

272fa494dd1976ee6f82d79ea706cf2a.ppt
- Количество слайдов: 35
 • • Today Vitamins, minerals, & deficiency diseases Synergies between nutrition & disease Especially vulnerable populations 4 faces of hunger © T. M. Whitmore
• • Today Vitamins, minerals, & deficiency diseases Synergies between nutrition & disease Especially vulnerable populations 4 faces of hunger © T. M. Whitmore
 • Contemporary acute deficiency diseases: Iron deficiency: ØMost common single nutrient deficiency in the world § > 1/3 of pop in many developing countries ØReduces cognitive performance, energy and work ability, and resistance to infection (especially to diarrheal and respiratory diseases) even in mild cases ØSevere forms = anemia © T. M. Whitmore
• Contemporary acute deficiency diseases: Iron deficiency: ØMost common single nutrient deficiency in the world § > 1/3 of pop in many developing countries ØReduces cognitive performance, energy and work ability, and resistance to infection (especially to diarrheal and respiratory diseases) even in mild cases ØSevere forms = anemia © T. M. Whitmore
 • Contemporary acute deficiency diseases: Iodine deficiency: ØIodine is lacking in soils from some mountain areas and in domr highly leached soils § e, . g. , Andes, Himalayas, C Africa, SE Asia. . . ØMajor consequences: § Swelling of thyroid (goiter) § Important mental deficiencies (cretinism) in kids if deficient in pregnant women © T. M. Whitmore
• Contemporary acute deficiency diseases: Iodine deficiency: ØIodine is lacking in soils from some mountain areas and in domr highly leached soils § e, . g. , Andes, Himalayas, C Africa, SE Asia. . . ØMajor consequences: § Swelling of thyroid (goiter) § Important mental deficiencies (cretinism) in kids if deficient in pregnant women © T. M. Whitmore
 • Contemporary acute deficiency diseases: Vitamin A deficiency: ØMajor consequences § To vision can lead to blindness § Also decreased immune function § Kids with severe protein-calorie malnutrition often have impaired sight as a result of this © T. M. Whitmore
• Contemporary acute deficiency diseases: Vitamin A deficiency: ØMajor consequences § To vision can lead to blindness § Also decreased immune function § Kids with severe protein-calorie malnutrition often have impaired sight as a result of this © T. M. Whitmore
 => reduced") Synergy: nutrition and disease • Poor nutrition (protein-calorie or other nutrient shortages) => reduced ability to fend off new infections or makes existing ones more severe • Diseases interfere with nutrient absorption and/or actively deplete nutrients from our bodies © T. M. Whitmore
Synergy: nutrition and disease • Poor nutrition (protein-calorie or other nutrient shortages) => reduced ability to fend off new infections or makes existing ones more severe • Diseases interfere with nutrient absorption and/or actively deplete nutrients from our bodies © T. M. Whitmore
 • How poor nutrition => disease Reduction in the body's innate immunities (that react to general patterns of proteins in pathogens) ØLess effective phagocytosis (process by which microorganisms are engulfed and encapsulated) ØWeakened epithelial barriers (protective coverings on body surfaces inside and out) ØLowered lysozyme production (a bodily protein that functions as an antibacterial) © T. M. Whitmore
• How poor nutrition => disease Reduction in the body's innate immunities (that react to general patterns of proteins in pathogens) ØLess effective phagocytosis (process by which microorganisms are engulfed and encapsulated) ØWeakened epithelial barriers (protective coverings on body surfaces inside and out) ØLowered lysozyme production (a bodily protein that functions as an antibacterial) © T. M. Whitmore
 How poor nutrition => disease II • Reduction in ability to generate acquired immunities - the specific immunities one acquires to a particular disease pathogen ØReduced production of humoral antibodies ØImpaired cell-mediated immunity © T. M. Whitmore
How poor nutrition => disease II • Reduction in ability to generate acquired immunities - the specific immunities one acquires to a particular disease pathogen ØReduced production of humoral antibodies ØImpaired cell-mediated immunity © T. M. Whitmore
 • How disease => poor nutrition Most infections interfere with the body's ability to absorb nutrition and/or actively deplete nutrients ØReduced appetite ØPoorer quality of diet ingested ØDiseases deplete bodily tissue ØFevers => increased metabolic rate thus, the body needs more kcal but they may not be there © T. M. Whitmore
• How disease => poor nutrition Most infections interfere with the body's ability to absorb nutrition and/or actively deplete nutrients ØReduced appetite ØPoorer quality of diet ingested ØDiseases deplete bodily tissue ØFevers => increased metabolic rate thus, the body needs more kcal but they may not be there © T. M. Whitmore
 • • Special case of GI tract diseases 1. 8 billion cases/yr of infant/weanling GI diseases Predominantly diarrheas, but also intestinal parasites, cholera, & various types of dysentery Ø Impede absorption of nutrients (diarrheas just don't let food sit in gut long enough) © T. M. Whitmore
• • Special case of GI tract diseases 1. 8 billion cases/yr of infant/weanling GI diseases Predominantly diarrheas, but also intestinal parasites, cholera, & various types of dysentery Ø Impede absorption of nutrients (diarrheas just don't let food sit in gut long enough) © T. M. Whitmore
 • Special case of GI tract diseases II Many if not most deaths (perhaps 1 million/ yr in the world) can be averted with adequate treatment (called Oral Rehydration Therapy) ØAccording to The Lancet (1978), ORT is "potentially the most important medical discovery of the 20 th century" ØClean water with 60 cent packets of salts/sugars to recover health ØFull recovery => increased nutrition above basic levels – often hard to get © T. M. Whitmore
• Special case of GI tract diseases II Many if not most deaths (perhaps 1 million/ yr in the world) can be averted with adequate treatment (called Oral Rehydration Therapy) ØAccording to The Lancet (1978), ORT is "potentially the most important medical discovery of the 20 th century" ØClean water with 60 cent packets of salts/sugars to recover health ØFull recovery => increased nutrition above basic levels – often hard to get © T. M. Whitmore
 Oral Rehydration Therapy (home made)") Oral Rehydration Therapy (packet for addition to water) Oral Rehydration Therapy (home made)
Oral Rehydration Therapy (packet for addition to water) Oral Rehydration Therapy (home made)
 • • • Especially vulnerable populations I Increased likelihood of malnutrition and more serious consequences Women in general due to cultural traditions that privilege food to males Pregnant women ØPoor nutrition => low birth weight babies ØDevelopmental problems for baby physically and mentally ØReduced resistance to diseases ØLess able to breast feed (=> less resistance for the baby as well) © T. M. Whitmore
• • • Especially vulnerable populations I Increased likelihood of malnutrition and more serious consequences Women in general due to cultural traditions that privilege food to males Pregnant women ØPoor nutrition => low birth weight babies ØDevelopmental problems for baby physically and mentally ØReduced resistance to diseases ØLess able to breast feed (=> less resistance for the baby as well) © T. M. Whitmore
 • • Especially vulnerable populations II Lactating women ØPoor nutrition seldom greatly interferes with ability to produce milk ØBut, poor nutrition does deplete the mother's body of necessary nutrients ØIf nutrition is not better between end of lactation and next pregnancy => spiral down to chronic anemia etc. Elderly ØAbility to fend off infections is reduced with great age and malnutrition hurts that as well © T. M. Whitmore
• • Especially vulnerable populations II Lactating women ØPoor nutrition seldom greatly interferes with ability to produce milk ØBut, poor nutrition does deplete the mother's body of necessary nutrients ØIf nutrition is not better between end of lactation and next pregnancy => spiral down to chronic anemia etc. Elderly ØAbility to fend off infections is reduced with great age and malnutrition hurts that as well © T. M. Whitmore
 • Especially vulnerable populations III Children ØMalnutrition in infants and children very problematic if timing coincides with critical growth processes § Up to age 5 risk is greatest ØEspecially at weaning age (approx 2 yrs) ØDue to impure water used to make weaning foods (not sufficiently boiled due to lack of fuel) and general low hygiene => § Kids die from diarrheal diseases and dehydration and malnutrition ØWeaning foods are typically not nutrient© T. M. Whitmore rich enough (e. g. , maize gruels)
• Especially vulnerable populations III Children ØMalnutrition in infants and children very problematic if timing coincides with critical growth processes § Up to age 5 risk is greatest ØEspecially at weaning age (approx 2 yrs) ØDue to impure water used to make weaning foods (not sufficiently boiled due to lack of fuel) and general low hygiene => § Kids die from diarrheal diseases and dehydration and malnutrition ØWeaning foods are typically not nutrient© T. M. Whitmore rich enough (e. g. , maize gruels)
 • Four Faces of Hunger I I. Starvation/Famine ØWidespread to complete lack of protein/calorie nutrition ØA small percentage of global hunger – perhaps 1% at risk annually ØLeads to increased mortality (usually to infectious diseases not starvation per se) ØGreat social disruption => increased problems with diseases and access to food ØIn any famine not all starve – the well off can buy food -- thus NOT usually only a simple shortage © T. M. Whitmore
• Four Faces of Hunger I I. Starvation/Famine ØWidespread to complete lack of protein/calorie nutrition ØA small percentage of global hunger – perhaps 1% at risk annually ØLeads to increased mortality (usually to infectious diseases not starvation per se) ØGreat social disruption => increased problems with diseases and access to food ØIn any famine not all starve – the well off can buy food -- thus NOT usually only a simple shortage © T. M. Whitmore
 • Four Faces of Hunger II II. Malnutrition/Undernutrition ØSeasonal or periodic P/C under-nutrition ØMost serious effects on kids and special needs adults (pregnant and lactating women, the elderly) Ø measures of malnutrition in children § Stunting - stature too short for age/sex (adjusted for local norms) => chronic § Wasting – weight too light for age/sex (adjusted for local norms) => acute © T. M. Whitmore
• Four Faces of Hunger II II. Malnutrition/Undernutrition ØSeasonal or periodic P/C under-nutrition ØMost serious effects on kids and special needs adults (pregnant and lactating women, the elderly) Ø measures of malnutrition in children § Stunting - stature too short for age/sex (adjusted for local norms) => chronic § Wasting – weight too light for age/sex (adjusted for local norms) => acute © T. M. Whitmore
 • Four Faces of Hunger III. Micro-nutrient deficiencies Ø Vitamin and mineral shortages • ØSometimes called “hidden hunger” IV. Nutrition-depleting illnesses ØSecondary malnutrition ØMost common nutrient depleting diseases are infant/weanling diarrheas – 5 million deaths annually world wide © T. M. Whitmore
• Four Faces of Hunger III. Micro-nutrient deficiencies Ø Vitamin and mineral shortages • ØSometimes called “hidden hunger” IV. Nutrition-depleting illnesses ØSecondary malnutrition ØMost common nutrient depleting diseases are infant/weanling diarrheas – 5 million deaths annually world wide © T. M. Whitmore
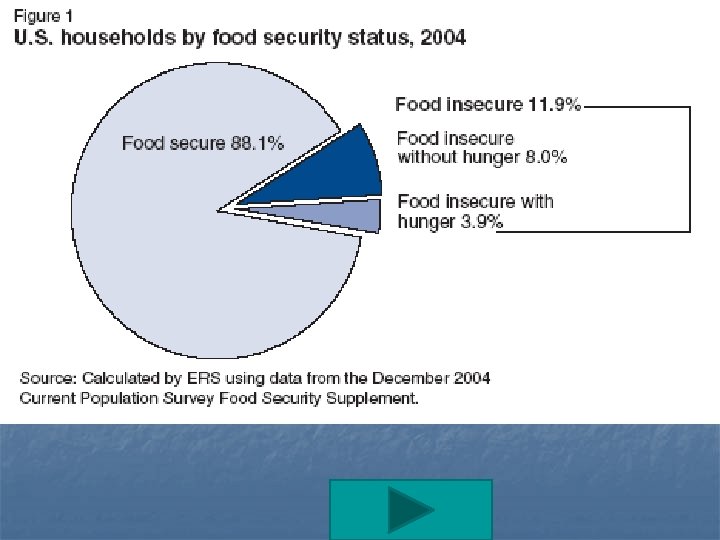
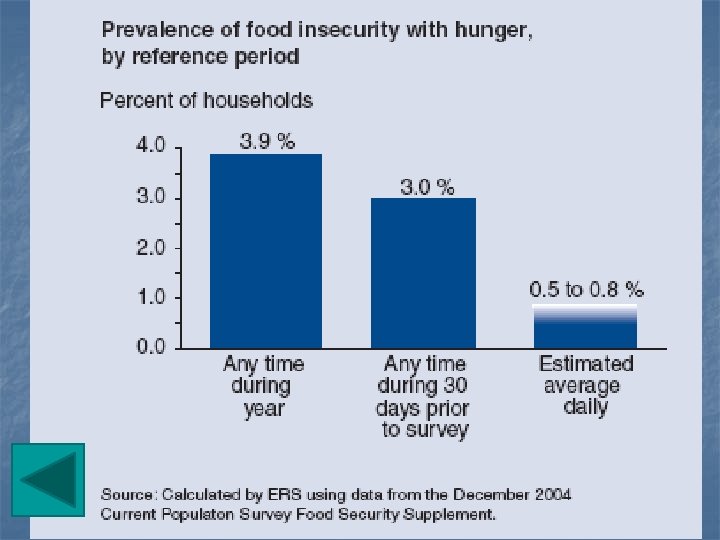
 • • • Global Hunger Global situation late 1990 s Data drawn from FAO’s SOFA report 2007 http: //www. fao. org/docrep/010/a 1200 e 00. htm The International Food Policy Research Institute: http: //www. ifpri. org/media/20071012 GHI. asp The concept of “food security” © T. M. Whitmore
• • • Global Hunger Global situation late 1990 s Data drawn from FAO’s SOFA report 2007 http: //www. fao. org/docrep/010/a 1200 e 00. htm The International Food Policy Research Institute: http: //www. ifpri. org/media/20071012 GHI. asp The concept of “food security” © T. M. Whitmore
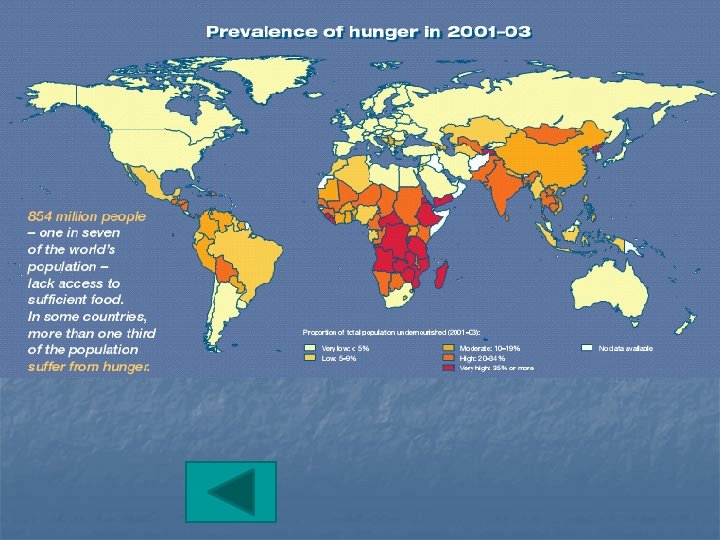
 ØLate") • • Global Trajectories of Hunger I Proportions undernourished (or food insecure) ØLate 1970 s ~ 28% ØLate 1990 s ~17% ØThus, some real progress ØLess progress in absolute numbers Micro-nutrient deficiencies ØIron: 40% of global south ØIodine: 12% of global south ØVitamin A: 14% of kids in global south © T. M. Whitmore
• • Global Trajectories of Hunger I Proportions undernourished (or food insecure) ØLate 1970 s ~ 28% ØLate 1990 s ~17% ØThus, some real progress ØLess progress in absolute numbers Micro-nutrient deficiencies ØIron: 40% of global south ØIodine: 12% of global south ØVitamin A: 14% of kids in global south © T. M. Whitmore
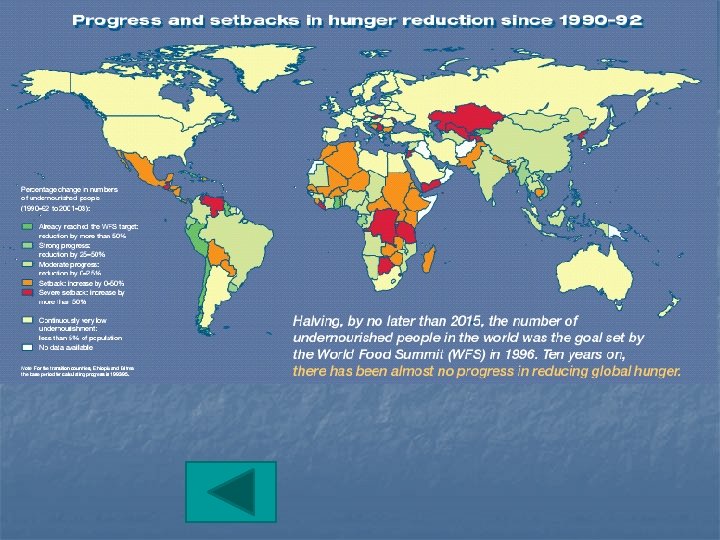
") Global Trajectories of Hunger II • • • Absolute numbers undernourished (or food insecure) Ø 1970 s ~ 900 m; 2000 ~ > 800 m Ø=> decrease of ~ 100 m in absolute numbers (but smaller %) Children 1993 ~ 200 m; now ~ 175 m World food summit target (MDG) in 2015 => 400 m ØCurrent trajectory => 475 -500 m by 2015 ØProgress in some places, regression in others © T. M. Whitmore
Global Trajectories of Hunger II • • • Absolute numbers undernourished (or food insecure) Ø 1970 s ~ 900 m; 2000 ~ > 800 m Ø=> decrease of ~ 100 m in absolute numbers (but smaller %) Children 1993 ~ 200 m; now ~ 175 m World food summit target (MDG) in 2015 => 400 m ØCurrent trajectory => 475 -500 m by 2015 ØProgress in some places, regression in others © T. M. Whitmore
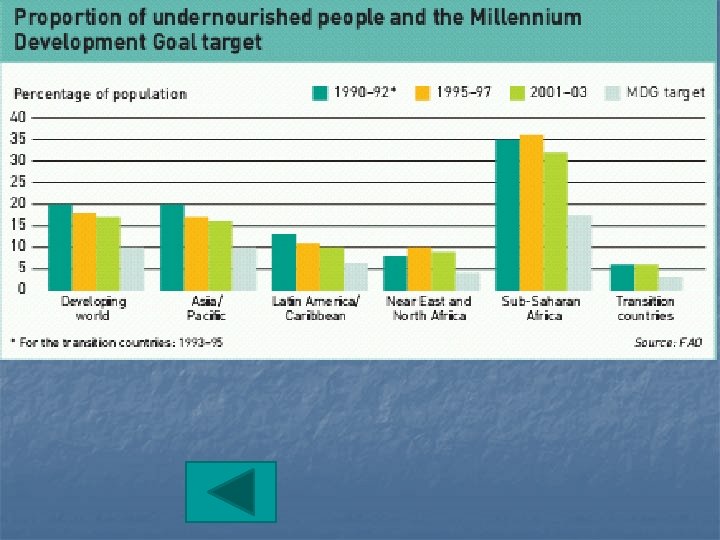
 • • Regional differences malnourished or food insecure Global South ØSub-Saharan Africa ØE. Asia, SE Asia, & Pacific ØSouth Asia ØLatin America & Caribbean ØNear East & N. Africa Developed Economies (mostly N America) © T. M. Whitmore
• • Regional differences malnourished or food insecure Global South ØSub-Saharan Africa ØE. Asia, SE Asia, & Pacific ØSouth Asia ØLatin America & Caribbean ØNear East & N. Africa Developed Economies (mostly N America) © T. M. Whitmore
 Source: FAO
Source: FAO

 Source: FAO
Source: FAO
 Source: FAO SOFA 2007
Source: FAO SOFA 2007
 Number of malnourished children, 1993, 2010, and 2020 Source: IFPRI IMPACT simulations.
Number of malnourished children, 1993, 2010, and 2020 Source: IFPRI IMPACT simulations.
 Source: IFPRI Global Hunger Index 2007
Source: IFPRI Global Hunger Index 2007
 Source: FAO SOFA 2007
Source: FAO SOFA 2007
 Countries with food shortfalls – requiring assistance
Countries with food shortfalls – requiring assistance