01f975ac661c808c374673c8ee0b3e70.ppt
- Количество слайдов: 52


: What are we learning from our")
Type 1 Diabetes Exchange (T 1 D Exchange): What are we learning from our type 1 diabetes kids and families? Beth A. Olson, BAN, RN, CDE Program Manager International Diabetes Center

T 1 D Exchange Mission and Goals Improve outcomes of people touched by T 1 D by facilitating better care and accelerating new therapies through a collaborative data collection and sharing network. A Helmsley Charitable Trust Initiative

What is the T 1 D Exchange? Clinic Registry Biobank Patient

Clinic Registry Objectives Collect clinical and laboratory data on a large number of patients with type 1 diabetes to: • Address pertinent clinical issues • Conduct exploratory/hypothesis-generating analyses • Identify patients interested in being contacted about participating in research studies • Categorize patients for future clinical studies and biobank analyses

T 1 D Exchange Clinic Network and Registry 67 Clinics – 25, 000+ patients with T 1 D

Clinic Registry Data Collection Data collected at enrollment and then annually • Informed consent obtained • Two-thirds of data obtained directly from participant’s completion of a questionnaire • One-third from medical records/clinic database

Characteristics of Participants

T 1 D Exchange: Age, Duration, Weight 07 -01 -12

T 1 D Exchange: Monitoring, Insulin Delivery 07 -01 -12

SMBG and A 1 C • In recent years state insurance plans have questioned whether or not sufficient evidence is available to justify coverage of self-monitoring of blood glucose (SMBG) for children with T 1 D.

Study Question Is Frequency of Self Blood Glucose Monitoring Related to A 1 c?

Purpose To examine the relationship between the number of times SMBG is performed per day and Hb. A 1 C among participants < 18 years of age in the T 1 D Exchange Clinic Registry.

Figure 2. Mean Hb. A 1 c Across Number of Self. Reported SMBG Per Day Stratified by Age Group (Excluding CGM Users) 10. 5% 10. 41% 0 -5 Years Old (N=267, p=0. 01) 10. 14% 10. 0% 6 -12 Years Old (N=2158, p < 0. 001) Mean Hb. A 1 c 13 -17 Years Old (N=2295, p < 0. 001) 9. 5% 9. 0% 9. 26% 9. 44% 8. 93% 8. 63% 8. 78% 8. 62% 8. 40% 8. 5% 8. 22% 8. 09% 8. 19% 7. 88% 7. 89% 7. 5% 7. 49% 7. 0% 0 -2 3 -4 5 -6 7 -9 ≥ 10 Number of Self-Reported SMBG per Day

T 1 D Exchange: Hb. A 1 c and SMBG 07 -01 -12

Association between Frequency of SMBG per Day and Hb. A 1 c by Age

Association between Frequency of SMBG per Day and Hb. A 1 c by Age and Insulin Delivery

Current Treatment of Childhood T 1 D The Aim: • To achieve and maintain blood glucose and Hb. A 1 c levels as close to normal as possible to delay and prevent the longterm complications of T 1 D

Current Treatment of Childhood T 1 D The Reality: • Mean Hb. A 1 c levels are 8. 3% for preteens and 8. 7% for teens in the US based on data from T 1 D Exchange Clinic Registry, 2012

Are Most Persons with T 1 D Meeting A 1 C Recommendations?

Proportion meeting Hb. A 1 c targets A 1 c Goal = <7. 0% A 1 c Goal= <8. 5% A 1 c Goal= <8. 0% A 1 c Goal= <7. 5%

T 1 D Exchange Clinic Registry Top 10 Findings 2012 -2013

Top 10 Findings 1. Most adults and children with T 1 D do not achieve Hb. A 1 c goals set by ADA 2. Adolescents and young adults with T 1 D have worse glucose control and are at higher risk for DKA than younger or older individuals with T 1 D. 3. Individuals with excellent glycemic control tend to manage their diabetes differently than those with poorer control 4. Frequency of home glucose monitoring is strongly associated with lower Hb. A 1 c levels

Adults and Children with Excellent vs Poor Glycemic Control Can you guess how the excellent control group differed from the poor control group in the T 1 D Exchange Clinic Registry?

Self-Monitoring of Blood Glucose

Bolusing Before a Meal

Insulin: Carb Ratios

Insulin Pump Use

Never Miss Insulin Doses

Study Questions • How often do you think insulin doses are omitted? • What is the impact of missed insulin doses on glycemic control?

Proportion of Participants Who Missed an Insulin Dose at least Once per Week by Age

Mean A 1 c by Missed Insulin Frequency and Age Mean A 1 c 7. 9% vs 9. 0% N=19, 908

Clinical Practice Case Study u u u 3 year old boy on multiple daily injections Parents are skilled at carb counting Finicky eater, eats frequently, challenging to predict food intake in advance Parents are giving injections after food to avoid chasing insulin with juice/candy Missed insulin doses or mismatch with timing of insulin and BG levels Problem Solving

Clinical Practice Case Study u u u 8 year old girl on multiple daily injections Single parent facing multiple challenges Frequently misses long-acting insulin A 1 c 9. 8% School nurse knowledgeable about T 1 D and family situation Problem Solving

Top 10 Findings 5. Severe hypoglycemia resulting in seizure or loss of consciousness occurs more commonly in older adults with longstanding T 1 D than has been appreciated. 6. In both children and adults, the frequency of severe hypoglycemia is not higher with tight glucose control vs poorer control in contrast to the findings of the DCCT 7. DKA does not occur any more frequently in insulin pump users than injection users

DCCT Findings 12 120 Severe Hypoglycemia 10 8 6 60 Relative risk of retinopathy 4 2 0 0 5. 5 6 6. 5 7 7. 5 8 8. 5 9 Hb. A 1 c (%) 9. 5 10 10. 5 0 Rate of severe hypoglycaemia (per 100 patient years) Rate pf progression of retinopathy (per 100 patient years) Lower Hb. A 1 C = Fewer Complications BUT More Hypo

Severe Hypoglycemia 07 -01 -12

DKA Insulin Delivery Method *Pump defined as ≥ 1 year of pump use

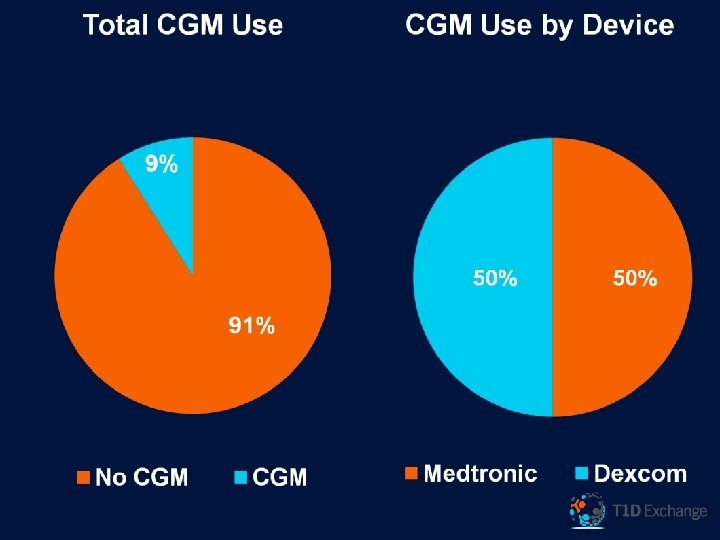
Top 10 Findings 8. The frequency of microalbuminuria in children, adolescents and young adults is strongly associated with glycemic control, T 1 D duration, and blood pressure. 9. Racial disparities exist in insulin pump use and Hb. A 1 c levels, even after adjusting for socio-economic status 10. CGM is used by only a small percentage of individuals with T 1 D. Among individuals who have used CGM, twothirds stopped using it.

Microalbuminuria by Hb. A 1 c and T 1 D Duration in Children and Young Adults

Pump use According to Race/Ethnicity and Income Among Youth <18 yo
 impacts Diabetes Management and Glycemic Control among Adolescents and")
Attention Deficit Hyperactivity Disorder (ADHD) impacts Diabetes Management and Glycemic Control among Adolescents and Young Adults with Type 1 Diabetes (T 1 D)

Missed Insulin Dose at Least 1 Time/Week

Mean Hb. A 1 c 45

Frequency of ≥ 1 DKA and SH Event in Past 3 Months

Summary • ADHD adversely affects diabetes management and clinical outcomes. • Participants taking medication for ADHD were less likely to have poor glycemic outcomes compared with pts not on meds • Further assessment of glycemic control in patients with ADHD, with and without treatment, is warranted

Clinical Practice Case Study u Situation: u 19 year old boy on insulin pump u On pump download, total daily dose is 80% basal; 20% bolus u Complains of poor appetite u Fear of hypoglycemia u A 1 c 10. 3% u Strategy: What are your options?

• Slide Title bill Courtesy of William Tamborlane, MD

Interest in Future Studies Email address provided

QUESTIONS?
01f975ac661c808c374673c8ee0b3e70.ppt