

1698694af27c60035493d65d691332f1.ppt
- Количество слайдов: 57
 University of Minnesota Information Technology in Healthcare Course: MILI/PUBH 6562 Fall Semester B, 2009 Stephen T. Parente, Ph. D. Associate Professor, UM sparente@csom. umn. edu
University of Minnesota Information Technology in Healthcare Course: MILI/PUBH 6562 Fall Semester B, 2009 Stephen T. Parente, Ph. D. Associate Professor, UM sparente@csom. umn. edu
 Class # 3 Health IT Data Structure: The Insurer • • • Basic data structures Units of analysis Health data over time Health insurance data architecture Small group exercise
Class # 3 Health IT Data Structure: The Insurer • • • Basic data structures Units of analysis Health data over time Health insurance data architecture Small group exercise
 Data Structure Fundamentals • Simple text/column data • Pre-packaged data • Relational databases
Data Structure Fundamentals • Simple text/column data • Pre-packaged data • Relational databases
 Simple Column Text Data Patient Joe Joe Mary Penny DOS 02/03/09 06/05/09 01/06/09 04/23/09 Procedure MD Visit Lab test MD Visit Eye Exam Allowed $100 $60 $100 $80
Simple Column Text Data Patient Joe Joe Mary Penny DOS 02/03/09 06/05/09 01/06/09 04/23/09 Procedure MD Visit Lab test MD Visit Eye Exam Allowed $100 $60 $100 $80
 Pre-packaged databases • • • MS-Access databases SQL databases SAS databases SPSS databases STATA databases Excel spreadsheets
Pre-packaged databases • • • MS-Access databases SQL databases SAS databases SPSS databases STATA databases Excel spreadsheets
 Relational Databases • The database stores data in individual files or tables with data items arranged in rows and columns. • AT LEAST one data item (the key) is common to each table and is used to LINK two or more tables for ad hoc queries. • Common method to use relational databases is through SQL (structured query language).
Relational Databases • The database stores data in individual files or tables with data items arranged in rows and columns. • AT LEAST one data item (the key) is common to each table and is used to LINK two or more tables for ad hoc queries. • Common method to use relational databases is through SQL (structured query language).
 Health Data Display by Different Units of Analysis • • • By provider By person By episode/incident By transactions Over fixed units of time
Health Data Display by Different Units of Analysis • • • By provider By person By episode/incident By transactions Over fixed units of time
 By Person
By Person
 By Episode
By Episode
 By Transaction
By Transaction
 Health Data Representation: Over Time? Jan Apr July Oct Dec =Pysch consult $50 K Mental Health Cumulative Cost Well Normal $0 Sick
Health Data Representation: Over Time? Jan Apr July Oct Dec =Pysch consult $50 K Mental Health Cumulative Cost Well Normal $0 Sick
 Insurers’ Role in Health Information Technology • They are the ‘links’ that connect to everything about a patient in an electronic form. – Employers – Providers – Patients – Government agencies – Researchers
Insurers’ Role in Health Information Technology • They are the ‘links’ that connect to everything about a patient in an electronic form. – Employers – Providers – Patients – Government agencies – Researchers
 Insurer’s IT Paradox • They are being held accountable for an insured patient’s total care. • Best breadth of data – Most all places of service – ‘Standardized’ data • Worst detail – No clinical info on patient health status and outcomes.
Insurer’s IT Paradox • They are being held accountable for an insured patient’s total care. • Best breadth of data – Most all places of service – ‘Standardized’ data • Worst detail – No clinical info on patient health status and outcomes.
 IS Management Structure CEO COO UR MCO CIO MIS Claims Systems CFO Actuarial Accounting Working Group Backbone
IS Management Structure CEO COO UR MCO CIO MIS Claims Systems CFO Actuarial Accounting Working Group Backbone
 HEALTH INSURANCE CLAIM FORM
HEALTH INSURANCE CLAIM FORM
 The Health MIS Pyramid Decision Support Software Life Support Software Clinical & Financial Data Hardware
The Health MIS Pyramid Decision Support Software Life Support Software Clinical & Financial Data Hardware
 Insurer Hardware - Mainframe
Insurer Hardware - Mainframe
 Insurance Database Architecture • • Claims Membership Provider files Case management Utilization review / Demand Management Decision-support databases Analytic / Financial data
Insurance Database Architecture • • Claims Membership Provider files Case management Utilization review / Demand Management Decision-support databases Analytic / Financial data
, submitted electronically (80%) - on average. • Key") Claims Data • Entered manually (20%), submitted electronically (80%) - on average. • Key items: – Claim ID and date or service – Member / Subscriber ID – Provider of service – Diagnosis & procedure – Charges, reimbursements & copays – Administrative information
Claims Data • Entered manually (20%), submitted electronically (80%) - on average. • Key items: – Claim ID and date or service – Member / Subscriber ID – Provider of service – Diagnosis & procedure – Charges, reimbursements & copays – Administrative information
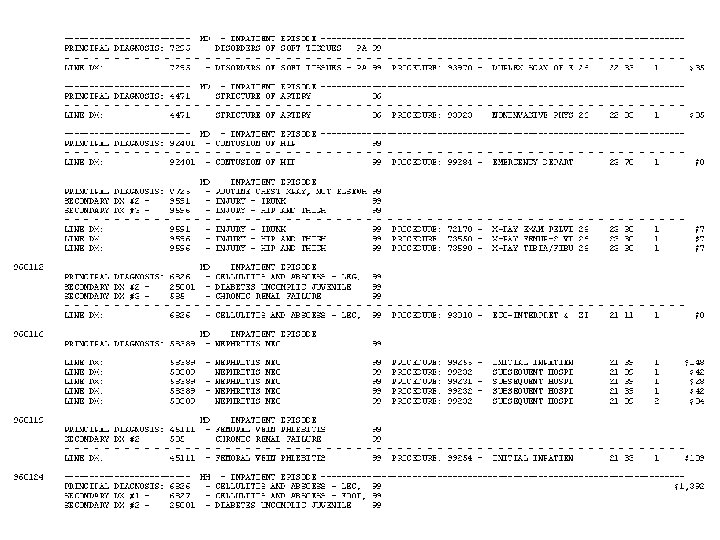
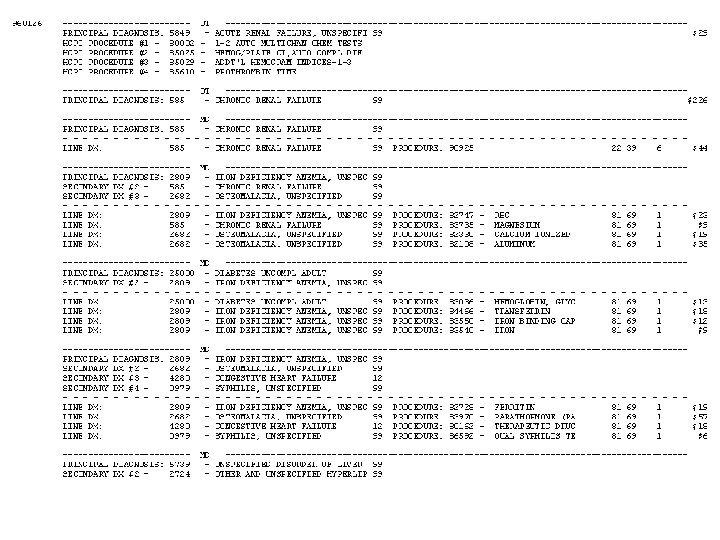
 Claims Data Example
Claims Data Example
 Claims Data Example
Claims Data Example
 •") Membership / Subscriber Data • Member / Subscriber ID (sometimes not person specific!) • If managed care, assigned gatekeeper • Dates of enrollment • Age, gender, case-mix, health risks • Address • Type of policy, employer • Status of benefits used during enrollment
Membership / Subscriber Data • Member / Subscriber ID (sometimes not person specific!) • If managed care, assigned gatekeeper • Dates of enrollment • Age, gender, case-mix, health risks • Address • Type of policy, employer • Status of benefits used during enrollment
 Subscriber Data Example
Subscriber Data Example
 Provider Files • Used to pay bills and identify providers to be included in ‘Panels’ for new products. • Key Data Items: – Provider ID – Specialty, Board Certification, Education – Malpractice history & insurance – Address – Profiling summary
Provider Files • Used to pay bills and identify providers to be included in ‘Panels’ for new products. • Key Data Items: – Provider ID – Specialty, Board Certification, Education – Malpractice history & insurance – Address – Profiling summary
 Provider File Example
Provider File Example
 Case Management • Patient tracking systems • Check to see if recommended ‘process of care’ is occurring as part of good quality care. • Patient reminder systems (mail) • Provider reminder systems (phone, mail & electronic) • Outcomes and cost assessment
Case Management • Patient tracking systems • Check to see if recommended ‘process of care’ is occurring as part of good quality care. • Patient reminder systems (mail) • Provider reminder systems (phone, mail & electronic) • Outcomes and cost assessment
 Utilization Review / Demand Management • Either run directly or contracted to 4 th party acting as Insurer’s agent. • Have decision-support systems based on clinical algorithms (and possibly patient’s claims) to manage a patient’s care. • Common conditions reviewed/managed: – Schizophrenia, depression – Heart disease – Diabetes, Asthma, Glaucoma – AIDS
Utilization Review / Demand Management • Either run directly or contracted to 4 th party acting as Insurer’s agent. • Have decision-support systems based on clinical algorithms (and possibly patient’s claims) to manage a patient’s care. • Common conditions reviewed/managed: – Schizophrenia, depression – Heart disease – Diabetes, Asthma, Glaucoma – AIDS
 Support Databases • Procedure fee schedules • Diagnosis codes • Institutional arrangements for managed care payment • Pharmacy fee schedules and formularies • ‘Grouper’ algorithms – DRGs, MDCs, – Case-mix and severity
Support Databases • Procedure fee schedules • Diagnosis codes • Institutional arrangements for managed care payment • Pharmacy fee schedules and formularies • ‘Grouper’ algorithms – DRGs, MDCs, – Case-mix and severity
 Life Support Systems • Accounts Receivable – Employers – Consumers – Government • Claims payment – Error checking – Provider payment – Fee schedules & payment algorithms • Benefits/eligibility
Life Support Systems • Accounts Receivable – Employers – Consumers – Government • Claims payment – Error checking – Provider payment – Fee schedules & payment algorithms • Benefits/eligibility
 Analytic / Financial Data • ‘Cleaned’ versions of claim, provider and membership files designed to: – Generate premium estimates – Adjust provider fee schedules – Profiling of: • • population (e. g. , all patients with diabetes) practices employer groups patients
Analytic / Financial Data • ‘Cleaned’ versions of claim, provider and membership files designed to: – Generate premium estimates – Adjust provider fee schedules – Profiling of: • • population (e. g. , all patients with diabetes) practices employer groups patients
 • What ‘information’ can") Small Group Exercises (Part 1 of a 2 Part Exercise) • What ‘information’ can health insurance data provide? • Name 2 major strengths and weaknesses of claims data as a management tool. • Poof: You’re a Blue Cross Blue Shield CIO. – You have $50 M to spend to upgrade your claims system. – It costs $1 M per text/character to enhance your data. – What data fields would you add? – Are there any data fields you would consider deleting or optimizing?
Small Group Exercises (Part 1 of a 2 Part Exercise) • What ‘information’ can health insurance data provide? • Name 2 major strengths and weaknesses of claims data as a management tool. • Poof: You’re a Blue Cross Blue Shield CIO. – You have $50 M to spend to upgrade your claims system. – It costs $1 M per text/character to enhance your data. – What data fields would you add? – Are there any data fields you would consider deleting or optimizing?
 Intermission
Intermission
 Medical Provider Data • • • Patient Diagnosis Information Treatment plan Referrals Outcomes Explanations for treatment
Medical Provider Data • • • Patient Diagnosis Information Treatment plan Referrals Outcomes Explanations for treatment
 The Operation • The Hospital submits lots of bills – – – Lab work Blood Anesthesia ER room time Supplies • Surgeon John submits a claim for surgery. • Dr. Bob submits a claim for IP consultation. • Internal hospital systems affected: – – Inventory Payroll Accounts receivable Medical records • PPO reimburses hospital. • PPO reimburses Dr. Bob • PPO reimburses Dr. John
The Operation • The Hospital submits lots of bills – – – Lab work Blood Anesthesia ER room time Supplies • Surgeon John submits a claim for surgery. • Dr. Bob submits a claim for IP consultation. • Internal hospital systems affected: – – Inventory Payroll Accounts receivable Medical records • PPO reimburses hospital. • PPO reimburses Dr. Bob • PPO reimburses Dr. John
 Medical Center Data Systems Life Support Data Hardware
Medical Center Data Systems Life Support Data Hardware
 Medical Data Collection - 1 • Operational data: Transaction-oriented – Hospital pharmacies – Laboratories – Radiology departments – Critical care units – Order-processing units
Medical Data Collection - 1 • Operational data: Transaction-oriented – Hospital pharmacies – Laboratories – Radiology departments – Critical care units – Order-processing units
 Medical Data Collection - 2 • Analytic data – Carry all variables of interest – Single record – Data is stored horizontally
Medical Data Collection - 2 • Analytic data – Carry all variables of interest – Single record – Data is stored horizontally
 Code Systems Standards - 1 • HL 7 - American National Standards Institute Health Level – Patient registration data – Patient orders – Clinical information (e. g. , vital signs) – Referral information – Clinical trial data – Other operational transactions
Code Systems Standards - 1 • HL 7 - American National Standards Institute Health Level – Patient registration data – Patient orders – Clinical information (e. g. , vital signs) – Referral information – Clinical trial data – Other operational transactions
 Code Systems Standards - 2 • X 12 - Data Interchange Standards Association’s Accredited Standards Committee – Insurance enrollment & payment – Administrative messages
Code Systems Standards - 2 • X 12 - Data Interchange Standards Association’s Accredited Standards Committee – Insurance enrollment & payment – Administrative messages
 Code Systems Standards - 3 • Diagnoses: International Classification of Diseases, Version 9 (ICD 9) • Procedures: Current Procedural Terminology, Version 4 (CPT 4) • Drugs: Food and Drug Administration’s Nation Drug Code (NDC) directory
Code Systems Standards - 3 • Diagnoses: International Classification of Diseases, Version 9 (ICD 9) • Procedures: Current Procedural Terminology, Version 4 (CPT 4) • Drugs: Food and Drug Administration’s Nation Drug Code (NDC) directory
 Code Systems Standards - 4 • LOINC - Logical Observations Identifier Names and Codes (LOINC) database: The Missing Link – Codes, names and synonyms for more than 12, 000 observations: • • • laboratory tests vital signs electrocardiograph measurement input & output measures clinical impressions discharge summary
Code Systems Standards - 4 • LOINC - Logical Observations Identifier Names and Codes (LOINC) database: The Missing Link – Codes, names and synonyms for more than 12, 000 observations: • • • laboratory tests vital signs electrocardiograph measurement input & output measures clinical impressions discharge summary
 Code Systems Standards Examples
Code Systems Standards Examples
 Integrated Delivery System IT Network Decision Support Life Support Data Hardware
Integrated Delivery System IT Network Decision Support Life Support Data Hardware
 Insurer Only Data 1/31/09 PCP visit Laboratory test Specialist visit Biopsy Surgery Sub-Acute Care 2/6/09
Insurer Only Data 1/31/09 PCP visit Laboratory test Specialist visit Biopsy Surgery Sub-Acute Care 2/6/09
 Medical Data Available to a U. S. Fee-for-Service Insurer Decision Support Life Support Data Hardware
Medical Data Available to a U. S. Fee-for-Service Insurer Decision Support Life Support Data Hardware
 Medical Data Available to a U. S. Staff Model HMO Decision Support Life Support Data Hardware
Medical Data Available to a U. S. Staff Model HMO Decision Support Life Support Data Hardware
 Provider Only Data 1/31/09 Referral to specialist White blood cell count high Cancer metastasized Malignant cancer remains 2/6/09
Provider Only Data 1/31/09 Referral to specialist White blood cell count high Cancer metastasized Malignant cancer remains 2/6/09
 E/CPR Model A
E/CPR Model A
 E/CPR Model B
E/CPR Model B
 What are the Pros & Cons of these Models? Are they out of date as useful data management models?
What are the Pros & Cons of these Models? Are they out of date as useful data management models?
 Data Available to the Average Medical Provider About a Patient’s Care 10% of Care 25% of Care 15% of Care 35% of Care
Data Available to the Average Medical Provider About a Patient’s Care 10% of Care 25% of Care 15% of Care 35% of Care
 Merging Insurer & Provider Data 1/31/09 PCP visit Referral to specialist Laboratory test Specialist visit White blood cell count high Biopsy Cancer metastasized Surgery Malignant cancer remains Sub-Acute Care 2/6/09
Merging Insurer & Provider Data 1/31/09 PCP visit Referral to specialist Laboratory test Specialist visit White blood cell count high Biopsy Cancer metastasized Surgery Malignant cancer remains Sub-Acute Care 2/6/09
 • What ‘information’ can") Small Group Exercises (Part 1 of a 2 Part Exercise) • What ‘information’ can health insurance data provide? • Name 2 major strengths and weaknesses of claims data as a management tool. • Poof: You’re a Blue Cross Blue Shield CIO. – You have $50 M to spend to upgrade your claims system. – It costs $1 M per text/character to enhance your data. – What data fields would you add? – Are there any data fields you would consider deleting or optimizing?
Small Group Exercises (Part 1 of a 2 Part Exercise) • What ‘information’ can health insurance data provide? • Name 2 major strengths and weaknesses of claims data as a management tool. • Poof: You’re a Blue Cross Blue Shield CIO. – You have $50 M to spend to upgrade your claims system. – It costs $1 M per text/character to enhance your data. – What data fields would you add? – Are there any data fields you would consider deleting or optimizing?
 • What ‘information’ can") Small Group Exercises (Part 2 of a 2 Part Exercise) • What ‘information’ can medical data provide? • If you are an insurance company CEO, how vital are clinical medical records to your business? • If you are hospital administrator, name one pro and one con to having access to health insurance data? What share of your profit/surplus are you willing to invest for such a link?
Small Group Exercises (Part 2 of a 2 Part Exercise) • What ‘information’ can medical data provide? • If you are an insurance company CEO, how vital are clinical medical records to your business? • If you are hospital administrator, name one pro and one con to having access to health insurance data? What share of your profit/surplus are you willing to invest for such a link?