
VALVULARHEARTDISEASE InternalMedicineDidactics August 12, 2009 StevenR. BruhlMD,











































valvular_heart_disease_im_8-12.ppt
- Размер: 4.3 Mегабайта
- Количество слайдов: 80
Описание презентации VALVULARHEARTDISEASE InternalMedicineDidactics August 12, 2009 StevenR. BruhlMD, по слайдам
VALVULARHEARTDISEASE Internal. Medicine. Didactics August 12, 2009 Steven. R. Bruhl. MD, MS
Overview • Aortic. Stenosis • Mitral. Stenosis • Aortic. Regurgitation – Acuteand. Chronic • Mitral. Regurgitation – Acuteand. Chronic
• Etiology • Pathophysiology • Physical. Exam • Natural. History • Testing • Treatment
Aortic. Stenosis
Aortic. Stenosis. Overview: • Normal. Aortic. Valve. Area: 34 cm 2 • Symptoms: Occurwhenvalveareais 1/4 th ofnormalarea. • Types: – Supravalvular – Subvalvular – Valvular
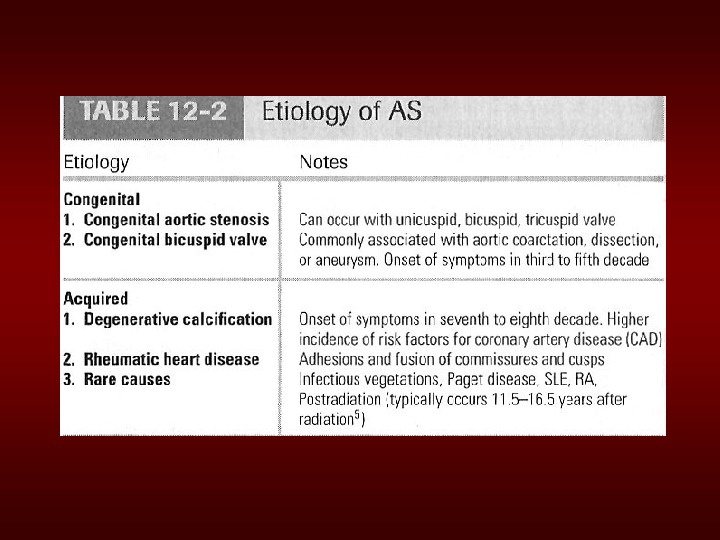
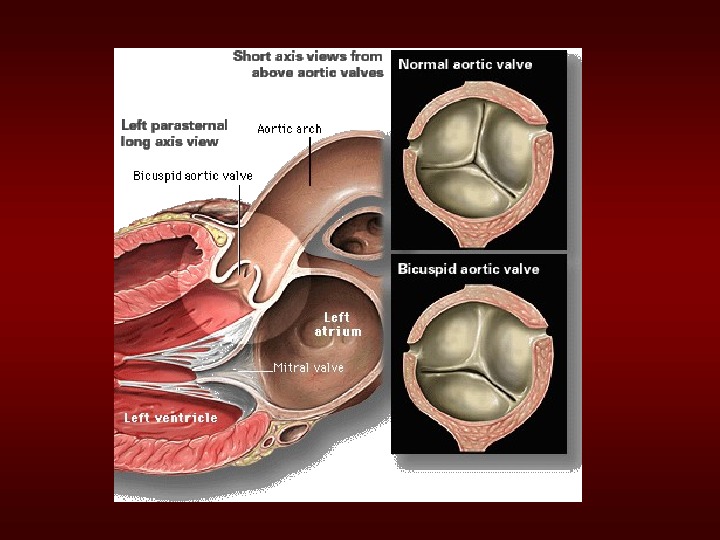
Etiologyof. Aortic. Stenosis • Congenital • Rheumatic • Degenerative/Calcific Patientsunder 70: >50%haveacongenital cause Patientsover 70: 50%duetodegenerative
Pathophysiologyof. Aortic. Stenosis • Apressuregradientdevelopsbetweenthe leftventricleandtheaorta. (increased afterload) • LVfunctioninitiallymaintainedby compensatorypressurehypertrophy • Whencompensatorymechanisms exhausted, LVfunctiondeclines.
Presentationof. Aortic. Stenosis Syncope: (exertional) Angina: (increasedmyocardialoxygen demand; demand/supplymismatch) Dyspnea: onexertionduetoheartfailure (systolicanddiastolic) Suddendeath
Physical. Findingsin. Aortic. Stenosis • Slowrisingcarotidpulse( pulsustardus )& decreasedpulseamplitude( pulsusparvus ) • Heartsoundssoftandsplitsecondheart sound, S 4 gallopdueto. LVH. • Systolicejectionmurmur cresendodecrescendocharacter. This peaks lateras the severity ofthestenosis increases. – Loudnessdoes. NOTtellyouanythingabout severity
Natural. History • Mild. ASto. Severe. AS: – 8%in 10 years – 22%in 22 years – 38%in 25 years • Theonsetofsymptomsisapoorprognostic indicator.
Evaluationof. AS • Echocardiographyisthemostvaluabletest fordiagnosis, quantificationandfollowup ofpatientswith. AS. • Twomeasurementsobtainedare: a) Leftventricularsizeandfunction: LVH, Dilation, and. EF b) Dopplerderivedgradientandvalvearea (AVA)
Evaluationof. AS Cardiaccatheterization: Shouldonlybedoneforadirect measurementifsymptomseverityandechoseveritydon’t match. ORpriortoreplacementwhenreplacementisplanned.
Managementof. AS • General IEprophylaxisindentalprocedures withaprosthetic. AVorhistoryofendocarditis. • Medical limitedrolesince. ASisamechanical problem. Vasodilatorsare relatively contraindicated insevere. AS • Aortic. Balloon. Valvotomy showslittle benefit. • Surgical. Replacement: Definitivetreatment
Echo. Surveillance • Mild: Every 5 years • Moderate: Every 2 years • Severe: Every 6 monthsto 1 year
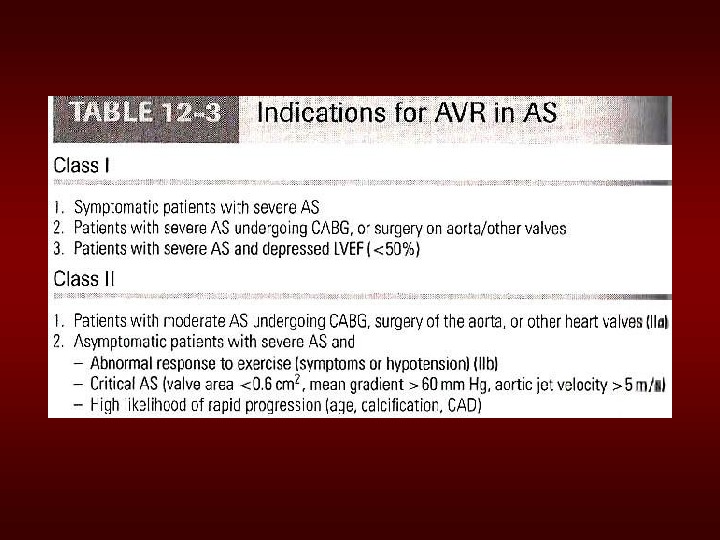
Simplified Indicationsfor. Surgery in. Aortic. Stenosis • Any. SYMPTOMATICpatientwithsevere AS(includessymptomswithexercise) • Anypatientwithdecreasing. EF • Anypatientundergoing. CABGwith moderateorsevere. AS
Summary • Diseaseofaging • Lookforthesignsonphysicalexam • Echocardiogramtoassessseverity • Asymptomatic: Medicalmanagementand surveillance • Symptomatic: Ao. Vreplacement(evenin elderlyand. CHF)
Mitral. Stenosis
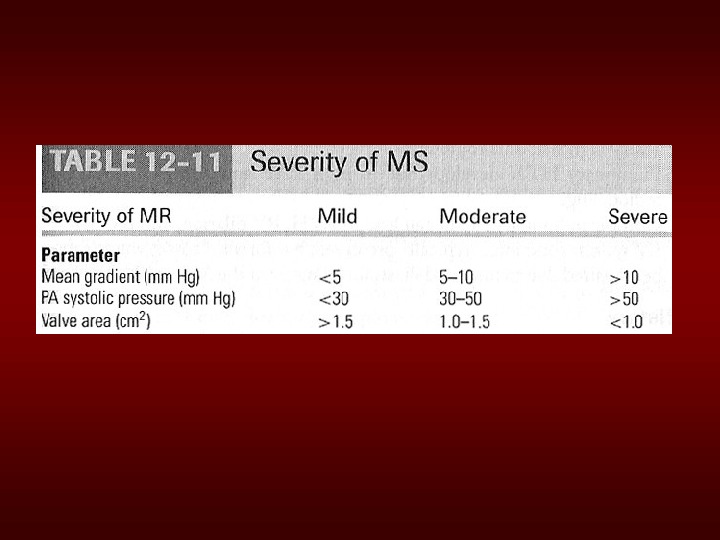
Mitral. Stenosis. Overview • Definition: Obstructionof. LVinflowthat preventsproperfillingduringdiastole • Normal. MVArea: 46 cm 2 • Transmitralgradientsandsymptomsbegin atareaslessthan 2 cm 2 • Rheumaticcarditisisthepredominantcause • Prevalenceandincidence: decreasingdue toareductionofrheumaticheartdisease.
Etiologyof. Mitral. Stenosis • Rheumaticheartdisease: 7799%ofall cases • Infectiveendocarditis: 3. 3% • Mitralannularcalcification: 2. 7%
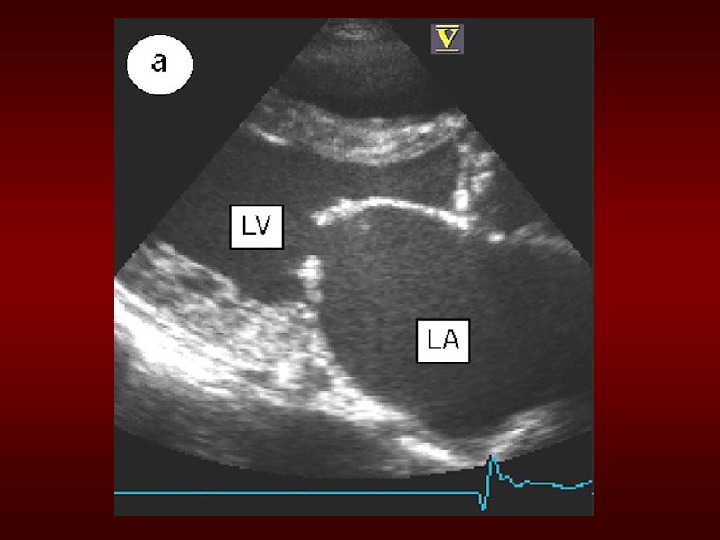
MSPathophysiology • Progressive. Dyspnea(70%): LAdilation pulmonarycongestion(reducedemptying) – worsewithexercise, fever, tachycardia, andpregnancy • Increased. Transmitral. Pressures: Leadstoleft atrialenlargementandatrialfibrillation. • Rightheartfailuresymptoms: dueto Pulmonaryvenous. HTN • Hemoptysis: duetoruptureofbronchialvessels duetoelevatedpulmonarypressure
Natural. Historyof. MS • Diseaseofplateaus: – Mild. MS: 10 yearsafterinitial. RHDinsult – Moderate: 10 yearslater – Severe: 10 yearslater • Mortality: Duetoprogressivepulmonary congestion, infection, andthromboembolism.
Physical. Exam. Findingsof. MS • prominent»a»waveinjugularvenouspulsations : Duetopulmonaryhypertensionandrightventricular hypertrophy • Signsofrightsidedheartfailure: inadvanced disease • Mitralfacies: When. MSissevereandthecardiac outputisdiminished, thereisvasoconstriction, resultinginpinkishpurplepatchesonthecheeks
• Diastolicmurmur: – Lowpitched diastolicrumble mostprominentat theapex. – Heardbestwiththepatientlyingontheleftside inheldexpiration – Intensityofthediastolicmurmur doesnot correlate withtheseverityofthestenosis. Heart. Soundsin. MS
• Loud. Opening. S 1 snap: heardattheapexwhen leafletsarestillmobile – Duetotheabrupthaltinleafletmotioninearly diastole, afterrapidinitialrapidopening, dueto fusionattheleaflettips. – Ashorter. S 2 toopeningsnapintervalindicates moreseveredisease. Heart. Soundsin. MS
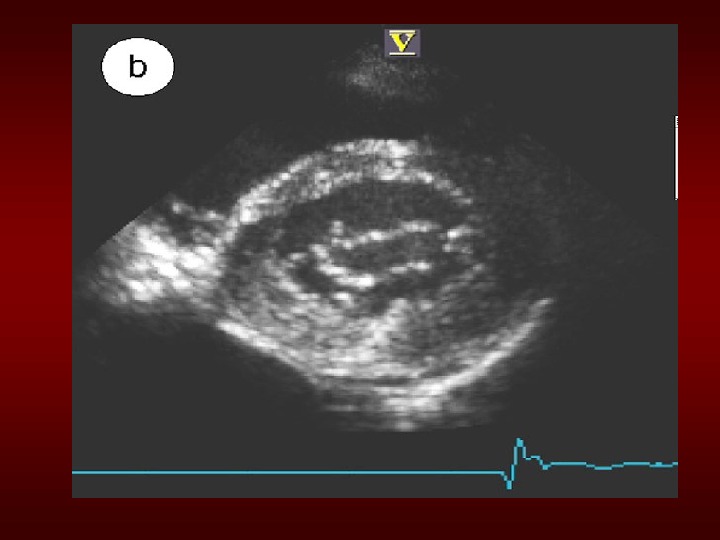
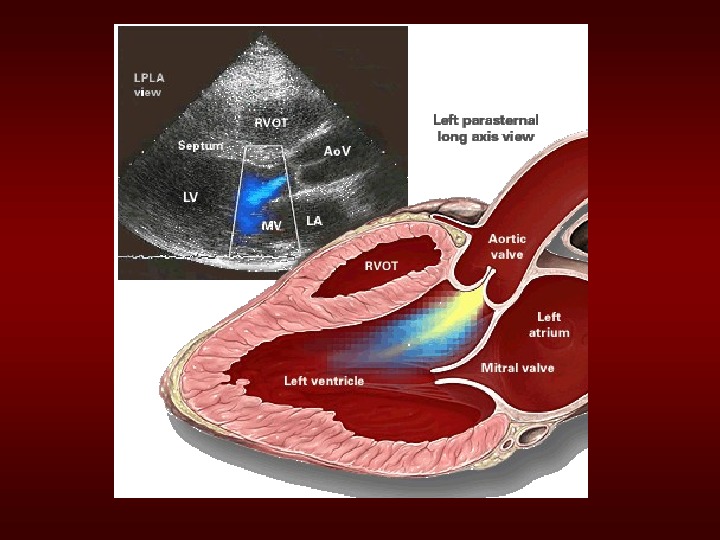
Evaluationof. MS • ECG : mayshowatrialfibrillationand. LA enlargement • CXR : LAenlargementandpulmonary congestion. Occasionallycalcified. MV • ECHO : The GOLDSTANDARD for diagnosis. Assesmitralvalvemobility, gradientandmitralvalvearea
Managementof. MS Serialechocardiography: – Mild: 35 years – Moderate: 12 years – Severe: yearly • Medications: MSlike. ASisamechanicalproblem andmedicaltherapydoesnotpreventprogression blockers, CCBs, Digoxinwhichcontrolheart rateandhenceprolongdiastoleforimproved diastolicfilling – Duireticsforfluidoverload
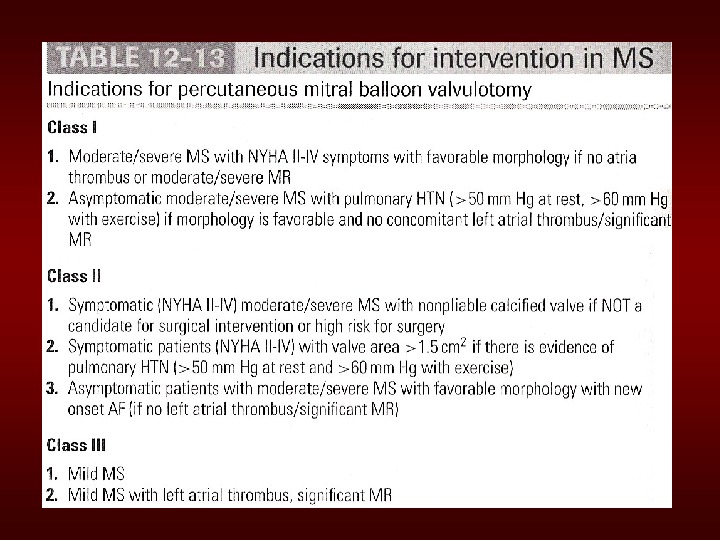
Managementof. MS • Identifypatientearlywhomightbenefitfrom percutaneousmitralballoonvalvotomy. • IEprophylaxis: Patientswithprostheticvalvesor a. Hxof. IEfordentalprocedures.
Simplified Indicationsfor. Mitral valvereplacement • ANYSYMPTOMATIC Patientwith NYHAClass. IIIor. IVSymptoms • Asymptomaticmoderateor. Severe. MSwith apliablevalvesuitablefor. PMBV
Aortic. Regurgitation
Aortic. Regurgitation. Overview • Definition: Leakageofbloodinto. LVduring diastoleduetoineffectivecoaptationofthe aorticcusps
Etiologyof. Acute. AR • Endocarditis • Aortic. Dissection • Physical. Findings: – Widepulsepressure – Diastolicmurmur – Floridpulmonaryedema
Treatmentof. Acute. AR • True. Surgical. Emergency: • Positiveinotrope: (eg, dopamine, dobutamine) • Vasodilators: (eg, nitroprusside) • Avoidbetablockers • Donotevenconsideraballoonpump
Etiologyof. Chronic. AR • Bicuspidaorticvalve • Rheumatic • Infectiveendocarditis
Pathophysiologyof. AR • Combinedpressure. ANDvolumeoverload • Compensatory. Mechanisms: LVdilation, LVH. Progressivedilationleadstoheart failure
Natural. Historyof. AR • Asymptomaticuntil 4 th or 5 th decade • Rateof. Progression: 46%peryear • Progressive. Symptomsinclude: Dyspnea: exertional, orthopnea, and paroxsymalnocturnaldyspnea Nocturnalangina: duetoslowingofheartrate andreductionofdiastolicbloodpressure Palpitations: duetoincreasedforceof contraction
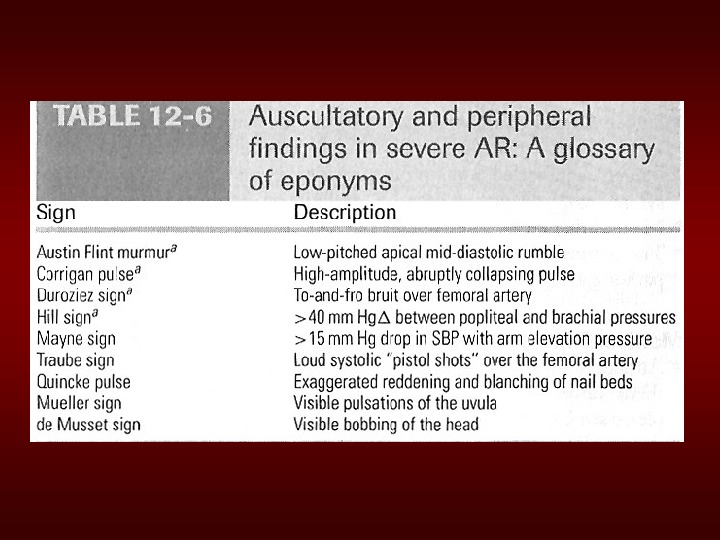
Physical. Examfindingsof. AR • Widepulsepressure: mostsensitive • Hyperdynamicanddisplacedapicalimpulse • Auscultation – Diastolicblowingmurmur attheleftsternal border – Austinflintmurmur (apex): Regurgitantjet impingesonanterior. MVLcausingittovibrate – Systolicejectionmurmur : duetoincreasedflow acrosstheaorticvalve
MRIofthe. Heart. Revealinga. Central, High. Velocity. Jet. Projectingintothe. Left. Ventricular. Cavity. Thejetclearlystrikestheanteriormitralvalveleaflet, causingdistortionandprematureclosure duringdiastole.
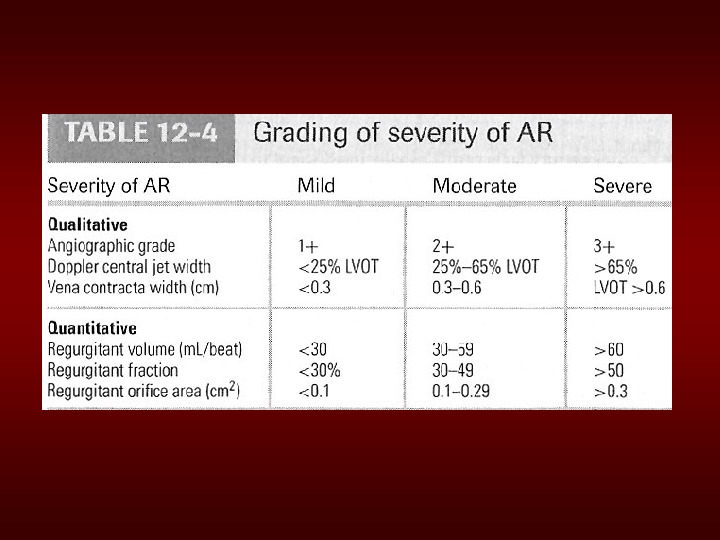
The. Evaluationof. AR • CXR: enlargedcardiacsilhouetteandaortic rootenlargement • ECHO : Evaluationofthe. AVandaorticroot withmeasurementsof. LVdimensionsand function(cornerstonefordecisionmakingand followupevaluation) • Aortography: Usedtoconfirmtheseverityof disease
Managementof. AR • General : IEprophylaxisindentalprocedures withaprosthetic. AVorhistoryof endocarditis. • Medical: Vasodilators(ACEI’s), Nifedipine improvestrokevolumeandreduce regurgitation onlyifptsymptomaticor. HTN. • Serial. Echocardiograms: tomonitor progression. • Surgical. Treatment: Definitive. Tx
Simplified. Indicationsfor. Surgical Treatmentof. AR • ANYSymptomsatrestorexercise • Asymptomatictreatmentif: – EFdropsbelow 50%or. LVbecomes dilated
Mitral. Regurgitation
• Definition: Backflowofbloodfromthe. LV tothe. LAduringsystole • Mild(physiological)MRisseenin 80%of normalindividuals. Chronic. Mitral. Regurgitation Overview
Acute. MR • Endocarditis • Acute. MI: • Malfunctionordisruptionofprosthetic valve
Managementof. Acute. MR • Myocardialinfarction: Cardiaccathor thrombolytics • Mostothercasesofmitralregurgitation isafterloadreduction: – Diureticsandnitrates – nitroprusside, eveninthesettingofa normalbloodpressure.
Managementof. Acute. MR • Donotattempttoalleviatetachycardia withbetablockers. Mildtomoderate tachycardiaisbeneficialinthesepatients becauseitallowslesstimefortheheartto havebackfill, whichlowersregurgitant volume.
Treatmentof. Acute. MR • Balloon. Pump • Nitroprussideevenifhypotensive • Emergent. Surgery
• Myxomatousdegeneration(MVP) • Ischemic. MR • Rheumaticheartdisease • Infective. Endocarditis Etiologiesof. Chronic. Mitral Regurgitation
Pathophysiologyof. MR • Pure. Volume. Overload • Compensatory. Mechanisms: Leftatrial enlargement, LVHandincreased contractility – Progressiveleftatrialdilationandright ventriculardysfunctionduetopulmonary hypertension. – Progressiveleftventricular volumeoverload leadstodilation andprogressiveheartfailure.
Physical. Examfindingsin. MR • Auscultation: soft. S 1 anda holosystolic murmurattheapexradiatingtotheaxilla – S 3(CHF/LAoverload) – Inchronic. MR, theintensityofthemurmur doescorrelate withtheseverity. • Exertion. Dyspnea: (exerciseintolerance) • Heart. Failure: Maycoincidewith increasedhemodynamicburdene. g. , pregnancy, infectionoratrialfibrillation
The. Natural. Historyof. MR • Compensatoryphase: 1015 years • Patientswithasymptomaticsevere. MR havea 5%/yearmortalityrate • Oncethepatient’s. EFbecomes<60% and/orbecomessymptomatic, mortality risessharply • Mortality: Fromprogressivedyspneaand heartfailure
Imagingstudiesin. MR • ECG: Mayshow, LAenlargement, atrial fibrillationand. LVhypertrophywithsevere. MR • CXR: LAenlargement, centralpulmonary arteryenlargement. • ECHO: Estimationof. LA, LVsizeand function. Valvestructureassessment – TEEiftransthoracicechoisinconclusive
Managementof. MR • Medications a) Vasodilatorsuchashydralazine b) Ratecontrolforatrialfibrillationwith blockers, CCB, digoxin c) Anticoagulationinatrialfibrillationandflutter d) Diureticsforfluidoverload
Managementof. MR • Serial. Echocardiography: – Mild: 23 years – Moderate: 12 years – Severe: 612 months • IEprophylaxis: Patientswithprosthetic valvesora. Hxof. IEfordentalprocedures.
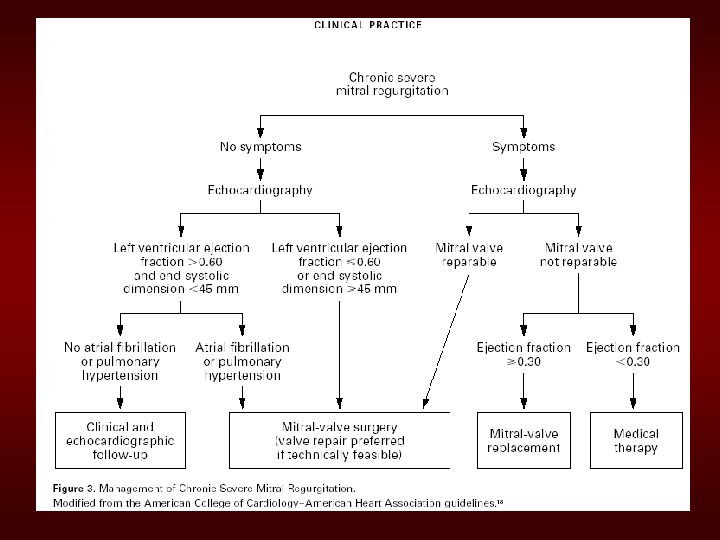
Simplified. Indicationsfor. MV Replacementin. Severe. MR • ANYSymptoms atrestorexercisewith (repairiffeasible) • Asymptomatic: – If. EF<60% – Ifnewonsetatrialfibrillation
THANKYOU