

e40b5facd5bc681b563bd81637e79e46.ppt
- Количество слайдов: 26
 Travelers’ Health April 2004 Dr. Tim Cook
Travelers’ Health April 2004 Dr. Tim Cook
 USEFUL WEBSITES Health Canada http: //www. hc-sc. gc. ca/pphb-dgspsp/tmp-pmv/index. html CDC Travelers' Health http: //www. cdc. gov/travel/ Morbidity and Mortality Weekly Report http: //www. cdc. gov. mmwr/
USEFUL WEBSITES Health Canada http: //www. hc-sc. gc. ca/pphb-dgspsp/tmp-pmv/index. html CDC Travelers' Health http: //www. cdc. gov/travel/ Morbidity and Mortality Weekly Report http: //www. cdc. gov. mmwr/
 CASE Healthy recently graduated physician joins MSF and immediately deploys to CAR (Central African Republic) What health risk mitigation information should he be given? Vaccines? Rx?
CASE Healthy recently graduated physician joins MSF and immediately deploys to CAR (Central African Republic) What health risk mitigation information should he be given? Vaccines? Rx?
 INFECTIOUS VECTOR-BORNE DISEASE MALARIA DENGUE FEVER NEMATODES • FILARIASIS, ONCHOCERCIASIS, LOAIASIS TRYPANOSOMIASIS YELLOW FEVER RICKETTSIAE (Ticke-borne) (JAPANESE ENCEPHALITIS – not in Africa)
INFECTIOUS VECTOR-BORNE DISEASE MALARIA DENGUE FEVER NEMATODES • FILARIASIS, ONCHOCERCIASIS, LOAIASIS TRYPANOSOMIASIS YELLOW FEVER RICKETTSIAE (Ticke-borne) (JAPANESE ENCEPHALITIS – not in Africa)
 DEET 28% lasts 6 -8 hours 6% lasts < 1") PPM (PERSONAL PROTECTION MEASURES) DEET 28% lasts 6 -8 hours 6% lasts < 1 hr 95% no longer available Slow-release better (Ultrathon, Sawyer’s) LONG SLEEVES, PANTS BEDNETS (Permethrin-impregnated)
PPM (PERSONAL PROTECTION MEASURES) DEET 28% lasts 6 -8 hours 6% lasts < 1 hr 95% no longer available Slow-release better (Ultrathon, Sawyer’s) LONG SLEEVES, PANTS BEDNETS (Permethrin-impregnated)
 Daily, day before until 1 wk after departing") MALARIA CHEMOPROPHYLAXIS MALARONE (Atovaquone + Proguanil) Daily, day before until 1 wk after departing S/E Mild GI, Head. Aches Safe in aircrew, drivers etc. EXPENSIVE ($5/DAY) MEFLOQUINE DOXYCYCLINE PRIMAQUINE
MALARIA CHEMOPROPHYLAXIS MALARONE (Atovaquone + Proguanil) Daily, day before until 1 wk after departing S/E Mild GI, Head. Aches Safe in aircrew, drivers etc. EXPENSIVE ($5/DAY) MEFLOQUINE DOXYCYCLINE PRIMAQUINE
 DENGUE Throughout tropics Day biting Aedes Egypti mosquito therefore use DEET night AND day No vaccine (yet!) PPM only
DENGUE Throughout tropics Day biting Aedes Egypti mosquito therefore use DEET night AND day No vaccine (yet!) PPM only
 INFECTIOUS HUMAN-BORNE TB – two step Mantoux recommended STDs incl Hep B / HIV Influenza • yr round in tropics Meningococcus
INFECTIOUS HUMAN-BORNE TB – two step Mantoux recommended STDs incl Hep B / HIV Influenza • yr round in tropics Meningococcus
 • Non-typhoid salmonella ETEC – commonest cause of") INFECTIOUS FOOD / WATER-BORNE Typhoid (salmonella) • Non-typhoid salmonella ETEC – commonest cause of travelers’ diarrhea • Toxin = secretory diarrhea Cholera – similar toxin as ETEC Other bacteria (shigella / campylobacter / yersinia Virus - Hepatitis A (Norwalk, Rota) less common Parasites (E. Histolytica, Cyclospora , Cryptosporidia) <3% of TD but more common in persistent diarrhea Schistosomiasis – DON’T SWIM IN FRESHWATER
INFECTIOUS FOOD / WATER-BORNE Typhoid (salmonella) • Non-typhoid salmonella ETEC – commonest cause of travelers’ diarrhea • Toxin = secretory diarrhea Cholera – similar toxin as ETEC Other bacteria (shigella / campylobacter / yersinia Virus - Hepatitis A (Norwalk, Rota) less common Parasites (E. Histolytica, Cyclospora , Cryptosporidia) <3% of TD but more common in persistent diarrhea Schistosomiasis – DON’T SWIM IN FRESHWATER
 Q fever (rickettsia) Brucellosis Tularemia Rabies Many others ALL") INFECTIOUS ZOONOSES (Animal – borne) Q fever (rickettsia) Brucellosis Tularemia Rabies Many others ALL RARE
INFECTIOUS ZOONOSES (Animal – borne) Q fever (rickettsia) Brucellosis Tularemia Rabies Many others ALL RARE
 Climb high, sleep low,") NON-INFECTIOUS FLORA FAUNA …. AVOID! ACCLIMATIZATION ALTITUDE SICKNESS (hikes Kilimanjaro!) Climb high, sleep low, go slow Acetazolamide (Diamox) 250 mg OD • Carbonated beverages taste flat! • Does not prevent HAPE, HACE – emergent descent or pressure bag, O 2, steroids, nifedipine, supportive care NEEDLE STICK INJURY (Bring triple therapy? )
NON-INFECTIOUS FLORA FAUNA …. AVOID! ACCLIMATIZATION ALTITUDE SICKNESS (hikes Kilimanjaro!) Climb high, sleep low, go slow Acetazolamide (Diamox) 250 mg OD • Carbonated beverages taste flat! • Does not prevent HAPE, HACE – emergent descent or pressure bag, O 2, steroids, nifedipine, supportive care NEEDLE STICK INJURY (Bring triple therapy? )
 VACCINES? ROUTINE RECOMMENDED REQUIRED
VACCINES? ROUTINE RECOMMENDED REQUIRED
 ROUTINE VACCINES Td. P MMR
ROUTINE VACCINES Td. P MMR
 RECOMMENDED HEPATITIS A – 2 doses, > 10 yrs HEPATITIS B – 3 doses, > 10 yrs TWINRIX – both A & B, 3 doses INFLUENZA – annually / pre-travel TYPHOID Typhum Vi – 1 dose, lasts 3 yrs, 75% effective Vivotif – oral, 4 doses, lasts 5 yrs, similar efficacy RABIES MENINGOCOCCUS
RECOMMENDED HEPATITIS A – 2 doses, > 10 yrs HEPATITIS B – 3 doses, > 10 yrs TWINRIX – both A & B, 3 doses INFLUENZA – annually / pre-travel TYPHOID Typhum Vi – 1 dose, lasts 3 yrs, 75% effective Vivotif – oral, 4 doses, lasts 5 yrs, similar efficacy RABIES MENINGOCOCCUS
 Oral vaccine against toxin of ETEC and cholera 2 doses") DUKORAL New (Aug 2003) Oral vaccine against toxin of ETEC and cholera 2 doses 1 wk apart ~75% effective Only lasts 3 months $$ (75)
DUKORAL New (Aug 2003) Oral vaccine against toxin of ETEC and cholera 2 doses 1 wk apart ~75% effective Only lasts 3 months $$ (75)
") REQUIRED YELLOW FEVER MENINGOCOCCUS (only req’d for participation in the Hajj, travel to Mecca)
REQUIRED YELLOW FEVER MENINGOCOCCUS (only req’d for participation in the Hajj, travel to Mecca)
 YELLOW FEVER monkey zoonosis transmitted to humans by mosquitoes Classic (but more severe than ususal) clinical manifestations: Fever, headache, abdo pain and vomiting; Short period of improvement; Then liver and kidney failure, shock +/- bleeding
YELLOW FEVER monkey zoonosis transmitted to humans by mosquitoes Classic (but more severe than ususal) clinical manifestations: Fever, headache, abdo pain and vomiting; Short period of improvement; Then liver and kidney failure, shock +/- bleeding
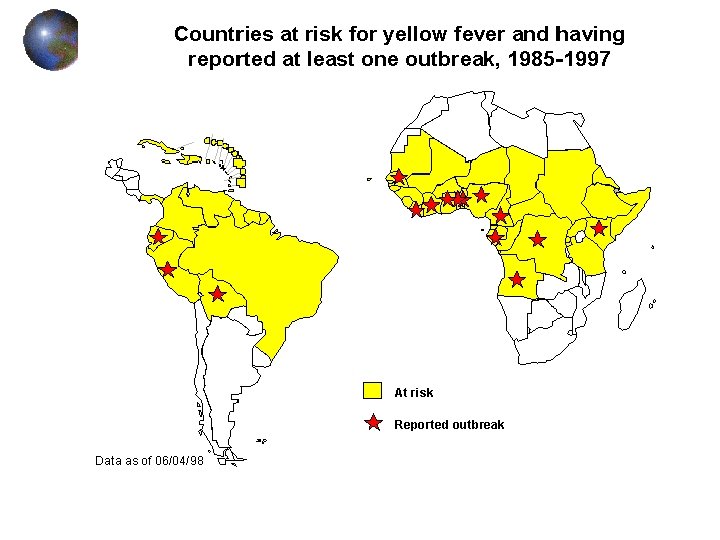
 YELLOW FEVER CONT’D certain countries require vaccination for entry live attenuated virus; may be safe in asymptomatic HIV; patients should be given choice single dose if egg anaphylaxis, two options: Intradermal skin testing with the vaccine Letter documenting contraindication --> waiver from embassy
YELLOW FEVER CONT’D certain countries require vaccination for entry live attenuated virus; may be safe in asymptomatic HIV; patients should be given choice single dose if egg anaphylaxis, two options: Intradermal skin testing with the vaccine Letter documenting contraindication --> waiver from embassy
 TYPHOID most important in Indian subcontinent use in travellers going outside of tourist areas or to places with known typhoid epidemics capsular polysaccharide vaccine; single injection MENINGOCOCCUS frequent epidemics in sub-Saharan Africa (belt across the middle of the continent from Guinea to Ethiopia); patient at risk if there >3 weeks or not staying in hotels risk in pilgrims going to Mecca for the hajj single dose to these travellers 10 - 14 days pretravel
TYPHOID most important in Indian subcontinent use in travellers going outside of tourist areas or to places with known typhoid epidemics capsular polysaccharide vaccine; single injection MENINGOCOCCUS frequent epidemics in sub-Saharan Africa (belt across the middle of the continent from Guinea to Ethiopia); patient at risk if there >3 weeks or not staying in hotels risk in pilgrims going to Mecca for the hajj single dose to these travellers 10 - 14 days pretravel
 HEPATITIS A fecal to oral prevalent in MANY countries; all of Africa and South America, SE Asia 0. 3% per month risk of infection in developing countries if patient is careful where they eat vaccine is inactivated virus safe, very effective protection after four weeks booster in 6 - 12 months (depending on formulation) can use Immune Globulin for prophylaxis in patients who can’t be vaccinated NOTE: other major indication for HAV vaccine is all patients with chronic liver disease
HEPATITIS A fecal to oral prevalent in MANY countries; all of Africa and South America, SE Asia 0. 3% per month risk of infection in developing countries if patient is careful where they eat vaccine is inactivated virus safe, very effective protection after four weeks booster in 6 - 12 months (depending on formulation) can use Immune Globulin for prophylaxis in patients who can’t be vaccinated NOTE: other major indication for HAV vaccine is all patients with chronic liver disease
 Japanese encephalitis mosquito-borne arbovirus important in late summer -- autumn in much of East Asia except urban China/Japan or Singapore consider in patients going in Summer/Fall, esp. to rural areas or for a prolonged stay in urban areas three doses over the course of a month Measles if born after 1970, with no proof of vaccination, if travelling to endemic area
Japanese encephalitis mosquito-borne arbovirus important in late summer -- autumn in much of East Asia except urban China/Japan or Singapore consider in patients going in Summer/Fall, esp. to rural areas or for a prolonged stay in urban areas three doses over the course of a month Measles if born after 1970, with no proof of vaccination, if travelling to endemic area
 PRESCRIPTIONS ANTI-MALARIAL STANDBY FOR TRAVELERS’ DIARRHEA Azithromycin – 1 g all at once Cipro – 1 g at once Acetazolamide
PRESCRIPTIONS ANTI-MALARIAL STANDBY FOR TRAVELERS’ DIARRHEA Azithromycin – 1 g all at once Cipro – 1 g at once Acetazolamide
 CASE 2 2 days after returning to Canada the physician calls you complaining that he has a fever (38. 5) and some diarrhea? What are your recommendations?
CASE 2 2 days after returning to Canada the physician calls you complaining that he has a fever (38. 5) and some diarrhea? What are your recommendations?
 FEVER IN RETURNING TRAVELER MALARIA, MALARIA DENGUE TYPHOID “DEVELOPED WORLD DISEASES” INFLUENZA, PNEUMONIA, UTI etc
FEVER IN RETURNING TRAVELER MALARIA, MALARIA DENGUE TYPHOID “DEVELOPED WORLD DISEASES” INFLUENZA, PNEUMONIA, UTI etc
 WHAT TO DO? Consider it a medical emergency! CBC (anemia, thrombocytopenia in malaria and dengue) Thick and thin smears (malaria) Blood cultures (typhoid) LDH (hemolysis - malaria) Stool cultures Treat as P. Falciparum until proven otherwise!
WHAT TO DO? Consider it a medical emergency! CBC (anemia, thrombocytopenia in malaria and dengue) Thick and thin smears (malaria) Blood cultures (typhoid) LDH (hemolysis - malaria) Stool cultures Treat as P. Falciparum until proven otherwise!