6f090726c09974b279ec00177b478906.ppt
- Количество слайдов: 57



The Role of Interoperability Standards for Emerging Countries Beatriz de Faria Leão, MD, Ph. D Health Standards Architect Zilics Health Information Systems, São Paulo, Brazil HL 7 Brazil - Co-Chair Advisory Council

Agenda • Overview and Health Challenges • Standards and National e. Health Policies in – – Uruguay Argentina Chile Brazil • The role of HL 7 in South America

Thanks to all that contributed for this presentation: • Alvaro Margolis - President IMIA - LAC • Ana Estela Haddad - Director of Management of Education in Health - Ministry of Health Brazil • Claudio Giulliano da Costa - CIO São Paulo Dept of Health, Brazil • Diego Kaminker - Chair HL 7 Argentina • Fernán González B. de Quirós - Hospital Italiano, Buenos Aires, Argentina • Julio Carrau - Chair HL 7 Uruguay • Jussara Macedo - Brazilian Supplementary Health Agency • Lincoln A. Moura Jr – IMIA Board - Treasurer • Marivan Santiago Abrahão - Chair HL 7 Brazil • Sergio A. König - Director IT&GS Consultores Ltda.

SOUTH AMERICA • • • 4 th continent in size Area 17, 840, 000 km² Population 371 millions Countries 12 Languages: Spanish, Portuguese, French, Dutch, English …. • GDP $3. 33 Trillion

http: //www. globalhealthfacts. org/topic. jsp? i=46

Facts: In spite of the huge difference in the health expenditure between South American countries and US …

Health indicators are not that different… Some health figures in Brazil • Prenatal coverage increased from 23% to 70% (including 6 doctor visits) over the last 15 years. • 90% vaccine coverage • Free access to antiretroviral treatment and to high complexity care. AIDS quick tests are available for 1/3 of deliveries and free ARV is guaranteed • Second country in the world in organ transplantations, first in publicly-funded transplants.

Uruguay National ehealth Policy • 3. 46 million people • 1. 7 million live in the capital Montevideo and its metropolitan area

Uruguay e. Health Policy • Sept 30 th, 2003 - Federal Government issued the bill nº 396/003, on the EHR for all citizens, suggesting the use of international standards, such as HL 7 and DICOM • March 2006, the elected Government, presents to the parliament the project of the NATIONAL INTEGRATED HEALTH SYSTEM (SISTEMA NACIONAL INTEGRADO DE SALUD) where sharing of information among all HC providers is mandatory, from 2007 on.

SUEIIDISS Sociedad Uruguaya de Estandarización, Intercambio e Integración de Datos e Información de Servicios de Salud • Founded in Nov 2005 • HL 7 affiliate (country 26) • 46 Members • Mission: to promote, develop, and provide training and capacity building on interoperability standards to share health information for patient care and health care management with all HC actors • Focus on HL 7 v 3 y CDA and IHE

www. sueiidiss. org

Uruguay / SUEIIDIS Interoperability Standards in use • IHE profiles: – Security digital certificates based on national PKI infrastructure • • • Consistent Time service provided by SUEIIDIS CDA (HL 7 v 3) for documents sharing Uruguay National Identification standards OIDs for objects identifications Common WSDL defined and shared among all participants
 • GDP (nominal)")
e. Health Standards in Argentina • 40 million people (estimate 2008) • GDP (nominal) 2007 estimate – Total $260. 7 billion – Per capita $6, 548

HL 7 Argentina www. hl 7 argentina. org • Founded on December 5 th, 2001 • 28 members (9 of them individuals) • HL 7 is not a national Standard for Argentina, but there are several developments involving the use of HL 7 standards for e-claims and interdepartmental interoperability (mainly using HL 7 V 2. x and CDA R 2) • Focus on training and dissemination of the HL 7 standards - > virtual learning platform – 600 people trained since 2001, from different countries in LA for the Spanish version – 200 international students for the English version

http: //campus. hl 7. org. ar/
 • GDP")
e. Health in Chile • Population 16, 598, 074 (June 2007 estimate) • GDP (nominal) 2007 estimate – Total $163. 792 billion – Per capita $9, 879

http: //www. hl 7 chile. cl/

Brazil: “Soft Power”- Emerging Giant

Brazil – Geo-political Perspective • The largest country in Latin America • The only Portuguesespeaking country in LA (52% of South America speak Portuguese) • The 5 th most populated country in the World • The 3 rd country in number of Internet hosts in America • GDP (nominal) 2008 estimate – Total US$ 673 billion – Per capita US$ 3, 640. 88

SUS – The Brazilian Health System • Universal Access – Health is a Right of All (~ 150 M individuals) • Full Coverage, Free of Charge – All Services and Procedures • SUS principles: – Equity – Universality – Integrality • Funding and Management are Shared – Federal, State and Municipal Levels • Supplementary Health for Those Wiling to Pay – ~ 1, 600 HMOs (~ 49 M individuals) – ANS (Agência Nacional de Saúde Suplementar) Regulates the Sector

et The Brazilian Healthcare Market ark d M s! • Extremely Fragmented Market: ~ U$ 90 B/year ate n er iin volume and some 50% in $ – SUS is the major Payer: ~ 66% rd lay oo 5. 500 cities d. P c – 190 M inhabitants, spread over e Un andnect. Health Plan Operators – Around 6, 000 Hospitals nd n 1, 600 (HMOs) a ed Hospitalsy Co than 80 beds – nt of e 70% Badl have less gm – Estimate that only 10% of Hospitals havei. Information Systems t n a d Fr en an – l 90% HMOs cover less than 50, 000 lives each m l a– Only 3% of HMOs coverestithan 200, 000 IT Sm nv morethatt 4 M nd each – The largest HMO covers less n a lives e. I ttl iimportant network of Health Organizations me – There is L no ge chain, added value and best – Lack of notion ana of production practices M – National Standards on their way – It’s a “Market of Discontent”

Healthcare Challenges in Brazil • Increasing demand for health care (aging, emerging of new diseases, re-emerging of considered overcome diseases) • Skyrocketing healthcare costs (Health Technology) • Inefficiency, paper base uncoordinated system, multiple formularies, poor resource allocation • Siloed systems - one for each health program • Lack of adequate information to support decision making, quality of care evaluation and to monitor disease management programs; • Few common health and healthcare information standards within the sector
 – HC")
Brazilian HC National Standards • Unique HC Identifiers – Individual (160 Million) – HC providers (180 Thousand) – Health Workers (1. 4 Million) • Content and Vocabularies – – – Essential Encounter Dataset Diagnostics (ICD-10), Procedures Immunization Charts Birth and Death National Registries (> 50 years) Notifiable Diseases ( Work related, external causes and communicable diseases) – Hospital Discharge Summaries – High Complexity Utilization Reports
")
Brazilian HC National Standards: National Unique Identifiers: • Individuals (160 million people uniquely identified) • Healthcare providers (181. 903 uniquely identified) – Includes information on: – Medical specialties, number of beds, equipments, private and public distribution, complexity level, – Health professionals (physicians, nurses and administrative personnel) – 1. 5 million healthcare professionals uniquely identified

Brazilian HC National Standards • Interoperability: – TISS – Private Health Information Exchange – Lab Integration (LOINC + HL 7 Brazil) • Security – National PKI infrastructure • Software Certification – Brazilian Health Informatics Society + Federal Medical Council (www. sbis. org. br/certificacao)

Tele. Health National Project • Promote the use of technology by the Family Health teams • Decrease the number of patients sent to secondary level • Evaluate different technologies, methodologies and costs • Improve quality of primary care • Leads to money-saving (preliminary figures are 100: 1) Source: Ana Estela Haddad, Bellagio, August, 2008

Tele. Health National Project Coverage: Nine State Clusters implementing Telehealth in 900 health units supporting about 2, 700 Health Family teams, covering 11, 000 inhabitants.



Private Healthcare Insurance Market 1. 600 active Health Plan Organizations 600. 000 estimated Healthcare providers 49. 3 million beneficiaries Selfregulation HPOS ANS State Regulation Sources; www. hl 7 brazil. org Set 2008

TISS - the Brazilian standard for HPOs and HC providers communication NSHA DATABASE (enroll/disenrollments , services utilization, health care indicators) HMOS NHS TISS - XML Demographics, Vital Statistics, Discharge Summary, Notifiable Diseases Healthcare providers Source: Jussara Macedo, ANS, 2007

TISS - Standards • Information structure: billing forms – – Consultation Hospital Discharge Lab, Medical Images Authorization for High Cost and High Complexity Procedures • Core Health Terminologies and Code Sets (e. g ICD-10) • Messaging: XML schemas and Web services • Privacy: ISO/NBR 17799 and SBIS/CFM Software Certification • Mandatory from May 2007 on Source: Jussara Macedo, ANS, 2007

TISS Transactions PROVIDERS Eligibility and prior Authorization Claim Generation Service Billing Claim Status Inquiries Accounts Receivable HPOS Health care Services Delivery Pre certification and Adjudication Claims Acceptation Patient Info Claim Status Inquiry Claim Status Response Claim Payment Adjudication Accounts Payable Source: Jussara Macedo, ANS, 2007

www. hl 7 brazil. org

HL 7 Brazil Actions • Harmonize National Standards with HL 7 • Training Programs • Working Groups – CDA, LOINC, Snomed, Support • Affiliationship – Individual - 10 – Corporate - 15 • INTERSYSYEM, ZILICS, MICROSOFT, INTEL, ANS, SERASA

HL 7 BRAZIL ACTIVITIES • FEB/2007 - creation of Institute HL 7 Brazil • COURSES – Oct/ 2007 - I BASIC COURSE OF HL 7 - with John Ritter - 70 persons - São Paulo – Abr /2008 - HL 7 - VERSION 3. 0 - with Mead Walker - 40 persons, São Paulo • MEETINGS – Oct/2007 - OPEN FORUM HL 7 INTEL - with William Edward Hammond - São Paulo – 1 er Congreso Iberoamericano de Informática Médica Normalizada, Montevideo, Uruguay – April /2008 - OPEN FORUM HL 7 - IT-MÍDIA - with Mead Walker- São Paulo

Case Studies • In. Cor – São Paulo Heart Institute – Continuous Glucose Monitoring System on a Intensive Care Unit HL 7 V 2. X • Fleury Laboratory – Microbiological Exams Management System • São Paulo City Health Department – SIGA Saúde LAB Integration

SIGA Saúde São Paulo City’s Health Information System Lab Integration Claudio Giulliano da Costa, MD CIO São Paulo Health Department

São Paulo is the largest city in South America, with 12 M inhabitants and some 22 M in the Metropolitan Area. Initial Figures: 400 Primary Care Units 60 Polyclinics 160 Hospitals 11 M Users 8. 5 M Emergency T/year 550 k Inpatients/year 11 M Primary Care C/year

SIGA SAÚDE • SIGA Saúde is São Paulo City’s Integrated and Distributed System for Managing the Public Healthcare System • The system belongs to São Paulo City, which is willing to share it withpresentcities, states and other in 100% of SIGA Saúde is countries São Paulo City public health care providers • SIGA Saúde has been developed using freesoftware open-code concepts.
 Dept of Health Internet")
SIGA Saúde IT Model Management SMS-SP (Surveillance, Auditing and Billing) Dept of Health Internet Patient Flow Organization & Mngmnt (Specialties, Beds, Exams) Electronic Health Record SP City Datacenter Access Control

SIGA Saúde Figures for May, 2008 • • 14, 301, 383 registered users 1, 017, 463 primary care scheduling / month 189, 393 specialized care consultations / month 1, 738, 807 medical prescriptions attended over the counter / month • 35, 000 authorizations of high cost & complexity procedures / month • 30% reduction in the waiting time for specialized consultations & procedures • Medication available at local pharmacies - supply chain control

SIGA Saúde Lab Integration • 2. 7 millions exams / month – About 300 different labs exams without previous authorization – Others need prior authorization • Manual process: transcribe errors, duplication of exams, bad resource allocation • Ordering HC providers – 403 Primary care Units – 100 Emergency and Specialized Units – 15 Hospitals • Executing Labs – Private Labs (3) + Public Labs (6)

SIGA Saúde Lab Integration Lab Orders LAB 1 LAB 2 LAB N LAB 3 XML SIGA Web Service: LAB XML Sample Collection Lab Order Authorization UBS AE AMAS Hospital Emergency

SIGA Saúde Lab Integration Lab Results LAB 1 LAB 2 LAB 3 LAB N XML SIGA Web Service: SIGA XML Lab Results (Common, Micro, Pathology) - CDA in Phase 1 UBS AE AMAS Hospital Emergency

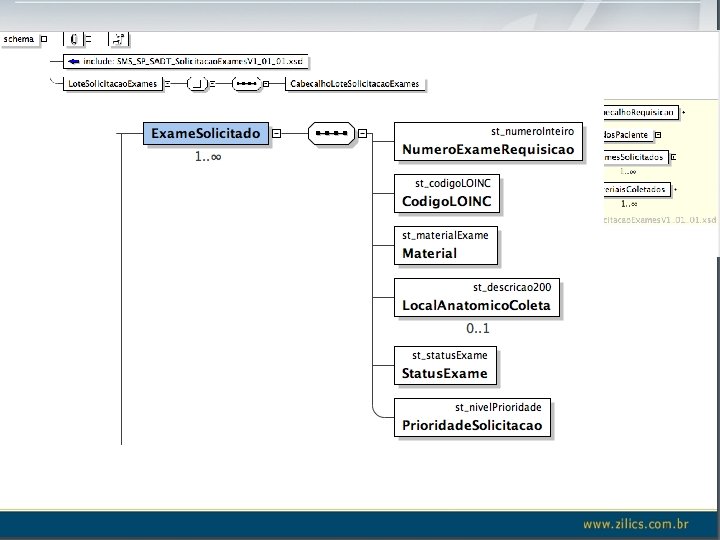
Standards used for SIGA’s Lab Integration • Identification: – Patient’s - National Health Card Number – HC provider and HC provider - National Registry CNES • Messages: – TISS: XML schemas (simple. Types, complex. Types, Messages, WSDL) – HL 7 v 3 - Lab orders and results information content (tags translated) – HL 7 v 3 pan-Canadian Messaging Standards • Vocabulary: – LOINC - Logical Observation Identifiers Names and Codes

HL 7 v 3 for LAB • Why V 3? – Information content of lab orders and result is VERY GOOD, much better than V 2 • V 3 Messages are too big, why? – Events that belong to applications are part of the message • Our approach – Use the core information content from V 3 – Change the “envelope” and “roles” to a simpler schema – Leave the information about the events on the application (Web Service or not) – Make a clean message - take advantage of the unique identifiers

TISS envelope

SIGA Saude Lab Integration: Current Status • Order messages in test • Results messages: – Common Lab Results - structured + Observations in free text – Microbiology - structured + text – Pathology - mostly text based • Web service is under testing • Results: – Phase 1: with a CDA approach (PDF attachment) – Phase 2: results structured using LOINC (October 15 th on)

SIGA SADT Lab Integration Challenges • LOINC was almost unknown in the beginning of the project (jan 2007) • Language Barriers / HR • Labs: had to redefine all internal codes and preformatted sentences to LOINC codes • HL 7 was not used, some have heard of v 2, v 3 was too “scary” and tools were too complicated • Solution - > T R A I N G HL 7 and LOINC

SIGA Saude Lab Integration LOINC Translation and Mapping • LOINC mapping to the SUS Procedure Table • For each SUS code: – There could be one or more LOINC codes for orders – Example:

SIGA SADT Lab Integration What have we achieved so far? • First LOINC translation to PT is ready, thanks to one of the private Lab • Today LOINC is being considered as the national vocabulary for exams both for the private and public systems • Shift of mind: from payment to patient care • Team work: mapping of the 300 exams is ready • Advantages of having a standard are now clearly understood

HL 7 Role for developing countries • HL 7 is “THE” organization able to foster standards development in emerging and developing countries • It’s a place where PEOPLE come together to: – – – Learn about standards Develop standards To adapt what is already there To propose new standards To create, to innovate and above all, To foster the development of interoperable health information systems

HL 7 role for developing countries • Suggestions: – – Promote South to South collaboration Re-thinking of v 3 (v 4? ) Learn from international examples Promote full interoperability with ISO 13606 - data types alignment – Better tools on open source environments – Free Distribution of HL 7 standards according to country HDI

Above all, let’s keep HL 7 friendly, open environment, where people leave their “egos” outside the room and feel comfortable to think outside the box in order to improve health care everywhere A living example of that is:

Bellagio, July 2008, Interoperability Week Thank you very much for your attention!
6f090726c09974b279ec00177b478906.ppt