bdd32d83608b406f2404a755ba0b0667.ppt
- Количество слайдов: 69



Thrombotic Disorders : Diagnosis and Treatment Michael Laposata, M. D. , Ph. D Edward and Nancy Fody Professor of Pathology Vanderbilt University School of Medicine Pathologist in Chief, Vanderbilt University Hospital

Thrombotic Disorders : Diagnosis and Treatment Michael Laposata, M. D. , Ph. D I have no disclosures to make that are relevant to this presentation and will make no reference to any specific product or company with which I am connected.

Thrombotic Disorders : Diagnosis and Treatment • Identify the most common genetic causes for thrombosis. • Learn the diagnostic tests used to identify genetic predisposition to thrombosis. • Learn the prophylaxis and treatment of hypercoagulable states.

Thrombotic Disorders : Diagnosis and Treatment Which of the following is the most common congenital cause for hypercoagulability? a) protein C deficiency b) protein S deficiency c) antithrombin III deficiency d) activated protein C resistance with the factor V Leiden

Hypercoagulability and Risk for Thrombosis When should you consider this and what tests should you order ?

Overview of Presentation • Background on hypercoagulable states • Description of : -Factor V Leiden -Prothrombin 20210 mutation -Protein C, Protein S and Antithrombin Deficiencies -Heparin-Induced Thrombocytopenia -Antiphospholipid Antibodies


CLOT FORMATION Vessel Wall Injury ------Platelet Adhesion Fibrin Formation Vessel Wall Contraction ------Platelet Aggregation

THROMBOSIS FORMATION – A USEFUL CLOT BECOMES A DAMAGING THROMBOSIS

The Appropriate Level of Hemostasis Bleeding Thrombosis Balance

Too Much Anticoagulation in a Thrombotic patient 2 Bleeding 1 Balance Thrombosis
 Surgery Immobilization Malignancy Pregnancy Oral Contraceptives")
COMMONLY ENCOUNTERED ACQUIRED RISK FACTORS Heparin-Induced Thrombocytopenia (HIT) Surgery Immobilization Malignancy Pregnancy Oral Contraceptives Estrogen Replacement Therapy Lupus Anticoagulant Anticardiolipin & Anti-Beta 2 Glycoprotein 1 Antibody Obesity Smoking

THE MOST COMMON HEREDITARY RISK FACTORS Activated protein C resistance Nearly always the factor V Leiden mutation May be heterozygous or homozygous Prothrombin G 20210 A mutation May be heterozygous or homozygous

LESS COMMON HEREDITARY RISK FACTORS Protein C deficiency Essentially always heterozygous Protein S deficiency Essentially always heterozygous Antithrombin deficiency Essentially always heterozygous

THE “SECOND HIT” THEORY FOR INITIATION OF THROMBOSIS The presence of more than one risk factor is needed to manifest thrombosis in most patients EXAMPLE: 1 Congenital 1 Acquired + Risk Factor = Thrombosis Risk Factor

Most People Have More Than 1 Risk Factor for Thrombosis Plane Ride Injury to Leg PROPHYLAXIS Injury to Leg NO THROMBOSIS ANTICOAGULANT THROMBOSIS RISK THROMBOSIS OCP Factor V Leiden At Birth OCP Factor V V V Leiden At 25 yo At 38 yo At 43 yo

Activated Protein C Resistance & The Factor V Leiden Mutation

RESISTANCE TO ACTIVATED PROTEIN C Anticoagulant Activity Factor V Procoagulant Activity • The factor V Leiden mutation produces a change in amino acid 506 • The factor V Leiden mutation does not affect the procoagulant activity of factor V

RESISTANCE TO ACTIVATED PROTEIN C AND THE FACTOR V LEIDEN MUTATION • The most remarkable feature of the factor V Leiden mutation is its high prevalence • It is found in about 50% of caucasian patients with familial thrombophilia, in 20% of all caucasian patients with a deep vein thrombosis, and in 3 -5% of the general caucasian population

Am J Med 2004; 116: 435 -442

RESISTANCE TO ACTIVATED PROTEIN C AND THE FACTOR V LEIDEN MUTATION • Factor V Leiden is the most commonly encountered risk factor for deep-vein thrombosis • Its role in arterial thrombosis remains unclear

RESISTANCE TO ACTIVATED PROTEIN C AND THE FACTOR V LEIDEN MUTATION • Oral contraceptives greatly increase the risk of thrombosis in patients with factor V Leiden • For women aged 15 to 49 who carry the mutation and use oral contraceptives, the risk of venous thrombosis is approximately 30 per 10, 000 per year, representing at least a 30 -fold increased risk

N. Engl. J. Med. 344, 1527, 2001

The Prothrombin 20210 Mutation

PROTHROMBIN MUTATION G 20210 A • Mutation at position 20210 in the prothrombin gene • Associated with elevated prothrombin (factor II) levels • High prevalence -1 - 3% of the general caucasian population - 5 - 10% of caucasian patients with thrombosis - up to 20% of caucasian patients with familial thrombosis • 3 -Fold increased risk of venous thrombosis in heterozygous individuals

PROTHROMBIN 20210 AND FACTOR V LEIDEN MUTATIONS TOGETHER ARE VERY PROTHROMBOTIC • The G 20210 A prothrombin-gene mutation and factor V Leiden individually are associated with an increased risk of venous thromboembolism • The risk among patients with both mutations is disproportionately higher than that among those with only one mutation N. Engl. J. Med. , 342: 374, 2000

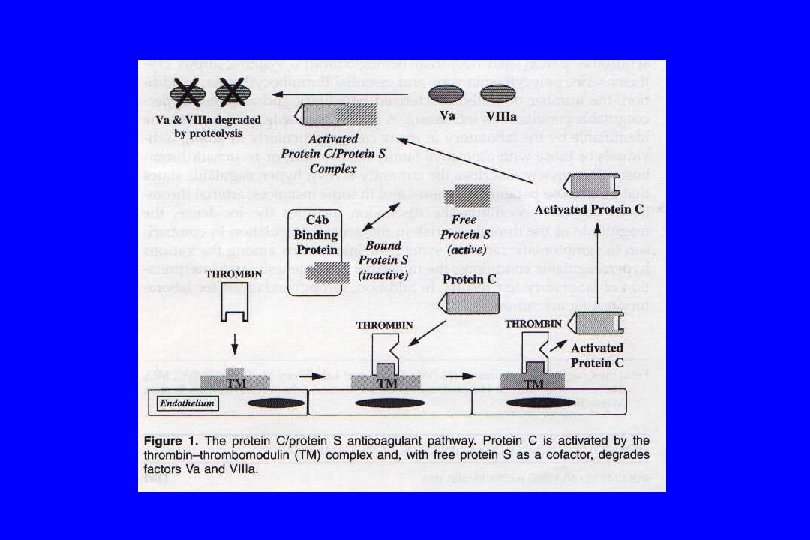
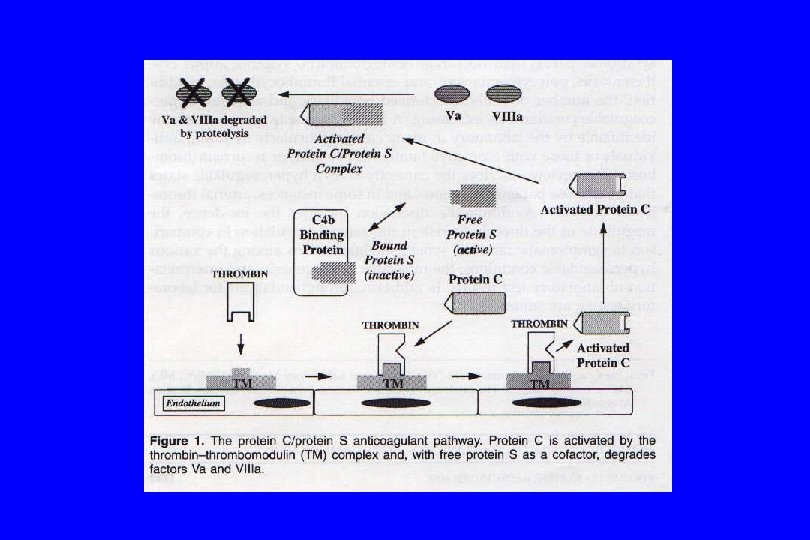
Protein C Deficiency
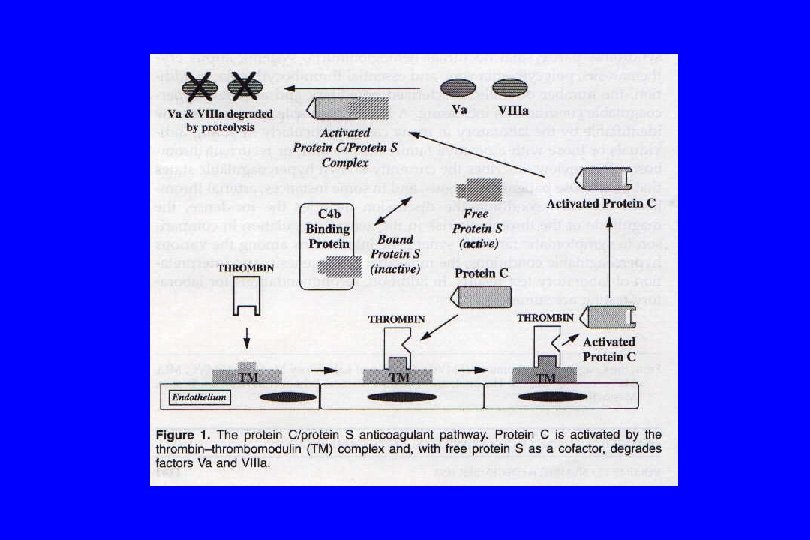

Protein S Deficiency

Antithrombin Deficiency

THE ANTITHROMBIN PATHWAY + + AT + Heparin + + AT Xa Heparin AT: Antithrombin + AT Antithrombin Conformational Change Heparin Inhibition of Xa + + AT Thrombin (IIa) + Heparin Inhibition of Thrombin

ANTITHROMBIN DEFICIENCY Antithrombin deficient patients may be moderately to severely heparin resistant and may require transfusion to increase their antithrombin level and permit an immediate heparin response

GENETIC DEFICIENCIES OF PROTEIN C, PROTEIN S, AND ANTITHROMBIN • The patients presenting with thrombosis are virtually always heterozygous patients with levels in the 40 -60% range • Homozygous deficiency is associated with values of less than 10% and death in infancy

Prevalence of Inherited Risk Factors for Thrombosis % of Population Factor V Leiden Prothrombin 20210 Low protein C Low Protein S Low Antithrombin 5. 0 (Caucasians) 2. 5 (Caucasians) 0. 2 -0. 4 0. 02 -0. 04

DATES OF DISCOVERY OF GENETIC RISK FACTORS FOR THROMBOSIS 1965 1980’s 1993 1996 Antithrombin III deficiency Protein C and protein S deficiency Activated protein C resistance (Factor V Leiden Mutation) Prothrombin G 20210 A Mutation

Genetically caused deficiencies of Protein C, Protein S and Antithrombin produce a risk for thrombosis -but if these deficiencies are acquired, they rarely represent an increased risk for thrombosis

ACQUIRED CONDITIONS OR TREATMENTS THAT DECREASE BOTH THE ANTICOAGULANT FACTORS AND THE PROCOAGULANT FACTORS Protein C Protein S Clot Formation Liver Disease Coumadin DIC Vitamin K Deficiency Heparin Antithrombin

ACQUIRED CONDITIONS OR TREATMENTS THAT DECREASE PROTEIN S SELECTIVELY AND DO NOT INCREASE THROMBOTIC RISK ON THE BASIS OF A LOW PROTEIN S Protein C Protein S Antithrombin Oral Contraceptives Estrogen Therapy Pregnancy Any Stimulus to Acute Phase Response
 Antiphospholipid Antibodies")
COMMONLY ENCOUNTERED LABORATORY DEFINED ACQUIRED RISK FACTORS FOR THROMBOSIS Heparin-Induced Thrombocytopenia (HIT) Antiphospholipid Antibodies : Lupus Anticoagulant Anticardiolipin Antibodies Anti-Beta 2 Glycoprotein 1 Antibodies

If there has been previous exposure to heparin or low molecular weight heparin, consider heparin – induced thrombocytopenia (HIT) as a cause for thrombosis

HEPARIN-INDUCED THROMBOCYTOPENIA Onset 4 -15 days after 1 st dose Moderate thrombocytopenia For this reason, must obtain platelet count before starting heparin therapy and monitor platelets at least every few days during heparin therapy

Proposed mechanism for the pathogenesis of heparininduced thrombocytopenia Courtesy of EM Van Cott, MD

NOT EVERYONE WITH AN HIT ANTIBODY DEVELOPS A CLOT Warkentin, T. , A. Greinacher. 2001. Heparin-Induced Thrombocytopenia: Second Edition. Marcel Dekker, Inc. New York, NY

The Consequences of Thrombosis in HIT are Often Severe Recovery 40 -60% Permanent Disability (amputation, stroke) 20 -30% Mortality 20 -30% Van Cott EM. Heparin-induced thrombocytopenia. Turnaround Times 1996; 5: 7 -11

ANTIPHOSPHOLIPID ANTIBODIES • Anticardiolipin antibodies • Antibodies to Beta 2 Glycoprotein I • Lupus anticoagulants ACL and/or Anti-Beta 2 GP I LA 25% 50% 25%

Courtesy of Dr. Alexander Kratz

Courtesy of Dr. Alexander Kratz

Courtesy of Dr. Alexander Kratz

Thrombotic Manifestations of Antiphospholipid Antibody Syndrome • Venous thrombosis more common than arterial • Venous thrombosis most common in the calf • Arterial thrombosis most common in the cerebral circulation

ELEVATED ANTIBETA 2 GLYCOPROTEIN 1 ANTIBODIES BASIS FOR POSITIVE TESTS FOR LUPUS ANTICOAGULANT, ANTICARDIOLIPIN ANTIBODIES AND ANTIBETA 2 GLYCOPROTEIN 1 ANTIBODIES The Clotting Times, Vol 5, Issue 3, 2005

INCIDENCE OF ANTIPHOSPHOLIPID ANTIBODIES • General population 3 -5% with increased frequency in older populations • Recent infection • HIV-positive • SLE patients 30% 20 -42% 18 -86%

ANTIPHOSPHOLIPID ANTIBODY SYNDROME: INTERNATIONAL CONSENSUS STATEMENT • Clinical criteria - Vascular thrombosis: one or more clinical episodes of thrombosis in any tissue or organ - Pregnancy complications: a) 1 unexplained fetal loss at or after 10 th week b) 1 premature birth at or before 34 th week c) 3 unexplained spontaneous abortions before 10 th week of gestation • Laboratory criteria - Moderate to high levels of Ig. G or Ig. M ACA or beta 2 glycoprotein I on two or more occasions at least 12 weeks apart - LA Abs detected on two or more occasions at least 12 weeks apart Need 1 clinical and 1 lab criterion for APA syndrome diagnosis

Who should be tested and when should the person be tested ? If there is any previous heparin or low molecular weight heparin exposure, add testing for HIT into the recommendations that follow

NON-CONTROVERSIAL SETTINGS IN THE U. S. The patient with multiple episodes or a clinically severe single episode of venous thrombosis • With the Leiden, Prothrombin 20210, C, S, AT, and APL Ab (LA with ACL or ABeta 2 GP 1 Ab) The patient with a single episode of venous thrombosis and a family history of venous thrombosis – • With the Leiden, Prothrombin 20210, C, S, and AT

NON-CONTROVERSIAL SETTINGS IN THE U. S. The woman with multiple fetal losses and no other identifiable cause • With the Leiden, Prothrombin 20210, C, S, AT, and APL Ab (LA with ACL or ABeta 2 GP 1 Ab) The patient with a stroke and a PFO that could allow a venous clot to enter the cerebral circulation – • With the Leiden, Prothrombin 20210, C, S, AT, and APL Ab (LA with ACL or ABeta 2 GP 1 Ab)

NON-CONTROVERSIAL SETTINGS IN THE U. S. The woman who is planning to use oral contraceptives and a family history of thrombosis • With the Leiden and Prothrombin 20210 is a reasonable approach The patient with a relative with a venous thrombosis and a heritable hypercoagulable state • With the marker for hypercoagulability found in the relative

CONTROVERSIAL CLINICAL SETTINGS The patient with an MI or peripheral arterial thrombosis or a stroke patient with no PFO • With the APL Ab (LA with ACL or ABeta 2 GP 1 Ab) because it can be a venous or arterial thrombotic risk factor is a reasonable approach The patient of Asian or African descent and no known causcasian ancestry • With the C, S, AT, and APL Ab (LA with ACL or ABeta 2 GP 1 Ab) is a reasonable approach

CONTROVERSIAL CLINICAL SETTINGS The woman who is planning to use oral contraceptives and has no family history of thrombosis • With the Leiden and Prothrombin 20210 is a reasonable approach The concerned patient who wants to know so that he or she carefully avoids the acquired risk factors for thrombosis • Minimally with the Leiden and Prothrombin 20210

WHEN NOT TO TEST THE PATIENT Activated protein C resistance • APC Resistance test suffers interference with lupus anticoagulant, argatroban, lepirudin • No interference with genetic test for Factor V Leiden Prothrombin G 20210 A mutation – • No interference with genetic test for 20210

WHEN NOT TO TEST THE PATIENT Protein C deficiency • Interference with warfarin-wait 10 -14 days after discontinuation Protein S deficiency – • Interference with warfarin-wait 10 -14 days after discontinuation • Wait 2 -3 months after delivery • Wait > 1 month after estrogen supplementation Antithrombin deficiency • Wait 1 -2 weeks after discontinuation of heparin or LMW heparin

WHEN NOT TO TEST THE PATIENT Protein C deficiency • Active Clotting ? Protein S deficiency – • Active Clotting ? Antithrombin deficiency • Active Clotting ?

Overview of Treatment of Hypercoagulable States

Duration of Warfarin Therapy 6 months vs. lifelong in most cases FACTORS TO CONSIDER – • Is this the first thrombotic event or a recurrence? • Which acquired risk factors were present at the time of initial clot formation and can they be removed? • Which genetic risk factors for thrombosis does the patient have and is there more than 1? • Does the patient have a bleeding problem or other factor that prevents coumadin use? • What was the clinical severity of the clot?

Achieving a Consensus on Warfarin Duration Most decide Much disagreement Most decide against lifelong on duration – even for lifelong anticoagulation among experts anticoagulation History of Mild Clot or Low Risk History of Severe Clot or High Risk

Summary of Presentation • Background on hypercoagulable states • Description of : -Factor V Leiden -Prothrombin 20210 mutation -Protein C, Protein S and Antithrombin Deficiencies -Heparin-Induced Thrombocytopenia -Antiphospholipid Antibodies
bdd32d83608b406f2404a755ba0b0667.ppt