
The Urinary System Functions of the Urinary System



 Right kidney usually 1.5-2cm caudal")









 Active transport: electrolytes,")

")





 Identify donor")
. Primary incision (non-laparoscope) www.viscom.ohiou.edu/kring/home.html")
. Locate and prepare kidney")
. Locate and prepare kidney")
. Locate and prepare kidney")
. Locate and prepare kidney")
. Locate and prepare kidney")
. Locate and prepare kidney")
.")
.")
 Kidney stones are hard pellets formed in the nephron as minerals")
 If permitted to nucleate large enough, stones can lodge in the")




 Normally linked to urinary tract infection. Treatments: Antibiotic therapy")
 linked to genetic defect in the intestinal")
 Genetic disease resulting in gradual kidney degeneration due to cyst")

 uses the patients peritoneal membrane as the")
9540-the_urinary_system.ppt
- Количество слайдов: 45
The Urinary System
Functions of the Urinary System Provide control over plasma/body electrolyte & water balance Maintains plasma osmolarity Maintains plasma pH Excrete nitrogenous waste (urea & creatine) Nitrogenous wastes often generated by amino acid metabolism Excrete drugs & other metabolites Urinary drug tests
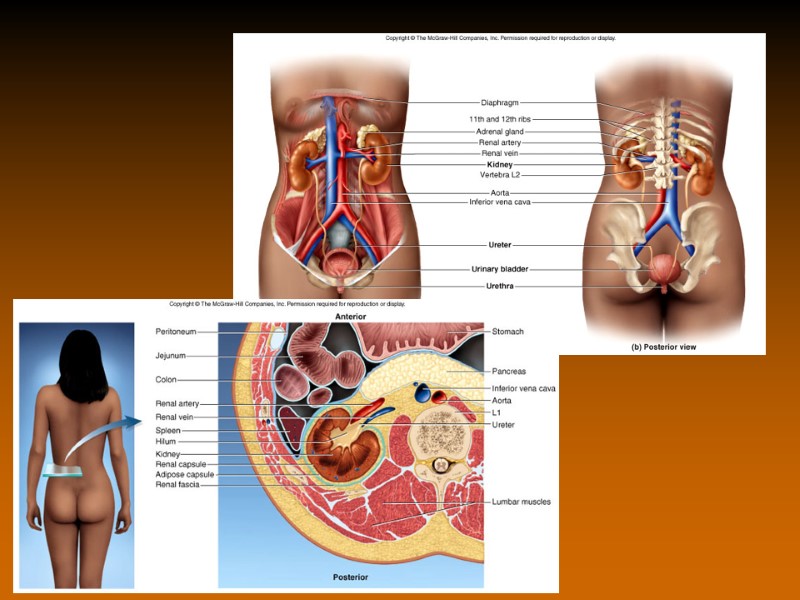
Anatomical Location Posterior abdominal cavity Retroperitoneal (behind the peritoneum) Right kidney usually 1.5-2cm caudal than left Kidneys connected to bladder via ureters Bladder located at anterior base of the pelvis
Gross Renal Anatomy Kidneys covered by “capsule” Intimate to kidney = Fibrous capsule Semi-transparent fibrous connective tissue Can be seen on male cadaver as a white layer Layer of adipose connective tissue Renal fascia that anchors kidney to abdominal wall & peritoneum
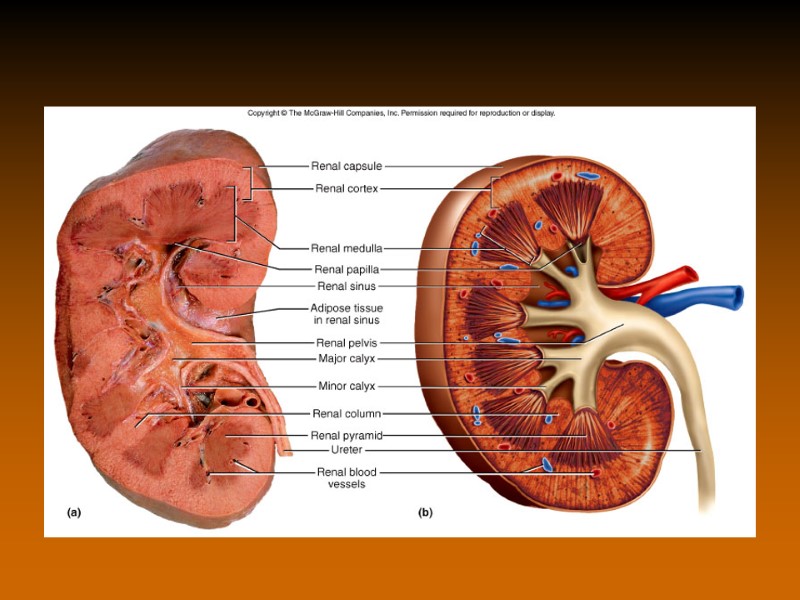
Gross Renal Anatomy Bisect the kidney and you see some key gross anatomical features: Outer cortex (red due to dense capillary network) Inner medulla region (dark red due to tubules & vasculature) Usually 8-15 renal pyramids separated by renal columns Apex of each renal pyramid = renal papillae (acts like a funnel) Renal papillae anastomize into minor calyx Minor calyces anastomize into major calyx
Microscopic Renal Anatomy Microscopically, the nephron is the functional unit of the kidney Over 1 million per kidney Knowledge of bloodflow pattern through kidney is very helpful in understanding kidney function Renal artery – interlobar arteries – arcuate arteries – interlobular arteries – afferent glomerular arterioles Afferent glomerular arterioles carry blood to the initial region of the nephron (glomerulus) Remember the gradient of pressure: highest in artery, lowest in capillary Arterioles retain enough pressure to permit the “filtration” to occur
Microscopic Renal Anatomy
Nephron Glomerulus is a very complicated structure whose architecture is vital for kidney filtration Capillary bed is squished into a ball (glomerulus) Capillary bed is fenestrated (large windows, but not as big as sinusoids in liver) Capillary is “encased” by unique cells = “podocytes” (foot cells) Podocytes extend “pedicels” onto the capillary body Between each foot or pedicel = “filtration space” where plasma contents can filter through glomerulus into the Bowman’s capsule (glomerular capsule)
The podocyte / pedicel structure is akin to the astrocytes in the blood – brain barrier. The podocytes & astrocytes wrap themselves around the capillary bed in their respective region. In the nephron, the podocytes allow MORE plasma to filter through than the astrocytes in the brain.
Nephron Once plasma has filtered out of the glomerulus, it enters the Bowman’s capsule (glomerular capsule) A funnel-like structure that initiates the nephron tubule network Into the proximal convoluted tubule Simple cuboidal epithelium with a distinctive apical brush border/microvillus structure Region of solute re-absorption Into the loop of Henle (nephron loop) Then “up” the distal convoluted tubule Simple cuboidal epithelium with markedly less apical brush border structure Region of water re-absorption This loop structure, which places the proximal tubule in very close approximation to the distal tubule = countercurrent exchange mechanism
Idealized tubule URINE
Idealized tubule
glomerulus PCT DCT “Concentrated” (plasma has been filtered out at glomerulus) Active transport: electrolytes, glucose, proteins etc. Slightly hypertonic, “extra-concentrated” “osmotic drag” of water Water-diluted blood, now iso-osmotic Afferent arteriole Efferent arteriole Vasa recta (tubule capillary network)
Ureter Urine flows from distal convoluted tubule – collecting duct – renal papilla – minor calyx – major calyx – renal pelvis – ureter Series of “collecting funnels” From renal pelvis –posterolateral edge of the bladder 3 layers of tissue (markedly similar to intestinal tract) Inner muscosa (forms continuous “sheet” from renal tubule – bladder) Known as “transitional epithelium”…can stretch Middle muscularis (opposite of the GI tract) Innermost layer (intimate to mucosa) = longitudinal muscle Outermost layer = circular muscle Outer Adventitia
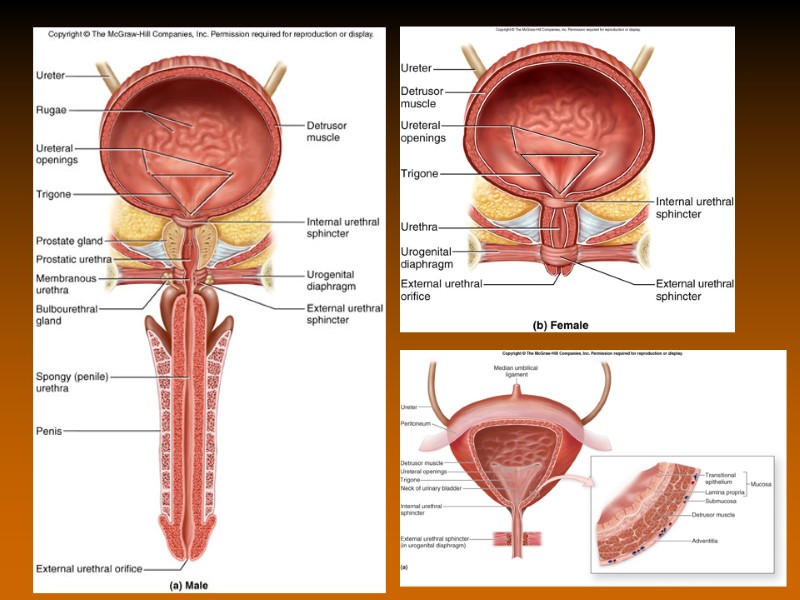
Bladder Posterior to pubic symphysis 4 layer organ Internal mucosa (transitional epithelium like ureter) Folded into “urinary bladder rugae” in order to allow bladder distension Region of the trigone (urethral opening) does not have rugae Submucosa Muscularis 3 layers of smooth muscle, similar to stomach “detrusor muscle” = combined 3 layers Base of trigone = neck = internal urinary/urethral sphincter Adventitia (actually parietal peritoneum)
Urethra Tube similar to ureter Lined with urethral glands that secrete mucus in order to protect lining Short distance between internal urinary/urethral sphincter (smooth muscle) and external urinary/urethral sphincter Note that the external urinary sphincter is NOT at the very end of the urethra Also recall how external urinary sphincter = skeletal muscle of the pelvic diaphragm Actual constrictor muscle group = bulbous spongiosum
Urethra Male vs female slightly different Female urethra short and relatively “straight” Urethral orifice located between labia minora A single-use tube (only for excretion of urine) Short & straight = more prone to infection (similar to estuchian canal of the middle ear) Male urethra longer and “S” shaped, divided into 3 regions: Prostatic: region passing through prostate gland Receives prostate excretions & ejaculatory fluid Membranous: region that passes through pelvic diaphragm Location of the external urinary sphincter Spongy: longest portion, to external urethral orifice Where bulbourethral glands (Cowper’s glands) secrete pre-ejaculate lubricant into urethra A DOUBLE-USE tube: urine & reproduction/ejaculate
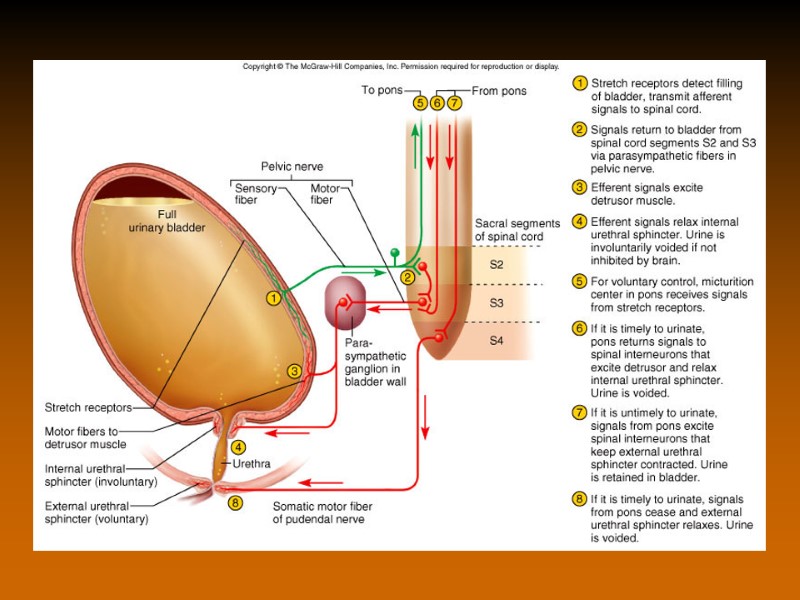
Urination / Micturation Reflex action to expel stored urine In infants/young, this is a simple reflex Voluntary control not developed until 2-3 years Requires development of cerebral cortex & maturation of the spinal cord (recall the cauda equina) Bladder can normally hold 1-1.5 liters of urine! 200-300 ml urine is enough to trigger the distension reflex that tells you that it’s time Stretch receptors trigger the micturation reflex PNS triggers detrusor muscle contraction & internal urinary sphincter relaxation Pudental nerve controls external urinary sphincter (bulbous spongiosum)
Kidney transplants Kidney transplants are the most frequently transplanted organs in the world. 12,000 kidney transplant procedures per year in USA alone. Donor kidneys can be harvested from two sources: Living donor (identical twin, serotype match) Cadaver
Why Transplant a Kidney? Indications for kidney transplant include: Diabetes, glomerulonephritis, polycystic kidney disease, pyelonephritis. End goals of the transplant include: Improved quality of life, reduce patient care costs and strain on healthcare provider. Reduce/remove the need for dialysis or CAPD (Continuous Ambulatory Peritoneal Dialysis). Remove dietary restrictions.
Kidney Transplant Procedure Identify acceptable patient (one that will tolerate transplant surgery) Identify donor organ (living donor or cadaver). Prepare patient (council, prophylactic immunosuppressant drugs, etc.) www.viscom.ohiou.edu/kring/home.html Donor is placed on their side to permit access to the donor kidney.
Kidney Transplant Procedure Surgical removal of donor kidney (living donor). Primary incision (non-laparoscope) www.viscom.ohiou.edu/kring/home.html
Kidney Transplant Procedure Surgical removal of donor kidney (living donor). Locate and prepare kidney for removal. Entering the kidney capsid (connective tissue anchoring the kidney to the dorsal abdomen) www.viscom.ohiou.edu/kring/home.html
Kidney Transplant Procedure Surgical removal of donor kidney (living donor). Locate and prepare kidney for removal. Ligating renal vasculature and ureter prior to removal www.viscom.ohiou.edu/kring/home.html
Kidney Transplant Procedure Surgical removal of donor kidney (living donor). Locate and prepare kidney for removal. All attempts are made to include as much vasculature and ureter as possible. www.kidneytransplant.org/live-donorlaparoscopictransplant.html
Kidney Transplant Procedure Surgical removal of donor kidney (living donor). Locate and prepare kidney for removal. Prepare donor kidney for serotype analysis (to minimize threat of rejection). Flushing donor kidney with ice cold saline prior to serotyping www.viscom.ohiou.edu/kring/home.html
Kidney Transplant Procedure Surgical removal of donor kidney (living donor). Locate and prepare kidney for removal. Prepare donor kidney for serotype analysis (to minimize threat of rejection). Flushing donor kidney with ice cold saline prior to serotyping www.viscom.ohiou.edu/kring/home.html
Kidney Transplant Procedure Surgical removal of donor kidney (living donor). Locate and prepare kidney for removal. Prepare donor kidney for serotype analysis (to minimize threat of rejection). Donor organs are kept on ice in order to minimize tissue degradation. www.viscom.ohiou.edu/kring/home.html
Kidney Transplant Procedure Prepare recipient for donor organ (once serotyping has indicated a match). www.viscom.ohiou.edu/kring/home.html Contrary to donor procedure, recipient is supine to expose the pelvis.
Kidney Transplant Procedure Prepare recipient for donor organ (once serotyping has indicated a match). Donor kidney is inserted deep into the pelvic region, and all vessels are reconnected. www.kidneytransplant.org/patientguide/insurgrey.html Note: recipient’s kidneys are NOT removed.
Nephrolithiasis (Kidney Stones) Kidney stones are hard pellets formed in the nephron as minerals crystallize in the tubule. Calcium oxalate stones ( 70-80%) Uric acid ( 7%) Magnesium ammonium phosphate ( 2%) Other (xanthine, cystine) ( 2%)
Nephrolithiasis (Kidney Stones) If permitted to nucleate large enough, stones can lodge in the lumen of nephron and lead to urinary blockade, infection, nephritic damage, and severe pain. 70-80% of the crystallized minerals from which stones can nucleate are actually passed out in urine without being noticed.
Stone Formation Stones are formed when urine is supersaturated with the salts that are normally found in urine. Volume reduction (low urinary volume) High salt concentration (defective re-absorption by the tubular cells, excessive salt concentration in serum leading to excess salt in the glomerular filtrate). Under supersaturated conditions, the salts will precipitate out and form crystals.
Stone Formation Stone nucleation upon crystal formation can result from: Decreased “protective” factors: Mg2+, citrate, pyrophosphate etc. Factors act to prevent crystal formation, or coat the crystal to prevent adherence to tubule wall. Altered urinary pH: pH < 5.5 can favor uric acid and cystine stone formation. pH > 6 can favor calcium phosphate and magnesium ammonium phosphate stone formation.
Calcium Oxalate Stones General treatment calls for: Increased fluid intake Increased calcium intake Decreased oxalate intake Spinach, strawberries, nuts, chocolate, tea, dark cola, wheat bran,
Uric Acid Stones Treatment by: Restricted protein diet (uric acid is derived from purine metabolism, and purine is found in protein from meat, beer, legumes, spinach, asparagus etc.). Increase fluid intake
Magnesium Ammonium Phosphate Stones (Struvite) Normally linked to urinary tract infection. Treatments: Antibiotic therapy (Lithostat to inhibit bacterial activity) Urinary tract irrigation with organic acid (Struvite stones are acid soluble) Recent evidence for “nanobacteria” as the major cause Nano because they are smaller than 0.2m (cannot be “sterile filtered”)
Cystine Stones Excessive cystine in urine (cystinurea) linked to genetic defect in the intestinal processing of cystine. Cystine is soluble in urine at low pH, therefore treatments are aimed at acidifying urine. Alkaline-Ash diet: Milk, Fat (Nuts), Vegetables (except corn and lentils), Fruit (except cranberries, prunes, plums), Sweets: Molasses
Polycystic Kidney Disease (PKD) Genetic disease resulting in gradual kidney degeneration due to cyst formation within the nephon Etiology is still being studied Linked to defective transporters along the nephron & absence of primary cilium among others
Renal Dialysis Should urinary system fail, renal dialysis is an option Either mechanical or through the use of patients own peritoneal cavity
Renal Dialysis Chronic ambulatory peritoneal dialysis (CAPD) uses the patients peritoneal membrane as the filtration medium Introduce dialysis fluid into the peritoneum, withdraw when it has “exchanged” and is full of metabolic waste (4-6 times daily)