

c62f93a01aeabd6778310e7e65995f63.ppt
- Количество слайдов: 19
 The State of the Excimer Laser for Coronary Intervention in the Drug Eluting Stent Era Salem Badr, Itsik Ben-Dor, Hironori Kitabata, Sa’ar Minha, Joshua P. Loh, Lakshmana K. Pendyala, Israel M. Barbash, Danny Dvir, Rebecca Torguson, Kenneth M. Kent, Lowell F. Satler, William O. Suddath, Augusto D. Pichard, and Ron Waksman. Medstar Washington Hospital Center, Washington DC
The State of the Excimer Laser for Coronary Intervention in the Drug Eluting Stent Era Salem Badr, Itsik Ben-Dor, Hironori Kitabata, Sa’ar Minha, Joshua P. Loh, Lakshmana K. Pendyala, Israel M. Barbash, Danny Dvir, Rebecca Torguson, Kenneth M. Kent, Lowell F. Satler, William O. Suddath, Augusto D. Pichard, and Ron Waksman. Medstar Washington Hospital Center, Washington DC
 Salem Badr, MD I/we have no real or apparent conflicts of interest to report.
Salem Badr, MD I/we have no real or apparent conflicts of interest to report.
 Background • Laser was introduced two decades ago for the treatment of complex coronary interventions. • Approved by FDA for coronary use for the following indications: 1. Dubulking of SVG 6. Total occlusions crossable by guide wire 2. Ostial lesion 7. Moderately calcified lesion 3. Eccentric lesions 8. Balloon refractory lesions 4. Long lesions 20 mm 9. In stent restenosis 5. Acute myocardial infarction.
Background • Laser was introduced two decades ago for the treatment of complex coronary interventions. • Approved by FDA for coronary use for the following indications: 1. Dubulking of SVG 6. Total occlusions crossable by guide wire 2. Ostial lesion 7. Moderately calcified lesion 3. Eccentric lesions 8. Balloon refractory lesions 4. Long lesions 20 mm 9. In stent restenosis 5. Acute myocardial infarction.
 § Since its introduction, several modifications in Laser technology have been made to further improve procedure outcomes and safety. § A xenon-chlorine (excimer) pulsed laser catheter (X 80; Spectranetics, Colorado Springs, CO)capable of delivering higher energy density with lower heat production (smaller area of ablation) § Technique of saline infusion for blood and dye clearance should prevent acoustomechanical trauma to the vessel wall which leads to decrease the rate of coronary dissection.
§ Since its introduction, several modifications in Laser technology have been made to further improve procedure outcomes and safety. § A xenon-chlorine (excimer) pulsed laser catheter (X 80; Spectranetics, Colorado Springs, CO)capable of delivering higher energy density with lower heat production (smaller area of ablation) § Technique of saline infusion for blood and dye clearance should prevent acoustomechanical trauma to the vessel wall which leads to decrease the rate of coronary dissection.
 Objective • We sought to evaluate the indications, complications and clinical outcome in patients undergoing percutaneous coronary intervention (PCI) with laser in DES era.
Objective • We sought to evaluate the indications, complications and clinical outcome in patients undergoing percutaneous coronary intervention (PCI) with laser in DES era.
 with") Methodology • The study includes all patients who underwent percutaneous coronary intervention (PCI) with laser in our institution from 2004 to 2011. • The analysis was conducted in accordance with our local Institutional Review Board regulations. • Laser catheter size and pharmacological therapy decisions were made by the operator.
Methodology • The study includes all patients who underwent percutaneous coronary intervention (PCI) with laser in our institution from 2004 to 2011. • The analysis was conducted in accordance with our local Institutional Review Board regulations. • Laser catheter size and pharmacological therapy decisions were made by the operator.
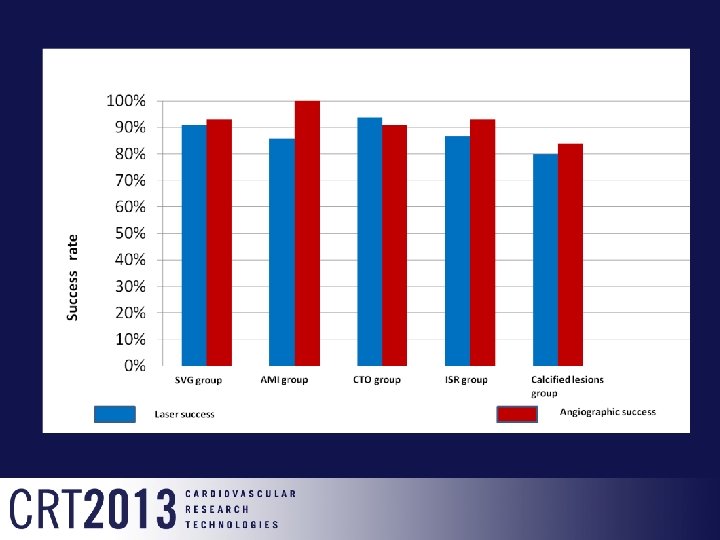
 Endpoints • Indications for laser use • Outcomes of the procedures: Laser success (defined as the laser catheter crossing the entire length of the stenotic lesion) Angiographic success (defined as <50% residual stenosis after laser and adjunctive therapy)
Endpoints • Indications for laser use • Outcomes of the procedures: Laser success (defined as the laser catheter crossing the entire length of the stenotic lesion) Angiographic success (defined as <50% residual stenosis after laser and adjunctive therapy)
 SVG n = 45 lesions Calcified group") 119 patients with 124 lesions (2004 -2011) SVG n = 45 lesions Calcified group n = 25 lesions CTO n = 32 lesions Acute MI n = 7 lesions Instent restenosis n = 15 lesions
119 patients with 124 lesions (2004 -2011) SVG n = 45 lesions Calcified group n = 25 lesions CTO n = 32 lesions Acute MI n = 7 lesions Instent restenosis n = 15 lesions
 Acute myocardial infarction N =") Results. Baseline characteristics Saphenous vein graft N = (45) Acute myocardial infarction N = (7) Chronic total occlusion N = (32) In-stent restenosis N = (15) Calcified lesion N = (25) Age 72. 3± 10. 2 65. 6± 15. 6 62. 0± 11. 6 62. 5± 10 70. 2± 13. 7 Men 31 (77. 5%) 6 (85. 7%) 23 (71. 9%) 10 (66. 7%) 15 (60%) Hypertension 39 (97. 5%) 4. 0 (66. 7%) 29 (90. 6%) 14 (93. 3%) 22 (88%) Diabetes 21 (53. 8%) 2. 0 (33. 3%) 15 (46. 9%) 9. 0 (60%) 9. 0 (36%) 38 (95%) 6. 0 (100%) 31 (96. 9%) 15 (100%) 24 (96%) PVD 17 (43. 6%) 0 9. 0 (28. 1%) 4. 0 (30. 8%) 2. 0 (8. 0%) Renal failure 2. 0 (5. 0%) 0 2. 0 (6. 3%) 1. 0 (6. 7%) 3. 0 (12%) Prior PCI 17 (47. 2%) 3. 0 (42. 9%) 9. 0 (31%) 11 (100%) 11 (47. 8%) Prior CABG 40 (100%) 2. 0 (28. 6%) 5. 0 (15. 6%) 6. 0 (40%) 7 (29. 2%) 43± 15% 42± 8. 0% 45± 17% 42± 15% 53± 11% Hyperlipidemia Ejection fraction
Results. Baseline characteristics Saphenous vein graft N = (45) Acute myocardial infarction N = (7) Chronic total occlusion N = (32) In-stent restenosis N = (15) Calcified lesion N = (25) Age 72. 3± 10. 2 65. 6± 15. 6 62. 0± 11. 6 62. 5± 10 70. 2± 13. 7 Men 31 (77. 5%) 6 (85. 7%) 23 (71. 9%) 10 (66. 7%) 15 (60%) Hypertension 39 (97. 5%) 4. 0 (66. 7%) 29 (90. 6%) 14 (93. 3%) 22 (88%) Diabetes 21 (53. 8%) 2. 0 (33. 3%) 15 (46. 9%) 9. 0 (60%) 9. 0 (36%) 38 (95%) 6. 0 (100%) 31 (96. 9%) 15 (100%) 24 (96%) PVD 17 (43. 6%) 0 9. 0 (28. 1%) 4. 0 (30. 8%) 2. 0 (8. 0%) Renal failure 2. 0 (5. 0%) 0 2. 0 (6. 3%) 1. 0 (6. 7%) 3. 0 (12%) Prior PCI 17 (47. 2%) 3. 0 (42. 9%) 9. 0 (31%) 11 (100%) 11 (47. 8%) Prior CABG 40 (100%) 2. 0 (28. 6%) 5. 0 (15. 6%) 6. 0 (40%) 7 (29. 2%) 43± 15% 42± 8. 0% 45± 17% 42± 15% 53± 11% Hyperlipidemia Ejection fraction
 Acute myocardial infarction N =") Results. Procedural data Saphenous vein graft N = (45) Acute myocardial infarction N = (7) Chronic total occlusion N = (32) In-stent restenosis N = (15) Calcified lesion N = (25) 88. 7± 43 105. 6± 60. 5 106. 2± 36. 4 73. 5± 24. 3 95. 4± 29 Left main 0 0 1. 0 (4. 0%) LAD 0 2. 0 (28. 6%) 5. 0 (15. 6%) 4. 0 (26. 7%) 5. 0 (20%) LCX 0 0 6. 0 (18. 8%) 6. 0 (40%) 4. 0 (16%) 0 3. 0 (42. 9%) 21 (65. 6%) 5. 0 (33. 3%) 15 (60%) 45 (100%) 2. 0 (28. 6%) 0 0. 9 mm 20 (44. 4%) 2. 0 (28. 6%) 27 (84. 4%) 5. 0 (33. 3%) 23 (92%) 1. 4 mm 14 (31. 1%) 2. 0 (28. 6%) 4. 0 (12. 5%) 4. 0 (26. 7%) 1. 0 (4%) 1. 7 mm 3. 0 (6. 7%) 1. 0 (14. 3%) 0 1. 0 (6. 7%) 0 2. 0 mm 4. 0 (8. 9%) 0 0 3. 0 (20%) 0 0 0 1. 0 (3. 1%) 0 0 Rota after 2. 0 (15%) 0 1. 0 (3. 1%) 1. 0(6. 7%) 6. 0 (24%) Brachytherapy 1. 0 (2. 2%) 0 1. 0 (3. 1%) 1. 0 (6. 7%) 0 Aspiration 3. 0 (6. 7%) 3. 0 (42. 9%) 1. 0 (3. 1%) 0 0 Cutting balloon 1. 0 (2. 2%) 1. 0 (14. 3%) 0 0 0 4. 0 (12. 5%) Procedural length (min) RCA SVG Laser Concomitant use of Rota before Tornus 0 0
Results. Procedural data Saphenous vein graft N = (45) Acute myocardial infarction N = (7) Chronic total occlusion N = (32) In-stent restenosis N = (15) Calcified lesion N = (25) 88. 7± 43 105. 6± 60. 5 106. 2± 36. 4 73. 5± 24. 3 95. 4± 29 Left main 0 0 1. 0 (4. 0%) LAD 0 2. 0 (28. 6%) 5. 0 (15. 6%) 4. 0 (26. 7%) 5. 0 (20%) LCX 0 0 6. 0 (18. 8%) 6. 0 (40%) 4. 0 (16%) 0 3. 0 (42. 9%) 21 (65. 6%) 5. 0 (33. 3%) 15 (60%) 45 (100%) 2. 0 (28. 6%) 0 0. 9 mm 20 (44. 4%) 2. 0 (28. 6%) 27 (84. 4%) 5. 0 (33. 3%) 23 (92%) 1. 4 mm 14 (31. 1%) 2. 0 (28. 6%) 4. 0 (12. 5%) 4. 0 (26. 7%) 1. 0 (4%) 1. 7 mm 3. 0 (6. 7%) 1. 0 (14. 3%) 0 1. 0 (6. 7%) 0 2. 0 mm 4. 0 (8. 9%) 0 0 3. 0 (20%) 0 0 0 1. 0 (3. 1%) 0 0 Rota after 2. 0 (15%) 0 1. 0 (3. 1%) 1. 0(6. 7%) 6. 0 (24%) Brachytherapy 1. 0 (2. 2%) 0 1. 0 (3. 1%) 1. 0 (6. 7%) 0 Aspiration 3. 0 (6. 7%) 3. 0 (42. 9%) 1. 0 (3. 1%) 0 0 Cutting balloon 1. 0 (2. 2%) 1. 0 (14. 3%) 0 0 0 4. 0 (12. 5%) Procedural length (min) RCA SVG Laser Concomitant use of Rota before Tornus 0 0
 Acute myocardial infarction N =") Results. In-hospital outcomes Saphenous vein graft N = (45) Acute myocardial infarction N = (7) Chronic total occlusion N = (32) In-stent restenosis N = (15) Calcified lesion N = (25) Dissection 0 0 3 (9. 4%) 1 (6. 7%) 0 Perforation 0 0 1 (3. 1%) 0 1 (4. 0%) No-reflow 0 0 0 1 (6. 7%) 2 (8. 0%) Thrombus 0 0 1 (3. 1%) 0 0 0 0 formation Death
Results. In-hospital outcomes Saphenous vein graft N = (45) Acute myocardial infarction N = (7) Chronic total occlusion N = (32) In-stent restenosis N = (15) Calcified lesion N = (25) Dissection 0 0 3 (9. 4%) 1 (6. 7%) 0 Perforation 0 0 1 (3. 1%) 0 1 (4. 0%) No-reflow 0 0 0 1 (6. 7%) 2 (8. 0%) Thrombus 0 0 1 (3. 1%) 0 0 0 0 formation Death
 Summary • Laser is a very useful tool in complex coronary intervention including calcified, CTO, SVG, AMI and instent restenosis. • Laser is safe and effective for balloon refractory lesions • The most common laser catheter used is 0. 9 mm. • Laser can also be used as an adjunct to facilitate rotational atherectomy.
Summary • Laser is a very useful tool in complex coronary intervention including calcified, CTO, SVG, AMI and instent restenosis. • Laser is safe and effective for balloon refractory lesions • The most common laser catheter used is 0. 9 mm. • Laser can also be used as an adjunct to facilitate rotational atherectomy.
 CASE - Saphenous vein graft Clinical History • 71 -year-old female • History of hypertension, hyperlipidemia, diabetes mellitus, and CABG in 2005 • Admitted after developing hypotension and chest pain during nuclear stress testing. The scintigraphy revealed ischemia involving the inferior and lateral walls.
CASE - Saphenous vein graft Clinical History • 71 -year-old female • History of hypertension, hyperlipidemia, diabetes mellitus, and CABG in 2005 • Admitted after developing hypotension and chest pain during nuclear stress testing. The scintigraphy revealed ischemia involving the inferior and lateral walls.
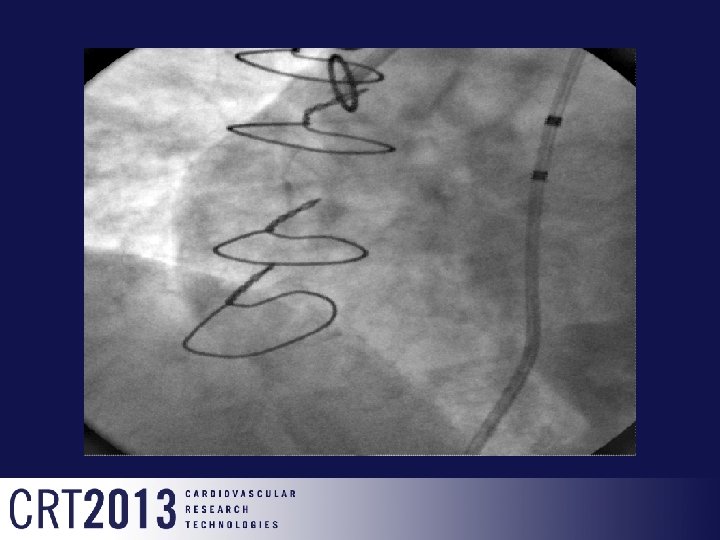
 0. 9 mm Laser
0. 9 mm Laser
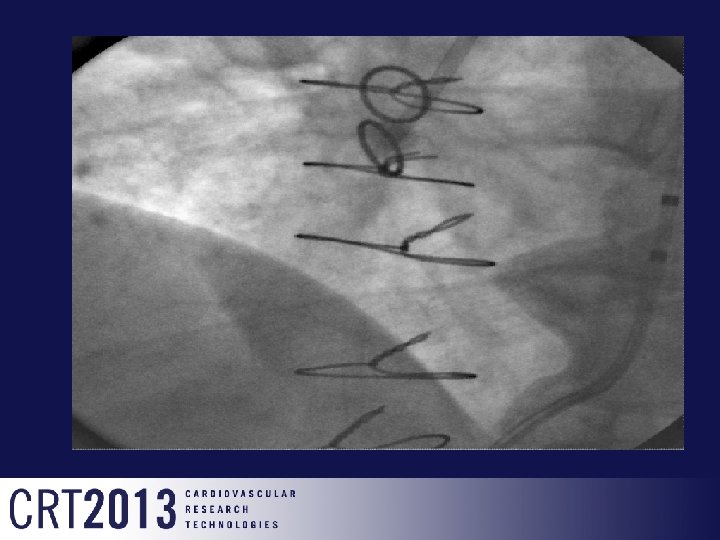
") distal protection device (Spider FX 5. 0 -mm)
distal protection device (Spider FX 5. 0 -mm)
 Thank you
Thank you