancyclovir, valgancyclovir. Ø Preemptive Rx: Monitor peripheral blood viral load, evidence of end-organ disease and then treat.

CMV CNS Disease: Ø CMV: hematogenous spread in monocytes, macrophages from blood to CNS. Ø Possibly through direct infection of CNS Ø Can infect: astrocytes, neurons, oligodendroglia, capillary endothelia

CMV CNS Disease: Most Data from HIV, AIDS Reported cases of cytomegalovirus of the brain, 1965 to 1995 Ø See table in: l Arribas et al, Cytomegalovirus Encephalitis, Annals of Internal Medicine, 1996, Vol 125, Issue 7

CMV CNS Disease: Polyradiculopathy Ø Symptoms: Ø Ø Initial lower extremity weakness Sacral pain, paresthesias Urinary retention Ascending flaccid paralysis Ø Ø Labs: CSF: Polymorphonuclear pleocytosis, Low Glucose (<40) +CMV by PCR in CSF Ø Peripheral Blood: CMV viremia Ø MRI: may see transverse hyperintense lesions on T 2 WI, gad enhancement of myelin, meninges, roots of spinal cord. Ø Treatment: Critical early diagnosis, IV gancyclovir, (if exp to gancylovir) add foscarnet, (50% respond, CI 1995)

CMV encephalitis lesions Pathologic lesions associated with cytomegalovirus encephalitis Ø See images in: l Arribas et al, Cytomegalovirus Encephalitis, Annals of Internal Medicine, 1996, Vol 125, Issue 7

CMV: Encephalitis Ø The microglial form: first described in renal transplant patient. Several glial nodules predominantly in grey matter.

CMV: Ventriculoencephalitis Ø Clinical: Can have abrupt presentation of confusion, apathy, impaired memory, withdrawal, nystagmus, motor weakness, cranial nerve deficits, ataxia, seizures, coma. Can rapidly progress. Ø Labs: CSF: Monocytic Pleocytosis, Low Glucose CMV PCR Positive in CSF: (Sensitivity, Specifity 80, 90%, PPV, NPV, 86 -92, 9598%) Serum CMV viremia Ø Ø Ø MRI: Subependymal enhancement, diffuse hyperintense T 2 WI, ventriculomegaly.

MRI of CMV patient Magnetic resonance images of a patient with cytomegalovirus ventriculitis Ependymal enhancement after injection of gadolinium. DPTA seen on coronal T 1 -weighted image. Ø Highly abnormal ependmal signal on proton densityweighted image of the brain in axial section. Ø Ø See images in: l Arribas et al, Cytomegalovirus Encephalitis, Annals of Internal Medicine, 1996, Vol 125, Issue 7

CMV Encephalitis in Transplant Patients Ø Miller et al, 2005, reviewed 4 prior documented cases (+one probable case) with new case of CNS infection in Peripheral Blood Stem Cell Transplant Patients. Ø 3 of 4 documented cases clinically had evidence of ventriculoencephalitis. Ø Rapid progression of cognitive dysfunction, confusion.

CMV Encephalitis in Transplant Patients Ø 2 of patients including their case report had high CSF viral loads (ex > one million) with relatively low viremia, 2 K range Ø 4 of 5 had CSF DNA genotypes performed. Ø One had UL 97 (gancyclovir R) and one had UL 54 (R to gancylovir and cidofovir) Ø Despite failing antiviral therapy, 2 of patients had no resistance mutations in DNA derived from CSF. Ø Ø Compartamentalization of CMV disease to CNS? Problems with CNS levels of Drugs?

Autopsy of Brain See Figure 1 in: Miller, G et al, Cytomegalovirus Ventriculoencephalitis in Peripheral Blood Stem Cell Transplant Recipient, CID 2006: 42: e 26 -9.
")
CMV Encephalitis: Treatment Ø Appropriate treatment is not defined Ø Anduze-Faries, et al (2000) published nonblinded pilot, multicenter study with HIV infected patients with myelitis (14), encephalitis (17) of patients who received gancyclovir 5 mg/kg iv bid, foscarnet 90 mg/kg bid for median of 41 days followed by maintenance therapy with once daily gancyclovir and foscarnet.
 showed clinical improvement or stabilization, 8 did not")
CMV Encephalitis: Treatment Ø 23 (74%) showed clinical improvement or stabilization, 8 did not respond. Ø Median survival for all of the patients was 3 months. Ø Many experts recommend dual gancyclovir, foscarnet bid, followed by lifelong once daily dose of combination therapy

CMV Encephalitis: Treatment Ø Other drugs: Ø Cidofovir (cytosine analog with probenecid Ø Leflunomide: interferes with late stage viral assembly

References: Ø Arribas et al, Cytomegalovirus Encephalitis, Annals of Internal Medicine, 1996, Vol 125, Issue 7 Ø Boivin, Guy. Diagnosis of Herpesvirus Infection of the Central Nervous System, HERPES Ø Crumpacker and Wadwa, chapter 134 Cytomegalovirus, Mandell and Bennett’s Textbook of Infectious Disease, p 1786 -, 2005 Ø Book available online via the UNC-CH Libraries Ø Griffiths, Paul, Cytomegalovirus Infection in the Central Nervous System, HERPES, Ø Maschke, M et al, CNS Manifestations of Cytomegalovirus Infections: Diagnosis and Treatment, CNS Drugs 2002: 16(5) 203 -315. Ø Miller, G et al, Cytomegalovirus Ventriculoencephalitis in Peripheral Blood Stem Cell Transplant Recipient, CID 2006: 42: e 26 -9. Ø Trulock, F, Cytomegalovirus infection in lung transplant recipients, Upto. Date 2006.

Search Pub. Med Ø CMV and the central nervous system l l Case Reports Reviews Differential Diagnosis Drug therapy
21a0163f4fdf5bb5bc4e4e0890656b78.ppt