

818f021ed0fadfda8f88ba9ff07f5ed7.ppt
- Количество слайдов: 20
 Trauma and Cardiac Resuscitation Dr. Paul Pageau Staff Physician Assistant Fellowship Director EMUS Department of Emergency Medicine University of Ottawa The Ottawa Hospital
Trauma and Cardiac Resuscitation Dr. Paul Pageau Staff Physician Assistant Fellowship Director EMUS Department of Emergency Medicine University of Ottawa The Ottawa Hospital
 Approach to patient with multisystem") Objectives n n General approach to Trauma/Resuscitation patients (A-B-C-D) Approach to patient with multisystem trauma (MVC, penetrating, and other) Approach to asystole/V-fib/STEMI patient and resuscitation, including drugs and therapeutic hypothermia Trauma code: Outline role of Emergency Physician, Emergency team, TTL, and other services
Objectives n n General approach to Trauma/Resuscitation patients (A-B-C-D) Approach to patient with multisystem trauma (MVC, penetrating, and other) Approach to asystole/V-fib/STEMI patient and resuscitation, including drugs and therapeutic hypothermia Trauma code: Outline role of Emergency Physician, Emergency team, TTL, and other services
 n Teamwork n") General Principles of Resuscitation Preparation n Triage (multiple and mass casualties) n Teamwork n Leadership n Communication n Crisis Resource management n Situation awareness n
General Principles of Resuscitation Preparation n Triage (multiple and mass casualties) n Teamwork n Leadership n Communication n Crisis Resource management n Situation awareness n
 Trauma A-B-C’s Primary Survey n A – Airway and C-spine n B – Breathing and Ventilation n C – Circulation and Hemorrhage control n D – Disability (Neuro) n E – Exposure and Environment control
Trauma A-B-C’s Primary Survey n A – Airway and C-spine n B – Breathing and Ventilation n C – Circulation and Hemorrhage control n D – Disability (Neuro) n E – Exposure and Environment control
 Adjuncts to Primary Survey Monitoring n Catheters n e. FAST n Consider transfer/ Trauma Code n
Adjuncts to Primary Survey Monitoring n Catheters n e. FAST n Consider transfer/ Trauma Code n
 n History and Physical examination n") Secondary Survey Head to Toe (finger or tube) n History and Physical examination n Continual reassessment of Vital signs n Complete Neuro exam n Specific radiologic evaluation (CT) n
Secondary Survey Head to Toe (finger or tube) n History and Physical examination n Continual reassessment of Vital signs n Complete Neuro exam n Specific radiologic evaluation (CT) n
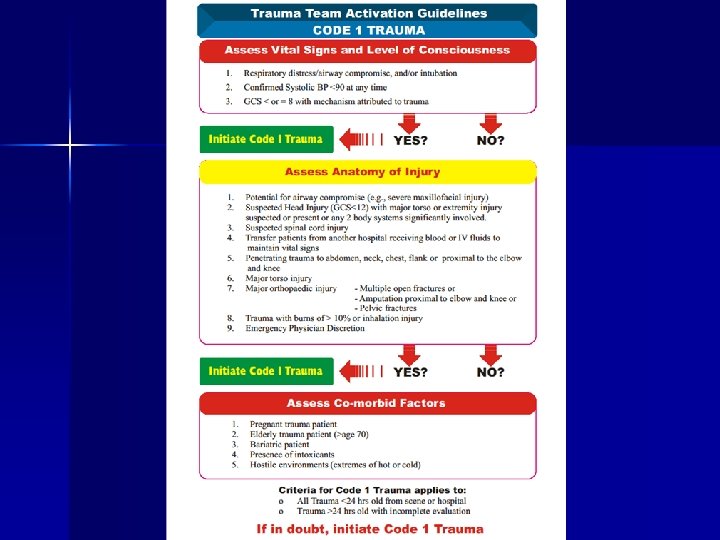
 n Trauma") Code One Trauma EP on duty +- Res/students, 3 RN’s (Chart, Action/Task) n Trauma Team Leader (Gen Surgery or Emerg staff) n Gen Surgery Sr Resident n Anaesthesia Resident n 2 Respiratory Therapists n 2 Patient Transport Workers n Advance care nurse practitioner – trauma n Clinical manager in ED n Trauma coordinator n Security n OR is notified n Trauma Dept is notified
Code One Trauma EP on duty +- Res/students, 3 RN’s (Chart, Action/Task) n Trauma Team Leader (Gen Surgery or Emerg staff) n Gen Surgery Sr Resident n Anaesthesia Resident n 2 Respiratory Therapists n 2 Patient Transport Workers n Advance care nurse practitioner – trauma n Clinical manager in ED n Trauma coordinator n Security n OR is notified n Trauma Dept is notified
 Code One Trauma n n n TTL is EP on duty until TTL on call arrives (<20 min) Gen Surg Resident may assume TTL role depending on Level of training Anaesthesia takes direction from TTL but mainly manages airway +- pain medication RN’s: IV catheters, monitoring, charting, other catheters, facilitating, anticipating RT’s: Airway assistance, Ventilation, monitoring
Code One Trauma n n n TTL is EP on duty until TTL on call arrives (<20 min) Gen Surg Resident may assume TTL role depending on Level of training Anaesthesia takes direction from TTL but mainly manages airway +- pain medication RN’s: IV catheters, monitoring, charting, other catheters, facilitating, anticipating RT’s: Airway assistance, Ventilation, monitoring
 Trauma Case 1 Hx: n 11 yo ATV no helmet, Collided with tree n Altered LOC, hematoma ant scalp, Ant chest contusion n EMS Vitals: HR 130, BP 80/60, Sats 90%RA, GCS=10, PERL n Long transport from Trail n IVF 1 L
Trauma Case 1 Hx: n 11 yo ATV no helmet, Collided with tree n Altered LOC, hematoma ant scalp, Ant chest contusion n EMS Vitals: HR 130, BP 80/60, Sats 90%RA, GCS=10, PERL n Long transport from Trail n IVF 1 L
 Trauma Case 1 n n n Boarded and collared wet clothes Vitals HR 120, BP 90/65, Sats 90% on O 2, RR 25, GCS=11, T 34. 8 tymp Vomitting Primary Survey: n Airway: moaning, emesis on face n Cspine protected n Decreased A/E on Right, dull percsn n Trachea midline n Decreased Cap refill n PERL n FAST pos pleural fluid, neg peritoneal fluid
Trauma Case 1 n n n Boarded and collared wet clothes Vitals HR 120, BP 90/65, Sats 90% on O 2, RR 25, GCS=11, T 34. 8 tymp Vomitting Primary Survey: n Airway: moaning, emesis on face n Cspine protected n Decreased A/E on Right, dull percsn n Trachea midline n Decreased Cap refill n PERL n FAST pos pleural fluid, neg peritoneal fluid
 Trauma Case 1 n n n pt vomits just prior to ETT roll onto side and suction pt develops pulseless VF when rolling defibrillate 2 J/kg X 1 vitals return to baseline
Trauma Case 1 n n n pt vomits just prior to ETT roll onto side and suction pt develops pulseless VF when rolling defibrillate 2 J/kg X 1 vitals return to baseline
 Trauma Case 1 Secondary Survey: n Right hemotympanum n Forehead abrasion and hematoma n Right chest contusion n Pelvis stable, Abdo soft Disposition: n Transfer to Tertiary care/ICU
Trauma Case 1 Secondary Survey: n Right hemotympanum n Forehead abrasion and hematoma n Right chest contusion n Pelvis stable, Abdo soft Disposition: n Transfer to Tertiary care/ICU
 Trauma Case 2 Large Community Hospital. OB/Anaesthesia in house, Peds often in house n EMS presents unannounced with 35 yr female MVC, VSA, 30 wks + pregnant. Hx: n 35 yo female. 30 wks+ pregnant, Belted passenger, T-boned, . n EMS on site <5 min: VSA, CPR and epinephrine X 2, intubated, 1 L NS n Arrival to ED after 25 mins downtime n
Trauma Case 2 Large Community Hospital. OB/Anaesthesia in house, Peds often in house n EMS presents unannounced with 35 yr female MVC, VSA, 30 wks + pregnant. Hx: n 35 yo female. 30 wks+ pregnant, Belted passenger, T-boned, . n EMS on site <5 min: VSA, CPR and epinephrine X 2, intubated, 1 L NS n Arrival to ED after 25 mins downtime n
 Trauma Case 2 Interventions? : n OB stat n Peds Primary Survey: n Intubated n Multiple right rib fractures – soft chest ? Air Entry on R n VSA – CPR in progress
Trauma Case 2 Interventions? : n OB stat n Peds Primary Survey: n Intubated n Multiple right rib fractures – soft chest ? Air Entry on R n VSA – CPR in progress
 Trauma Case 2 Interventions? : n perimortem C/S n ? Chest tube R Secondary Survey: n Pupils fixed dilated n blood from L ear and visible brain matter R skull n Pregnant abdomen n Pelvis unstable
Trauma Case 2 Interventions? : n perimortem C/S n ? Chest tube R Secondary Survey: n Pupils fixed dilated n blood from L ear and visible brain matter R skull n Pregnant abdomen n Pelvis unstable
 Cardiac Arrest and Resuscitation Principles: Chain of survival: n Recognition and activation n Early CPR n Rapid defibrillation n Advanced life support n Integrated post-cardiac arrest care
Cardiac Arrest and Resuscitation Principles: Chain of survival: n Recognition and activation n Early CPR n Rapid defibrillation n Advanced life support n Integrated post-cardiac arrest care
 Cardiac arrest n n n n Call for help, Defibrillator, CPR Shockable rhythm? 200 J CPR Asystole/PEA CPR Epi 1 mg q 3 -5 min, Atropine 1 mg q 3 -5 min X 3 Check for shockable rhythm q 2 min CPR Treat contributing factors (H’s and T’s) Consider antiarrhythmics: amiodarone 300 mg, or Lidocaine 1 mg/kg, Consider magnesium 1 – 2 gms for torsades
Cardiac arrest n n n n Call for help, Defibrillator, CPR Shockable rhythm? 200 J CPR Asystole/PEA CPR Epi 1 mg q 3 -5 min, Atropine 1 mg q 3 -5 min X 3 Check for shockable rhythm q 2 min CPR Treat contributing factors (H’s and T’s) Consider antiarrhythmics: amiodarone 300 mg, or Lidocaine 1 mg/kg, Consider magnesium 1 – 2 gms for torsades
 ROSC Evaluate for STEMI PCI/code STEMI n In comatose pts evaluate for therapeutic hypothermia n Stabilize, monitor, definitive care n
ROSC Evaluate for STEMI PCI/code STEMI n In comatose pts evaluate for therapeutic hypothermia n Stabilize, monitor, definitive care n
 Approach to patient with multisystem") Objectives n n General approach to Trauma/Resuscitation patients (A-B-C-D) Approach to patient with multisystem trauma (MVC, penetrating, and other) Approach to asystole/V-fib/STEMI patient and resuscitation, including drugs and therapeutic hypothermia Trauma code: Outline role of Emergency Physician, Emergency team, TTL, and other services
Objectives n n General approach to Trauma/Resuscitation patients (A-B-C-D) Approach to patient with multisystem trauma (MVC, penetrating, and other) Approach to asystole/V-fib/STEMI patient and resuscitation, including drugs and therapeutic hypothermia Trauma code: Outline role of Emergency Physician, Emergency team, TTL, and other services