71a82a532fd74a55c6c6cebfc69f7757.ppt
- Количество слайдов: 45



Two Intimate Epidemics: Peripubertal Obesity and Polycystic Ovarian Syndrome BY Professor Mohammad Emam OB & GYN Dept. Mansoura Faculty of Medicine. Egypt 2007
 Peripubertal obesity( PPO):")
Definitions Obesity is: excessive storage of triglycerides in adipose cells. (Adipocytes) Peripubertal obesity( PPO): comprises childhood and adolescent obesity.

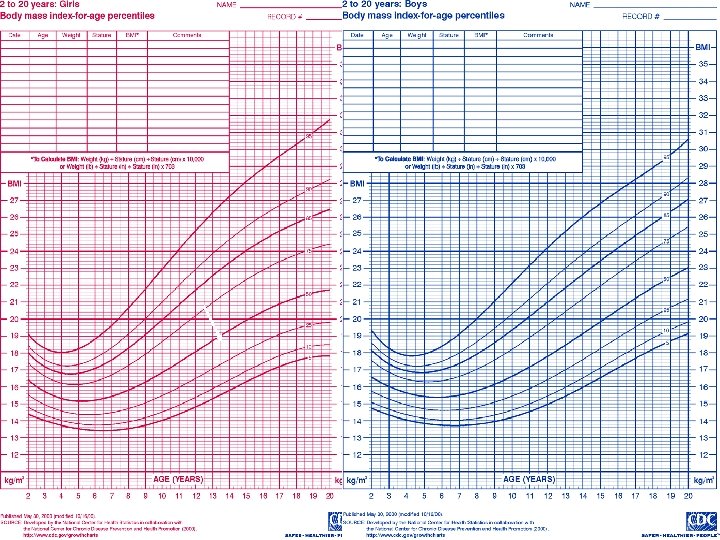
Definitions For children, § overweight = BMI 85 th to 95 th percentile for age § Obese= Above 95 th percentile for age. For adolescent and adults, § BMI > 25 = overweight § BMI > 30 = obese, § BMI > 40 = morbidly obese
 Two of the following three features are present, after")
Definition PCOS ( After 2003) Two of the following three features are present, after exclusion of other etiologies : (i) Oligomenorrhoea and or Anovulation (ii) Hyperandrogenism and/or hyperandrogenemia. (iii) Polycystic ovaries (sonar).

RATIONALE Peripubertal obesity : § Is associated with medical and psychosocial co-morbidities that are both immediate and long-term. PCOS: § Is one of the co-morbidities and sequelae of Peripubertal obesity. § An emerging epidemic especially in developing countries. Prevention of Peripubertal obesity is the first line for prevention of PCOS.

Objective: To illustrate the link between two current epidemics , Peripubertal obesity and PCOS. To pinpoint the role of gynecologists regarding these two epidemics.

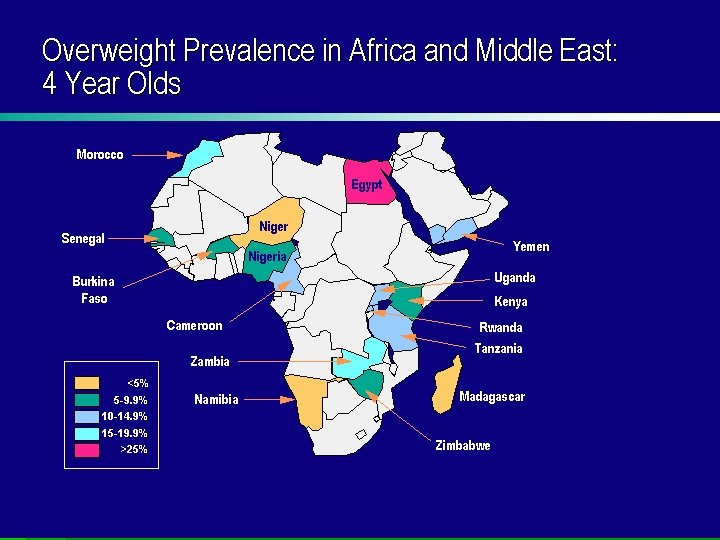
Peripubertal obesity Prevalence In USA : doubled in 6 -12 year. § tripled in adolescents. § 15% of 6 -19 year are obese. In different countries : § Range from ( 10% to 25%). §

Childhood Obesity Epidemic Source: National Center for Health Statistics, 1999 National Health and Nutrition Examination Survey.

MORE THAN 1 IN 4 CHILDREN IS OVERWEIGHT or OBESE!!

Peripubertal obesity -A true epidemic Obesity is now 4 X more common than malnutrition in developing countries. Obesity would surpass tobacco as leading cause of death.

Peripubertal obesity -A true Epidemic The current epidemic is due to interactions between genetic , epigenetic and environmental factors : Increased sedentary life § Decrease in physical activity. §Increased energy intake §

Causes of Childhood Obesity Genetics Cultural Neuroendocrine Childhood obesity Behavioral Socioeconomic

Obesity Is Caused by Long-Term Positive Energy Balance Fat Stores

Peripubertal obesity Weight gain: Energy In Energy Out

§Snacking as a food trend has increased in children over the past two decades.

Swollen Food Over the last 2 decades, almost every food portion has swollen. 210 Calories 2. 4 ounces 610 Calories 6. 9 ounces

Soft Drinks Become part of the daily diet for many school age children. Leads to a higher daily energy intake and reduced intakes of some essential nutrients
 Create Talk Snack More Relate Talk Buy More")
TV and Computer ( Sedentary behavior) Create Talk Snack More Relate Talk Buy More TV TV Eat More Imagine Run Sit More Play Read


Some Interesting Results TV & computer= Main culprit for energy imbalance. Healthy Kids Watch Less TV. Sedentary children are more likely to be obese.

Consequences of Peripubertal obesity later in life Psychosocial Poor self-esteem Depression Eating disorders Pulmonary Sleep Apnea Asthma Exercise Intolerance Gastrointestinal Gallstones Steatohepatitis Neurological Pseudotumor cerebri Cardiovascular Dyslipidemia (hypercholesterolemia and (hypertriglyceridemia) Hypertension Coagulopathy Chronic inflammation Endothelial dysfunction Renal Glomerulosclerosis Musculoskeletal Slipped capital femoral epiphysis Blount’s disease Forearm fracture Flat feet Endocrine Type 2 Precocious puberty Polycystic ovary syndrome (girl) Hypogonadism (boys)
 Metabolic Syndrome. Hypertension Fatty Liver. Liability")
Sequelae Specific to Children ( Disease of Diseases) Metabolic Syndrome. Hypertension Fatty Liver. Liability for PCOS at adolescence. Early Sexual Maturation. Asthma Sleep apnea

Sequelae Specific to Children … cont Persistence of Obesity at Adulthood: § Overweight adolescents have a 70% chance of becoming overweight adults. § Increases to 80% if one or both parents are obese. Obese 6 year old has a 25% chance of becoming obese adult Obese 12 year old has a 75% chance of becoming a obese adult.

PCOS : An Epidemic About 20% of reproductive age women demonstrate the ultrasound picture of polycystic ovaries. About 5 - 10 % have clinical or biochemical signs of Anovulation androgen excess. PCOS, starts in adolescence But Unfortunately not always diagnosed at that age ,

PCOS : An Epidemic Caused by Complex interaction of genetic , epigenetic and environmental factors. An epidemic in developing countries ( ED & PCOS !!!!).

Link between Peripubertal obesity & PCOS Peripubertal obesity PCOS IR & ghrelin & Leptin & Fat, steroid

Prevalence Of Insulin Resistance Syndrome In PCOS Affects 2/3 of the PCOS women

Prevalence Of Insulin Resistance Syndrome In Childhood obesity §Prevalence about 28% (Cook et al, 2003 & de Ferranti et al. , 2004)
 Pregnancy Genetics Aging Drugs Insulin Resistance Hyperinsulinemia")
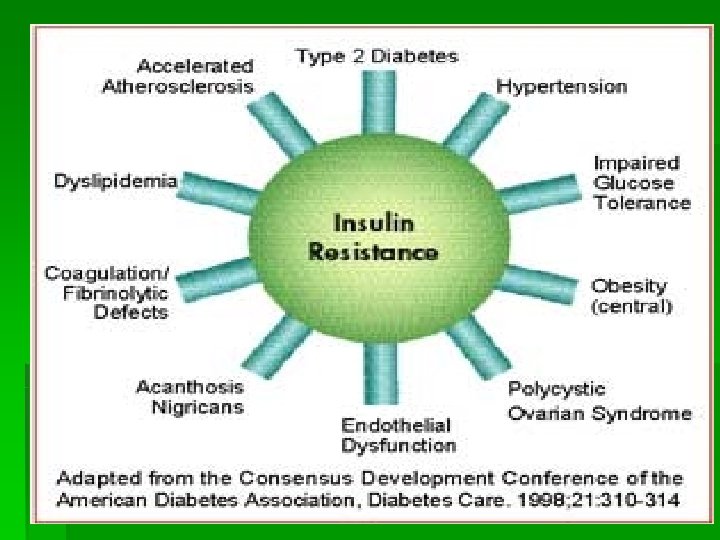
The Central Player ( Insulin Resistance ) Pregnancy Genetics Aging Drugs Insulin Resistance Hyperinsulinemia Lifestyle obesity Increased lipid storage PCOS Altered steroid hormone metabolism Altered lipoprotein & cholesterol metabolism

IR : The central paradox §The high ovarian response to insulin. §Opposed by the whole body resistance.
 is 167 AA peptide secreted by adipocytes and circulates")
LEPTIN Leptin (leptos = thin) is 167 AA peptide secreted by adipocytes and circulates in blood. Blood levels proportional to total fat mass. Exerts a specific action on steroidogenesis and follicular maturation in ovary. Effects: - appetite inhibition - effects on GH-RH and Gn. RH
 A peptide 28 AA peptide. Secreted by gastric mucosa on an")
GHRELIN (orexigenic effects) A peptide 28 AA peptide. Secreted by gastric mucosa on an empty stomach. Fasting GHRELIN level in most obese are lower than in non obese. § APPETITE FOOD INTAKE § FAT UTILIZATION IN OBESITY, GHRELIN level . OVERPRODUCTION OBESITY

GHRELIN & Leptin antagonism The satiety effect of leptin is abolished by co-injection of ghrelin leptin / ghrelin antagonism.

Role of Gynecologist Management of PCOS should start by early intervention in hi-risk peripubertal kids by prevention of obesity. Prevention of peripubertal obesity: § Primary prevention is vital. § secondary prevention: § Effective treatment programs for children and adolescent who are already overweight.
 § Dietetics § Physical activity")
approach For prevention Cooperation between : § Medical (pediatric) § Dietetics § Physical activity § Psychological / socialogical

Primary Prevention Achieving equilibrium of the energy balance. § Energy input = Energy loss. . FOOD INTAKE ENERGY EXPENDITURE
 Surgery Pharmacotherapy Lifestyle Modification Diet Physical Activity")
Secondary Prevention (Obesity Treatment Pyramid) Surgery Pharmacotherapy Lifestyle Modification Diet Physical Activity

Secondary prevention Life- style modifications: Diet modification Weight loss Exercise Psychosocial support. üImprove IR ( Metformin)

Conclusions We are facing two current epidemics which affect a large scale of population and also affect their reproductive future. Childhood Obesity is a Public Health Perspective

Recommendations: We recommend cooperation of multifaceted, large-scale interventions for Prevention of peripubertal obesity : § Dietary modification. § Increased physical activity. § Decreased sedentary activity. § Behavior modification.

OB& GYN, Mansoura Faculty of Medicine EGYPT Telfax 0020502319922 & 0020502312299 Email. mae 335@hotmail. com
71a82a532fd74a55c6c6cebfc69f7757.ppt