ca9fea882653912ca9ffd4d106fbf6e7.ppt
- Количество слайдов: 76
 Topics Survey Results FY ’ 07 Overall Process Verification and Eligibility Specialized Child Care COPA 3455 IPACS IMEDGE/Scanning Policy and. Appeals Q & A
Topics Survey Results FY ’ 07 Overall Process Verification and Eligibility Specialized Child Care COPA 3455 IPACS IMEDGE/Scanning Policy and. Appeals Q & A
 COPA Ø Can you produce a 3455? 60% Yes Ø 40% No Does the Activity Number show? 58% Yes 42% No
COPA Ø Can you produce a 3455? 60% Yes Ø 40% No Does the Activity Number show? 58% Yes 42% No
 Top Topics for Discussion COPA Eligibility and Verification IMEDGE IPACS
Top Topics for Discussion COPA Eligibility and Verification IMEDGE IPACS
 Eligibility / Verification Ø What areas of eligibility are major concerns? • • Ø What areas of income verification need explanation? • • Ø Employment/Income Verification Income Guidelines Documentation Cash payees What areas of DCFS documentation need more clarification? • Homeless • Incapacitated Adult / Child
Eligibility / Verification Ø What areas of eligibility are major concerns? • • Ø What areas of income verification need explanation? • • Ø Employment/Income Verification Income Guidelines Documentation Cash payees What areas of DCFS documentation need more clarification? • Homeless • Incapacitated Adult / Child
 IMEDGE/SCANNING Ø Has your site been trained on the scanning process? • 10% – Yes • 90% – No Ø Some main topics regarding the scanning process? • Training • Equipment • Cost • Procedure • Technical Assistance
IMEDGE/SCANNING Ø Has your site been trained on the scanning process? • 10% – Yes • 90% – No Ø Some main topics regarding the scanning process? • Training • Equipment • Cost • Procedure • Technical Assistance
 IPACS Ø Are you familiar with the Illinois Department of Human Services IPACS system? • 25% Yes • 75% No Ø Some main topics regarding IPACS? • Impact on eligibility process • Delay in approval process • Procedural changes • Inconsistent data
IPACS Ø Are you familiar with the Illinois Department of Human Services IPACS system? • 25% Yes • 75% No Ø Some main topics regarding IPACS? • Impact on eligibility process • Delay in approval process • Procedural changes • Inconsistent data
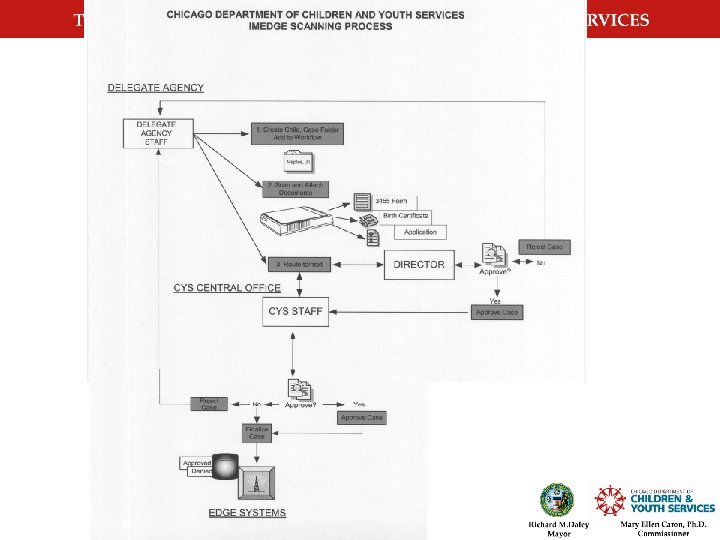
 COPA CYS 3455 IMEDGE CYS 3455 & Documentation Scanning system No IMEDGE Required Documentation? Scanning system Yes IPACS system No Yes Valid Information? CCMIS Billings
COPA CYS 3455 IMEDGE CYS 3455 & Documentation Scanning system No IMEDGE Required Documentation? Scanning system Yes IPACS system No Yes Valid Information? CCMIS Billings
 Who’s affected by the changes? 1. CYS Delegates and Partners who have program models that are funded wholly or in part by IDHS 2. CYS Delegates and Partners who receive reimbursement from CYS for IDHS funded programs (CCMIS)
Who’s affected by the changes? 1. CYS Delegates and Partners who have program models that are funded wholly or in part by IDHS 2. CYS Delegates and Partners who receive reimbursement from CYS for IDHS funded programs (CCMIS)
 COPA CYS 3455
COPA CYS 3455
 CYS 3455 Changes Page 1 Required for COPA • Ethnicity • Educational Level • Employment Status • Revision Date
CYS 3455 Changes Page 1 Required for COPA • Ethnicity • Educational Level • Employment Status • Revision Date
 USE THE MOST CURRENT 3455 ALWAYS
USE THE MOST CURRENT 3455 ALWAYS
 CYS 3455 Changes Page 1 Required for COPA • Receiving WIC? • Revision Date
CYS 3455 Changes Page 1 Required for COPA • Receiving WIC? • Revision Date
 CYS 3455 Changes Page 2 No major changes • Revision Date bottom left
CYS 3455 Changes Page 2 No major changes • Revision Date bottom left
 CYS 3455 Changes Page 2 b Members page • Effective June 1, 2006 • All members counted in the family size excluding children
CYS 3455 Changes Page 2 b Members page • Effective June 1, 2006 • All members counted in the family size excluding children
 CYS 3455 Changes Page 3 Applicant Certification • Items 8, 9, 10
CYS 3455 Changes Page 3 Applicant Certification • Items 8, 9, 10
 Item # 8 • I understand the information provided will be checked using State databases, and if inconsistencies are discovered, the processing of my application may be delayed or denied.
Item # 8 • I understand the information provided will be checked using State databases, and if inconsistencies are discovered, the processing of my application may be delayed or denied.
 Item # 9 • I understand that I am not required to provide my Social Security Number and that if I deliberately provide an incorrect or fictitious Social Security Number I may be prosecuted for fraud.
Item # 9 • I understand that I am not required to provide my Social Security Number and that if I deliberately provide an incorrect or fictitious Social Security Number I may be prosecuted for fraud.
 Item # 10 • My signature is my consent and authorization for information to be released to the Chicago Department of Children and Youth Services, the Illinois Department of Human Services or its agents that may establish my eligibility or my continued eligibility for the Child Care Program.
Item # 10 • My signature is my consent and authorization for information to be released to the Chicago Department of Children and Youth Services, the Illinois Department of Human Services or its agents that may establish my eligibility or my continued eligibility for the Child Care Program.
 CYS 3455 Changes Page 4 Provider Certification • Item #10 • Revised Date
CYS 3455 Changes Page 4 Provider Certification • Item #10 • Revised Date
 How to complete a COPA 3455 • Document in folder • School Age 7 - 12 • Activity Number
How to complete a COPA 3455 • Document in folder • School Age 7 - 12 • Activity Number
 School Age 7 - 12
School Age 7 - 12
 COPA - Activity# Missing? • Activity #’s are agency, site and program model specific. • Contact La Tasha White-Grey @ cy 00515@cityofchicago. org
COPA - Activity# Missing? • Activity #’s are agency, site and program model specific. • Contact La Tasha White-Grey @ cy 00515@cityofchicago. org
 I N T R O D U C I N G
I N T R O D U C I N G
 IMEDGE The
IMEDGE The
 The Site Readiness Checklist must be FULLY completed. The vendor cannot install with missing information.
The Site Readiness Checklist must be FULLY completed. The vendor cannot install with missing information.
 Summary: The End
Summary: The End
 PILOT AGENCY MEETING • Meeting for last summers pilot agencies on 6/28/06 @ CYS Central office. • Meeting start time 1: 00 P. M.
PILOT AGENCY MEETING • Meeting for last summers pilot agencies on 6/28/06 @ CYS Central office. • Meeting start time 1: 00 P. M.
 Verification and Eligibility
Verification and Eligibility
 Verification CYS will. . . • retrieve all child care documentation via IMEDGE • check for completeness and accuracy • verify all IDHS cases using the IPACS system • determine eligibility using the CCMIS system • update the IMEDGE system with rejection, denial and approval information • publish child care billings every month for all delegates
Verification CYS will. . . • retrieve all child care documentation via IMEDGE • check for completeness and accuracy • verify all IDHS cases using the IPACS system • determine eligibility using the CCMIS system • update the IMEDGE system with rejection, denial and approval information • publish child care billings every month for all delegates
 Verification Child Care providers must… • post and distribute all Child Care Program requirements to new and existing clients • ensure that clients have been informed of and read items #8, 9, 10 on page 3 under Applicant Certification • gather all information from clients that will determine child care eligibility • notify clients of their right to appeal
Verification Child Care providers must… • post and distribute all Child Care Program requirements to new and existing clients • ensure that clients have been informed of and read items #8, 9, 10 on page 3 under Applicant Certification • gather all information from clients that will determine child care eligibility • notify clients of their right to appeal
 Eligibility State databases may not reflect termination of benefits and delay the eligibility process if all required information is not submitted The following documentation will be used to determine eligibility: » » » CYS 3455 Social Security number or other documentation Current pay stubs or other income verification HSEV (collaboration cases) Other (RASP, employer verification letters, training schedule, termination of benefits, etc…
Eligibility State databases may not reflect termination of benefits and delay the eligibility process if all required information is not submitted The following documentation will be used to determine eligibility: » » » CYS 3455 Social Security number or other documentation Current pay stubs or other income verification HSEV (collaboration cases) Other (RASP, employer verification letters, training schedule, termination of benefits, etc…
 Best Practices Acquire the most accurate information from clients Revise in-take questions for the client interview: v ask for all information of members of household that are part of the “Family Composition” (defined under 01. 02 of the IDHS Child Care Manual) v ask if the client has received any “Non-exempt Income” (defined under 01. 02 of the IDHS Child Care Manual) v ask if the client and/or family members have had more than one employer during the last two quarters if the year
Best Practices Acquire the most accurate information from clients Revise in-take questions for the client interview: v ask for all information of members of household that are part of the “Family Composition” (defined under 01. 02 of the IDHS Child Care Manual) v ask if the client has received any “Non-exempt Income” (defined under 01. 02 of the IDHS Child Care Manual) v ask if the client and/or family members have had more than one employer during the last two quarters if the year
 Best Practices Request letters and documentation from all sources indicating termination of payments and benefits Ensure Social Security Numbers are valid Accept documentation (defined under 01. 01 IDHS Child Care Manual) when Social Security Numbers are not provided: v Birth certificate (U. S. and other countries) v Baptismal certificate v Medical record, etc…
Best Practices Request letters and documentation from all sources indicating termination of payments and benefits Ensure Social Security Numbers are valid Accept documentation (defined under 01. 01 IDHS Child Care Manual) when Social Security Numbers are not provided: v Birth certificate (U. S. and other countries) v Baptismal certificate v Medical record, etc…
 Time Lines • CYS Child Care eligibility timelines have not changed. • Agency “route to” date to CYS will become the stamp date. • CYS processing time is approx. 10 -15 days
Time Lines • CYS Child Care eligibility timelines have not changed. • Agency “route to” date to CYS will become the stamp date. • CYS processing time is approx. 10 -15 days
 Specialized Child Care
Specialized Child Care
 Specialized Child Care While the fundamental objective for all CYS child care programs is to provide services to children daily in a safe, nurturing environment that fosters their healthy social, emotional, physical and intellectual development, it is through the CYS Specialized Child Care component that special cases/special needs of enrolled children and families are addressed. The following are the most often used categories for Special Cases with no Co-Payment: Ø Incapacitated Adult Ø Special Needs ( Child with disability) Ø Non-DCFS Social Service Referral Ø DCFS Foster Child Ø Child of Teen Ward
Specialized Child Care While the fundamental objective for all CYS child care programs is to provide services to children daily in a safe, nurturing environment that fosters their healthy social, emotional, physical and intellectual development, it is through the CYS Specialized Child Care component that special cases/special needs of enrolled children and families are addressed. The following are the most often used categories for Special Cases with no Co-Payment: Ø Incapacitated Adult Ø Special Needs ( Child with disability) Ø Non-DCFS Social Service Referral Ø DCFS Foster Child Ø Child of Teen Ward
 Ø On letterhead stationery (preferably typed)") Incapacitated Adult: Single /Two -Parent Family Documentation: (Adult) Ø On letterhead stationery (preferably typed) by the Physician, Psychiatrist or other licensed practitioner. Ø The name & date of birth of the caretaker(s) parent(s) or guardian(s) who is (are) disabled. Ø The nature of disability, including the physical limitations and onset date of disabling condition. Ø The length of time the disability is expected to last, including whether the condition(s) is temporary or permanent. Ø Recommendation that child care be provided during the period of disability Eligibility • Collaboration – 1 year • Child Care – 6 months
Incapacitated Adult: Single /Two -Parent Family Documentation: (Adult) Ø On letterhead stationery (preferably typed) by the Physician, Psychiatrist or other licensed practitioner. Ø The name & date of birth of the caretaker(s) parent(s) or guardian(s) who is (are) disabled. Ø The nature of disability, including the physical limitations and onset date of disabling condition. Ø The length of time the disability is expected to last, including whether the condition(s) is temporary or permanent. Ø Recommendation that child care be provided during the period of disability Eligibility • Collaboration – 1 year • Child Care – 6 months
 A child must be under 13 years old, unless the") Incapacitated Child (Special Needs/Incapacitated) A child must be under 13 years old, unless the child is a foster child, to be considered for eligibility in this category. Documentation: (Child) Ø Documentation is submitted on letterhead stationery (preferably typed) by the Physician, Psychiatrist or other licensed practitioner Ø Name and birth date of the child with the disability Ø Nature of the disability including the diagnosis, degree of developmental delay(s) in specified areas of development and onset of disability Ø The length of time the disability is expected to last, including whether the condition(s) is temporary or permanent. Ø How services will meet the special developmental need of the child. Ø Recommendation that child care is needed. Eligibility • Collaboration – 1 year • Child Care – 6 months
Incapacitated Child (Special Needs/Incapacitated) A child must be under 13 years old, unless the child is a foster child, to be considered for eligibility in this category. Documentation: (Child) Ø Documentation is submitted on letterhead stationery (preferably typed) by the Physician, Psychiatrist or other licensed practitioner Ø Name and birth date of the child with the disability Ø Nature of the disability including the diagnosis, degree of developmental delay(s) in specified areas of development and onset of disability Ø The length of time the disability is expected to last, including whether the condition(s) is temporary or permanent. Ø How services will meet the special developmental need of the child. Ø Recommendation that child care is needed. Eligibility • Collaboration – 1 year • Child Care – 6 months
 Non –DCFS Social Service Agency Referral Cases Clients/families referred through a certified, licensed, or registered professional due to an experience of or discerned potential for child abuse, neglect, exploitation, or similarly harmful circumstances. Families residing in homeless shelters that operate Children in Shelters Program (Salvation Army) or Recovery homes. Documentation: Ø Must include an evaluation of the current child/family situation and need for the children to receive child care service. Ø The printed/typed name, location, telephone number and signature of the professional making the referral must be on the letter/evaluation Ø A description of the family situation , including all names, birth dates legal guardianship for each child needing child care, current living arrangement/whereabouts of all pertinent family members and all problems and planned resolution(s), short term and long term must be provided. Ø A recommendation that child care is necessary to correct specified problem(s). Ø An indication that continued casework services (including and explanation of who (name and agency name), what specific services and anticipated time frame of services that will be provided to the family that is typed or legible. Eligibility • Collaboration – 1 year • Child Care – 6 months
Non –DCFS Social Service Agency Referral Cases Clients/families referred through a certified, licensed, or registered professional due to an experience of or discerned potential for child abuse, neglect, exploitation, or similarly harmful circumstances. Families residing in homeless shelters that operate Children in Shelters Program (Salvation Army) or Recovery homes. Documentation: Ø Must include an evaluation of the current child/family situation and need for the children to receive child care service. Ø The printed/typed name, location, telephone number and signature of the professional making the referral must be on the letter/evaluation Ø A description of the family situation , including all names, birth dates legal guardianship for each child needing child care, current living arrangement/whereabouts of all pertinent family members and all problems and planned resolution(s), short term and long term must be provided. Ø A recommendation that child care is necessary to correct specified problem(s). Ø An indication that continued casework services (including and explanation of who (name and agency name), what specific services and anticipated time frame of services that will be provided to the family that is typed or legible. Eligibility • Collaboration – 1 year • Child Care – 6 months
 Foster Care The case worker, from DCFS or a private agency that is contracted with DCFS, must specify in a letter the special developmental (physical) need for child care services. Documentation: Ø A letter that must state how child care will meet the special need of the individual child or a DCFS Foster Child Referral Form. Ø Copy of the Medical Card – Case ID# begins with (98…), (J…. ) Eligibility • Collaboration – 6 months • Child Care – 6 months
Foster Care The case worker, from DCFS or a private agency that is contracted with DCFS, must specify in a letter the special developmental (physical) need for child care services. Documentation: Ø A letter that must state how child care will meet the special need of the individual child or a DCFS Foster Child Referral Form. Ø Copy of the Medical Card – Case ID# begins with (98…), (J…. ) Eligibility • Collaboration – 6 months • Child Care – 6 months
 Child of DCFS Teen Ward The child of a teen DCFS ward (in foster care) is not the foster child however the teen parent is a ward (in foster care) until the teen becomes 21 years old or is emancipated through the Cook County Juvenile Court(Judge) which can be before the teen’s 21 st birthday. Documentation: Ø An original letter from DCFS or the contracting agency, stating that the teen parent is in school, employed or in a employment training program and child care is needed. Ø The letter must also list the teen parents DCFS case ID number, Social Security number, a copy of the birth certificate for each child and the case workers’ name, agency name and phone number Ø In addition to documentation from the school/training program/employer. Eligibility • Collaboration – 1 year • Child Care – 6 months
Child of DCFS Teen Ward The child of a teen DCFS ward (in foster care) is not the foster child however the teen parent is a ward (in foster care) until the teen becomes 21 years old or is emancipated through the Cook County Juvenile Court(Judge) which can be before the teen’s 21 st birthday. Documentation: Ø An original letter from DCFS or the contracting agency, stating that the teen parent is in school, employed or in a employment training program and child care is needed. Ø The letter must also list the teen parents DCFS case ID number, Social Security number, a copy of the birth certificate for each child and the case workers’ name, agency name and phone number Ø In addition to documentation from the school/training program/employer. Eligibility • Collaboration – 1 year • Child Care – 6 months
 CYS/DCFS SPECIAL CASE Note: Scenario #1 If a new family is submitting a application with the required documentation for the first time and is not employed, there is no Co-Payment. or Scenario #2 If a Child Care Employment Related family circumstances change within the redetermination period, a application with the required documentations may be submitted and no Co-Payment. Both cases will be categorized as a DCFS Special Case.
CYS/DCFS SPECIAL CASE Note: Scenario #1 If a new family is submitting a application with the required documentation for the first time and is not employed, there is no Co-Payment. or Scenario #2 If a Child Care Employment Related family circumstances change within the redetermination period, a application with the required documentations may be submitted and no Co-Payment. Both cases will be categorized as a DCFS Special Case.
 The IPACS presentation is for informational purposes only.
The IPACS presentation is for informational purposes only.
 IPACS IDHS Bureau of Child Care and Development June 2006
IPACS IDHS Bureau of Child Care and Development June 2006
 IPACS Illinois Public Aid Communication System
IPACS Illinois Public Aid Communication System
 IDHS Promotes Access to Child Care Through Partnerships Multiple Delivery Systems § Chicago Department of Children and Youth Services (CYS Delegate Agencies) § Child Care Resource and Referral Agencies (CCR&Rs) and INCCRRA § Site Administered Child Care Providers § Head Start Program Collaboration
IDHS Promotes Access to Child Care Through Partnerships Multiple Delivery Systems § Chicago Department of Children and Youth Services (CYS Delegate Agencies) § Child Care Resource and Referral Agencies (CCR&Rs) and INCCRRA § Site Administered Child Care Providers § Head Start Program Collaboration
 Objectives The Non-Child Care Eligibility system has been developed to establish a consistent statewide process for CCR&R Agencies, Site Administered Child Care providers, CYS and IDHS Bureau of Child Care and Development for use when processing Child Care Applications and Redeterminations. The goal is to better utilize funding by ensuring applicants meet all eligibility guidelines, using all available information. This includes screens on the Non-Child Care Eligibility system.
Objectives The Non-Child Care Eligibility system has been developed to establish a consistent statewide process for CCR&R Agencies, Site Administered Child Care providers, CYS and IDHS Bureau of Child Care and Development for use when processing Child Care Applications and Redeterminations. The goal is to better utilize funding by ensuring applicants meet all eligibility guidelines, using all available information. This includes screens on the Non-Child Care Eligibility system.
 Information Sources The information comes from sources outside the jurisdiction of the Bureau of Child Care and Development. Therefore, • The information is not specifically formatted to determine Child Care eligibility. • Information is to be used collaboratively with other relevant facts in determining eligibility EMPLOYER CLIENT PACIS IDHS
Information Sources The information comes from sources outside the jurisdiction of the Bureau of Child Care and Development. Therefore, • The information is not specifically formatted to determine Child Care eligibility. • Information is to be used collaboratively with other relevant facts in determining eligibility EMPLOYER CLIENT PACIS IDHS
 – RPY status – Grant") Data Bases Used • ACID (Automated Client Information Database) – RPY status – Grant amount – Assistance unit information (DOB, SSN, relationships, type benefits, living in home) – Earned and unearned income codes – RSP activity
Data Bases Used • ACID (Automated Client Information Database) – RPY status – Grant amount – Assistance unit information (DOB, SSN, relationships, type benefits, living in home) – Earned and unearned income codes – RSP activity
 – Unemployment Compensation – Multiple") Data Bases Used • AWVS (Automated Wage Verification System) – Unemployment Compensation – Multiple employers – Average monthly income amounts (for comparison to check stubs) • KIDS (Key Information Delivery System) – Child Support payments – SSNs – Relationships • Chicago Student On-Line – Determine if child not on parents PACIS case has other address and/or guardian listed
Data Bases Used • AWVS (Automated Wage Verification System) – Unemployment Compensation – Multiple employers – Average monthly income amounts (for comparison to check stubs) • KIDS (Key Information Delivery System) – Child Support payments – SSNs – Relationships • Chicago Student On-Line – Determine if child not on parents PACIS case has other address and/or guardian listed
 PACIS Basic Principles For confirmation, not determination. Use as a guide, not to decide. When you cannot verify, you must clarify. Screen print, baby, screen print.
PACIS Basic Principles For confirmation, not determination. Use as a guide, not to decide. When you cannot verify, you must clarify. Screen print, baby, screen print.
 First Step – Child Care Tracking System • CYS will check to see if the family has an active child care case or a recently denied application through IDHS or AFC • IDHS and AFC will check COPA for active or a recently denied CYS cases as well
First Step – Child Care Tracking System • CYS will check to see if the family has an active child care case or a recently denied application through IDHS or AFC • IDHS and AFC will check COPA for active or a recently denied CYS cases as well
 CCTS Name Search Screen
CCTS Name Search Screen
 Non-Child Care Eligibility Inquiry Menu
Non-Child Care Eligibility Inquiry Menu
 ACID SCREEN 1 DATE : 04 15 02 TIME : 14 05 29 LAST NAME, FIRST NAME RPY CASE ID: 04 - 215 - 06 - A 12345 STREET ADDRESS AND APT. # CSLD: 403 TA: 31 DEF: 1 TAR: 61 CITY OR TOWN, STATE ZIPCODE-XXXX TERM ID: C 501 EFF DATE: 03/02 NO 552: 05 SCH: 06 LAST MED DET DT: 01/02 LAST OPEN: 12/01 REDER DATE: 01/02 SSA #: 123 -45 -6789 END MED DT: CERT DATE: EBT ACCT: 000000123 INST DATE: DIR DEL CD: OGRTRSN: TRANOPA: 4 ID EXP DATE: 05/19/02 MEC REST: CASE STAT: ACTIVE REGULAR CASE BANK: ACCNT: FROM 94 215 00 B 12345 BNK SSN: PHONE: 312 793 -3610 FOOD STAMP STAT: ACTIVE OPA: 00 PROP: 0 LANGCDE: 00 FDST APP STAT: APPRV 1 MONTH NATORG: 00 SPONSOR: 00 NOLVTOG: 08 SPEND-DOWN STAT: RACE: 2 UTRENT: 01 #FSEATOG: 05 REDETERMINATIONS MAJCR: 00 PUBLICH: 0 BX 26: SUPERV: 112233333 LIST CD: FOODST: 1 LIVARR: 00 CASEWKR: 113344444 DISP CD: 1 REP CODE: DATE APR: 02/07/02 CRITERIA: P-W 03/99 REPORT PROCESSED AMT GR CHG: . 00 BX 25: DCFS/DHS: ->2001 ->2002 PHONE 2: - M J J A S O N D J F M A M GRANT HISTORY Y Y Y MEDICAL HISTORY Y Y Y Y Y Y FOOD STAMP HISTORY Y Y Y Y Y 2=NEEDS 3=PEOPL 4=HIST 5=2943 6=MED/PCIS PF/F 10: ARS
ACID SCREEN 1 DATE : 04 15 02 TIME : 14 05 29 LAST NAME, FIRST NAME RPY CASE ID: 04 - 215 - 06 - A 12345 STREET ADDRESS AND APT. # CSLD: 403 TA: 31 DEF: 1 TAR: 61 CITY OR TOWN, STATE ZIPCODE-XXXX TERM ID: C 501 EFF DATE: 03/02 NO 552: 05 SCH: 06 LAST MED DET DT: 01/02 LAST OPEN: 12/01 REDER DATE: 01/02 SSA #: 123 -45 -6789 END MED DT: CERT DATE: EBT ACCT: 000000123 INST DATE: DIR DEL CD: OGRTRSN: TRANOPA: 4 ID EXP DATE: 05/19/02 MEC REST: CASE STAT: ACTIVE REGULAR CASE BANK: ACCNT: FROM 94 215 00 B 12345 BNK SSN: PHONE: 312 793 -3610 FOOD STAMP STAT: ACTIVE OPA: 00 PROP: 0 LANGCDE: 00 FDST APP STAT: APPRV 1 MONTH NATORG: 00 SPONSOR: 00 NOLVTOG: 08 SPEND-DOWN STAT: RACE: 2 UTRENT: 01 #FSEATOG: 05 REDETERMINATIONS MAJCR: 00 PUBLICH: 0 BX 26: SUPERV: 112233333 LIST CD: FOODST: 1 LIVARR: 00 CASEWKR: 113344444 DISP CD: 1 REP CODE: DATE APR: 02/07/02 CRITERIA: P-W 03/99 REPORT PROCESSED AMT GR CHG: . 00 BX 25: DCFS/DHS: ->2001 ->2002 PHONE 2: - M J J A S O N D J F M A M GRANT HISTORY Y Y Y MEDICAL HISTORY Y Y Y Y Y Y FOOD STAMP HISTORY Y Y Y Y Y 2=NEEDS 3=PEOPL 4=HIST 5=2943 6=MED/PCIS PF/F 10: ARS
 ACID SCREEN 2 CASE ID: 04 - 236 - 06 - EI 0000 NEEDS CODE AMT/RIN PERS TCOST SBY 643 10/01 675 10/01 1 676 07/97 INCOME/DEDUCTIONS RESERVES FOOD STAMPS: CODE AMNT SCR NUM RNO CODE AMOUNT CASEINHH: 1 EARNED: 645. 00 599 215. 00 999999000 701 35. 00 NOINHH: 03 UNERND: 162. 00 802 0645 H 35 Y 999999000 NOEATTG: 03 DCC: . 00 UTILIND: 1 HSECST: 100. 00 CERTEX: 11/02 UTLCST: 255. 00 EPA: . 00 MEDEXP: . 00 NCA: . 00 CS: . 00 BUS EXP RNO DCD AMT NUM EIE DT-CNT FIL: . 00 TOTINC: 461. 00 401 . 00 999999000 . 00 0 00/00 00 CATELGIND: 8 BONUS: 217. 00 NEWSHLTRMX: PRO/RET: P MTCH MTPRS TPERS PERALLW TNEEDS TOTDED GRANT SURINC RESERVE 02 03 377. 00 215. 00 162. 00 35. 00 1=BASIC 3=PEOPL 4=HIST 5=2943 6=MED/PCIS PF/F 10: ARS
ACID SCREEN 2 CASE ID: 04 - 236 - 06 - EI 0000 NEEDS CODE AMT/RIN PERS TCOST SBY 643 10/01 675 10/01 1 676 07/97 INCOME/DEDUCTIONS RESERVES FOOD STAMPS: CODE AMNT SCR NUM RNO CODE AMOUNT CASEINHH: 1 EARNED: 645. 00 599 215. 00 999999000 701 35. 00 NOINHH: 03 UNERND: 162. 00 802 0645 H 35 Y 999999000 NOEATTG: 03 DCC: . 00 UTILIND: 1 HSECST: 100. 00 CERTEX: 11/02 UTLCST: 255. 00 EPA: . 00 MEDEXP: . 00 NCA: . 00 CS: . 00 BUS EXP RNO DCD AMT NUM EIE DT-CNT FIL: . 00 TOTINC: 461. 00 401 . 00 999999000 . 00 0 00/00 00 CATELGIND: 8 BONUS: 217. 00 NEWSHLTRMX: PRO/RET: P MTCH MTPRS TPERS PERALLW TNEEDS TOTDED GRANT SURINC RESERVE 02 03 377. 00 215. 00 162. 00 35. 00 1=BASIC 3=PEOPL 4=HIST 5=2943 6=MED/PCIS PF/F 10: ARS
 ACID SCREEN 3 PAGE 1 OF 1 ASSISTANCE UNIT CASE ID: 04 - 215 - 06 - A 12345 01 00009999 FIRST NAME LAST NAME BX 78: REL: 02 STAT MO/FA: --/- 09/25/1974 -F 123 -00 -0000 V 04/15/92 ACT: - VET: 1 ED: F MAR: 1 WRK: 8 PC/H: 9 MT: 1 CT: 30 TPL: 000 AL#: CL#: BX 64: -- EDD: I/FI: CNT: 18 02 00000001 CHILD NO. 1 BX 78: REL: 05 STAT MO/FA: 13/24 05/13/1992 -F 1234 -01 -0000 V 02/04/93 ACT: - VET: 1 ED: - MAR: - WRK: PC/H: - MT: 3 CT: 30 TPL: 000 AL#: CL#: BX 64: -- EDD: I/FI: CNT: 03 09700002 CHILD NO. 2 BX 78: REL: 05 STAT MO/FA: 13/24 07/28/1994 -F 123 -02 -0000 V 02/28/95 ACT: - VET: 1 ED: - MAR: - WRK: PC/H: - MT: 3 CT: 30 TPL: 000 AL#: CL#: BX 64: -- EDD: I/FI: CNT: 04 10700003 CHILD NO. 3 BX 78: REL: 05 STAT MO/FA: 13/24 09/26/1998 -M 123 -03 -0000 V 01/08/99 ACT: - VET: 1 ED: - MAR: - WRK: PC/H: - MT: 3 CT: 30 TPL: 000 AL#: CL#: BX 64: -- EDD: I/FI: CNT: 05 117000004 CHILD NO. 4 BX 78: REL: 05 STAT MO/FA: 13/24 12/15/1999 -M 123 -04 -0000 V 01/18/01 ACT: - VET: 1 ED: - MAR: - WRK: PC/H: - MT: 3 CT: 30 TPL: 000 AL#: CL#: BX 64: -- EDD: I/FI: CNT: 1=BASIC 2=NEEDS 4=HIST 5=2943 6=MED/PCIS PF/F 8: MMIS PF/F 10: ARS
ACID SCREEN 3 PAGE 1 OF 1 ASSISTANCE UNIT CASE ID: 04 - 215 - 06 - A 12345 01 00009999 FIRST NAME LAST NAME BX 78: REL: 02 STAT MO/FA: --/- 09/25/1974 -F 123 -00 -0000 V 04/15/92 ACT: - VET: 1 ED: F MAR: 1 WRK: 8 PC/H: 9 MT: 1 CT: 30 TPL: 000 AL#: CL#: BX 64: -- EDD: I/FI: CNT: 18 02 00000001 CHILD NO. 1 BX 78: REL: 05 STAT MO/FA: 13/24 05/13/1992 -F 1234 -01 -0000 V 02/04/93 ACT: - VET: 1 ED: - MAR: - WRK: PC/H: - MT: 3 CT: 30 TPL: 000 AL#: CL#: BX 64: -- EDD: I/FI: CNT: 03 09700002 CHILD NO. 2 BX 78: REL: 05 STAT MO/FA: 13/24 07/28/1994 -F 123 -02 -0000 V 02/28/95 ACT: - VET: 1 ED: - MAR: - WRK: PC/H: - MT: 3 CT: 30 TPL: 000 AL#: CL#: BX 64: -- EDD: I/FI: CNT: 04 10700003 CHILD NO. 3 BX 78: REL: 05 STAT MO/FA: 13/24 09/26/1998 -M 123 -03 -0000 V 01/08/99 ACT: - VET: 1 ED: - MAR: - WRK: PC/H: - MT: 3 CT: 30 TPL: 000 AL#: CL#: BX 64: -- EDD: I/FI: CNT: 05 117000004 CHILD NO. 4 BX 78: REL: 05 STAT MO/FA: 13/24 12/15/1999 -M 123 -04 -0000 V 01/18/01 ACT: - VET: 1 ED: - MAR: - WRK: PC/H: - MT: 3 CT: 30 TPL: 000 AL#: CL#: BX 64: -- EDD: I/FI: CNT: 1=BASIC 2=NEEDS 4=HIST 5=2943 6=MED/PCIS PF/F 8: MMIS PF/F 10: ARS
 ACID SCREEN 6 PAGE 1 ASSISTANCE UNIT MEDICAL/W & T ACTIVITIES CASE ID: 04 - 215 - 06 - 000 A 12345 01 000009999 FIRST NAME 09/25/1974 EDD: CARVE: CHOICE: 5 LSSI: HIB: SMIB: QMB: RENAL: CM: ENROLL: BEGIN: END: PRV: ENROLL: BEGIN: END: RRP: TYP: BX 27: B: E: ACT DT: 01/14/02 CDE: 0350 HR: 30 CNTL: 07/01/02 MGR: 215 TRANS: 075 05/06/99 3999 00 06/11/99 C 83 000
ACID SCREEN 6 PAGE 1 ASSISTANCE UNIT MEDICAL/W & T ACTIVITIES CASE ID: 04 - 215 - 06 - 000 A 12345 01 000009999 FIRST NAME 09/25/1974 EDD: CARVE: CHOICE: 5 LSSI: HIB: SMIB: QMB: RENAL: CM: ENROLL: BEGIN: END: PRV: ENROLL: BEGIN: END: RRP: TYP: BX 27: B: E: ACT DT: 01/14/02 CDE: 0350 HR: 30 CNTL: 07/01/02 MGR: 215 TRANS: 075 05/06/99 3999 00 06/11/99 C 83 000
 MORE INFORMATION ON NEXT PAGE -- DEPRESS PA 1") Automated Wage Verification System (AWVC) MORE INFORMATION ON NEXT PAGE -- DEPRESS PA 1 PAGE 1 04/17/2002 AWVS INQUIRY SYSTEM OF 2 SSNO: XXX XX XXXX YEAR: QTR: CLAIMANT: LAST NAME, FIRST NAME BIRTH: 12/15/1970 STREET ADDRESS SPOUSE: CITY OR TOWN STATE ZIPCODE COUNTY: 200 COOK ALIAS SSNO: CLAIM DATE: 12/31/2000 LATEST CHK: 07/18/2001 WKLY BASIC BEN: 111. 00 BENEFIT PERIOD: 12/31/2000 THRU 12/30/2001 DEP ALLOWANCE: 36. 00 MAX BEN AMT: 2, 886. 00 MAX BEN BAL: WK BEN AMT: 147. 00 EMPLOYER ID/NAME/PLANT/ADDR/CITY/ST/ZIP ----- WAGES BY QUARTER ----- 1/2001 2/2001 3/2001 4/2001 1705724 EMPLOYER NO. 1 000 STREET ADDRESS CITY OR TOWN STATE ZIPCODE 252 92 4205110 EMPLOYER NO. 2 STREET ADDRESS CITY OR TOWN STATE ZIPCODE 1248 PAY DATE AMOUNT WKS PD PAY END-DT | PAY DATE AMOUNT WKS PD PAY END-DT 07/18/2001 147. 00 01 07/07/2001 | 07/05/2001 294. 00 02 06/30/2001 06/20/2001 294. 00 02 06/16/2001 | 06/06/2001 294. 00 02 06/02/2001 05/23/2001 294. 00 02 05/19/2001 | 05/09/2001 294. 00 02 05/05/2001 04/25/2001 294. 00 03 04/21/2001 |
Automated Wage Verification System (AWVC) MORE INFORMATION ON NEXT PAGE -- DEPRESS PA 1 PAGE 1 04/17/2002 AWVS INQUIRY SYSTEM OF 2 SSNO: XXX XX XXXX YEAR: QTR: CLAIMANT: LAST NAME, FIRST NAME BIRTH: 12/15/1970 STREET ADDRESS SPOUSE: CITY OR TOWN STATE ZIPCODE COUNTY: 200 COOK ALIAS SSNO: CLAIM DATE: 12/31/2000 LATEST CHK: 07/18/2001 WKLY BASIC BEN: 111. 00 BENEFIT PERIOD: 12/31/2000 THRU 12/30/2001 DEP ALLOWANCE: 36. 00 MAX BEN AMT: 2, 886. 00 MAX BEN BAL: WK BEN AMT: 147. 00 EMPLOYER ID/NAME/PLANT/ADDR/CITY/ST/ZIP ----- WAGES BY QUARTER ----- 1/2001 2/2001 3/2001 4/2001 1705724 EMPLOYER NO. 1 000 STREET ADDRESS CITY OR TOWN STATE ZIPCODE 252 92 4205110 EMPLOYER NO. 2 STREET ADDRESS CITY OR TOWN STATE ZIPCODE 1248 PAY DATE AMOUNT WKS PD PAY END-DT | PAY DATE AMOUNT WKS PD PAY END-DT 07/18/2001 147. 00 01 07/07/2001 | 07/05/2001 294. 00 02 06/30/2001 06/20/2001 294. 00 02 06/16/2001 | 06/06/2001 294. 00 02 06/02/2001 05/23/2001 294. 00 02 05/19/2001 | 05/09/2001 294. 00 02 05/05/2001 04/25/2001 294. 00 03 04/21/2001 |
 KIDS Case Information P 0 IMAOXX KEY INFORMATION DELIVERY SYSTEM 04/17/02 DHSDXXXX IV-D CASE INQUIRY PARTICIPANT LIST 11: 56: 30 PAGE: 1 IV-D NUM: C 00000001 PART S O LAST NAME FIRST NAME M RIN TYPE T T DOB REL SSN ========= = ===== = = ========= 1 ROBERTS BENJI 00001 CHLD A 2 08/13/1996 CHLD XXXXX 0001 2 ROBERTS JULIA 00002 CLI A 04/08/1967 MOTH XXXXX 0002 3 PRATT BENJAMIN P 000000099 RR A 12/09/1965 FATH 990000099 4 ROBERTS BENITO 00003 CHLD A 2 08/13/1996 CHLD XXXXX 0003 ENTER LINE NUM TO SELECT PART __ --------------------------------------- ENTER-SELECT PART PF 7 -UP PF 8 -DOWN PF 9 -CASE SUMMARY
KIDS Case Information P 0 IMAOXX KEY INFORMATION DELIVERY SYSTEM 04/17/02 DHSDXXXX IV-D CASE INQUIRY PARTICIPANT LIST 11: 56: 30 PAGE: 1 IV-D NUM: C 00000001 PART S O LAST NAME FIRST NAME M RIN TYPE T T DOB REL SSN ========= = ===== = = ========= 1 ROBERTS BENJI 00001 CHLD A 2 08/13/1996 CHLD XXXXX 0001 2 ROBERTS JULIA 00002 CLI A 04/08/1967 MOTH XXXXX 0002 3 PRATT BENJAMIN P 000000099 RR A 12/09/1965 FATH 990000099 4 ROBERTS BENITO 00003 CHLD A 2 08/13/1996 CHLD XXXXX 0003 ENTER LINE NUM TO SELECT PART __ --------------------------------------- ENTER-SELECT PART PF 7 -UP PF 8 -DOWN PF 9 -CASE SUMMARY
 KIDS Account Information P 4 IMAQAN KEY INFORMATION DELIVERY SYSTEM 05/10/06 DHSD 00000 DISBURSEMENTS TO CLIENT 11: 14: 58 *MORE* PAGE 1 PART NAME DOE JANE RIN 0000 SSN 111 -22 -3333 V V IV-D IV-A 94 -200 -000 AB 00000 DOCKET FIPS N MAIL DATE NCP RIN CASE NUM AMT N MAIL DATE NCP RIN CASE NUM AMT = ========= ======== 1 05/05/06 D 123456789 C 0000 7. 72 A 02/23/06 D 123456789 C 0000 27. 70 2 05/05/06 D 123456789 C 0000 30. 16 B 02/23/06 D 123456789 C 0000 108. 00 3 04/20/06 D 123456789 C 0000 27. 70 C 02/09/06 D 123456789 C 0000 27. 70 4 04/20/06 D 123456789 C 0000 108. 00 D 02/09/06 D 123456789 C 0000 108. 00 5 04/06/06 D 123456789 C 0000 3. 96 E 01/26/06 D 123456789 C 0000 7. 42 6 04/06/06 D 123456789 C 0000 15. 44 F 01/26/06 D 123456789 C 0000 28. 95 7 03/23/06 D 123456789 C 0000 27. 70 G 12/30/05 D 123456789 C 0000 20. 30 8 03/23/06 D 123456789 C 0000 108. 00 H 12/30/05 D 123456789 C 0000 79. 17 9 03/09/06 D 123456789 C 0000 15. 84 I 12/15/05 D 123456789 C 0000 27. 70 0 03/09/06 D 123456789 C 0000 61. 74 J 12/15/05 D 123456789 C 0000 108. 00 --------------------M=MAIL, D=DIRECT ENTER LN# _ OR NCP RIN _____ DATE BEGIN VIEW 05/10/2006
KIDS Account Information P 4 IMAQAN KEY INFORMATION DELIVERY SYSTEM 05/10/06 DHSD 00000 DISBURSEMENTS TO CLIENT 11: 14: 58 *MORE* PAGE 1 PART NAME DOE JANE RIN 0000 SSN 111 -22 -3333 V V IV-D IV-A 94 -200 -000 AB 00000 DOCKET FIPS N MAIL DATE NCP RIN CASE NUM AMT N MAIL DATE NCP RIN CASE NUM AMT = ========= ======== 1 05/05/06 D 123456789 C 0000 7. 72 A 02/23/06 D 123456789 C 0000 27. 70 2 05/05/06 D 123456789 C 0000 30. 16 B 02/23/06 D 123456789 C 0000 108. 00 3 04/20/06 D 123456789 C 0000 27. 70 C 02/09/06 D 123456789 C 0000 27. 70 4 04/20/06 D 123456789 C 0000 108. 00 D 02/09/06 D 123456789 C 0000 108. 00 5 04/06/06 D 123456789 C 0000 3. 96 E 01/26/06 D 123456789 C 0000 7. 42 6 04/06/06 D 123456789 C 0000 15. 44 F 01/26/06 D 123456789 C 0000 28. 95 7 03/23/06 D 123456789 C 0000 27. 70 G 12/30/05 D 123456789 C 0000 20. 30 8 03/23/06 D 123456789 C 0000 108. 00 H 12/30/05 D 123456789 C 0000 79. 17 9 03/09/06 D 123456789 C 0000 15. 84 I 12/15/05 D 123456789 C 0000 27. 70 0 03/09/06 D 123456789 C 0000 61. 74 J 12/15/05 D 123456789 C 0000 108. 00 --------------------M=MAIL, D=DIRECT ENTER LN# _ OR NCP RIN _____ DATE BEGIN VIEW 05/10/2006
 Chicago Student On Line PA 5027 AA ILLINOIS DEPARTMENT OF PUBLIC AID DATE: 05/10/06 TERMID: DHSD 000 CSOC INQUIRY RESPONSE REPORT TIME: 14: 18: 42 PAGE: 01 3(6 YEARS) INQUIRY CRITERIA: DOE JOHN 03/17/1996 CHICAGO STUDENT MATCHED BY: NAME AND BIRTH DATE JOHN , DOE 03/17/1996 ADDRESS: 1111 N CHICAGO PLACE GUARDIAN: JANE DOE REL TO STUDENT: MOTHER LEAVE DATE: REASON: SCHOOL NAME: ROBERT BATES ELEMENTARY SCHOO GRADE LEVEL: SECOND GRADE STUDENT DATABASE: 05/08/2003 SCHOOL DATABASE: 01/10/2002
Chicago Student On Line PA 5027 AA ILLINOIS DEPARTMENT OF PUBLIC AID DATE: 05/10/06 TERMID: DHSD 000 CSOC INQUIRY RESPONSE REPORT TIME: 14: 18: 42 PAGE: 01 3(6 YEARS) INQUIRY CRITERIA: DOE JOHN 03/17/1996 CHICAGO STUDENT MATCHED BY: NAME AND BIRTH DATE JOHN , DOE 03/17/1996 ADDRESS: 1111 N CHICAGO PLACE GUARDIAN: JANE DOE REL TO STUDENT: MOTHER LEAVE DATE: REASON: SCHOOL NAME: ROBERT BATES ELEMENTARY SCHOO GRADE LEVEL: SECOND GRADE STUDENT DATABASE: 05/08/2003 SCHOOL DATABASE: 01/10/2002
 CYS Policy
CYS Policy
 Collaboration BIG ISSUE: What do I do with a collaboration child no longer income eligible for the childcare program?
Collaboration BIG ISSUE: What do I do with a collaboration child no longer income eligible for the childcare program?
 Appeals Process
Appeals Process
 Appeals Process Types of Appeals Denial of benefits Cancellation of benefits Co-payment Payment amount or nonpayment of child care subsidy (Providers)
Appeals Process Types of Appeals Denial of benefits Cancellation of benefits Co-payment Payment amount or nonpayment of child care subsidy (Providers)
 Appeals Process Step 1: Client files an appeal Call 1 -800 -435 -0774 or send written appeal within 60 days the notice is signed and mailed (04. 01 IDHS Policy) Local IDHS office serving the client or IDHS Bureau of Assistance Hearing (BAH) or CYS or Delegate Agency or IDHS Bureau of Child Care and Development (BCCD) Step 2: CYS receives written appeal CYS forwards appeal to BAH within 48 hours
Appeals Process Step 1: Client files an appeal Call 1 -800 -435 -0774 or send written appeal within 60 days the notice is signed and mailed (04. 01 IDHS Policy) Local IDHS office serving the client or IDHS Bureau of Assistance Hearing (BAH) or CYS or Delegate Agency or IDHS Bureau of Child Care and Development (BCCD) Step 2: CYS receives written appeal CYS forwards appeal to BAH within 48 hours
 Appeals Process Step 3: Notification of appeals IDHS Local Office or CYS notifies BCCD that an appeal has been filed. Step 4: Hearing Scheduled BAH schedules the hearing, allowing BCCD at least 2 weeks to review the case and gather the required information and evidence.
Appeals Process Step 3: Notification of appeals IDHS Local Office or CYS notifies BCCD that an appeal has been filed. Step 4: Hearing Scheduled BAH schedules the hearing, allowing BCCD at least 2 weeks to review the case and gather the required information and evidence.
 Appeals Process Step 5: CYS receives notification of hearing Reviews the case CYS pre-hearing conference Attempts to resolve issue If issue is resolved, contact the child care appeals coordinator in Springfield.
Appeals Process Step 5: CYS receives notification of hearing Reviews the case CYS pre-hearing conference Attempts to resolve issue If issue is resolved, contact the child care appeals coordinator in Springfield.
 Appeals Process Step 6: Appeal Hearing by telephone BAH notifies appellant, CYS and local office of hearing decision
Appeals Process Step 6: Appeal Hearing by telephone BAH notifies appellant, CYS and local office of hearing decision
 Notice of Cancellation Appeals notification
Notice of Cancellation Appeals notification
 Denial Notice Appeals Notification
Denial Notice Appeals Notification