3ae48a055f4cbfa1ffe4af9dffc1e2f2.ppt
- Количество слайдов: 34



The returning traveller A few cases Richard Bellamy ID Physician

Case 1 • A 23 year-old African man presented with a 3 day history of intermittent fever. He was a student who had spent his summer holiday in Nigeria. He had returned one week previously. • What investigations would you perform?

• His malaria film showed a parasitaemia of 24%. • Which patients can be treated in the community ? • Where should patients requiring treatment in hospital be sent? (ID unit or general medicine) Spend 5 minutes discussing in pairs or small groups.

• Treatment of falciparum malaria usually requires hospital admission in the UK. Patients can deteriorate rapidly. • Non-falciparum malaria could be treated outside hospital. • Treatment of non-severe malaria is usually straightforward and could occur in any hospital. Options include quinine, doxycycline and atovaquone/proguanil. • Treatment of severe malaria is difficult and requires specialist input. However a GP is unlikely to be able to evaluate severity reliably.
 • • • Parasitaemia")
Features of severe malaria (you only need 1 of these) • • • Parasitaemia >2% (5% if endemic) Schizonts (not dual infection) Temp >39 o. C Non-ambulant Cerebral involvement Pulmonary oedema • • Hypovolaemia Creat >265 mmol/L Hb <8 g/dl or PCV <0. 20 Hypoglycaemia Bleeding/ DIC Bilirubin >50 Acidosis

Case 2 • A 46 year-old man presented with a 1 -day history of diarrhoea. He was a soldier who had returned from Sierra Leone. • What 2 questions do you want to ask him ? • How would you manage him? Spend 5 minutes discussing in pairs or small groups.

• • • Find out whether he has had contact with patients with Ebola. – Category 1: no contact – Category 2: contact with PPE – Category 3: contact without PPE or breach of PPE. Find out if he has been febrile or if he has a temperature now. If febrile and category 2/3 phone 999. If afebrile routine care is appropriate (unlikely VHF). If category 1 but febrile, VHF is possible depending on exact exposure history. Seek specialist advice before admission as could be high possibility or low possibility of Ebola.
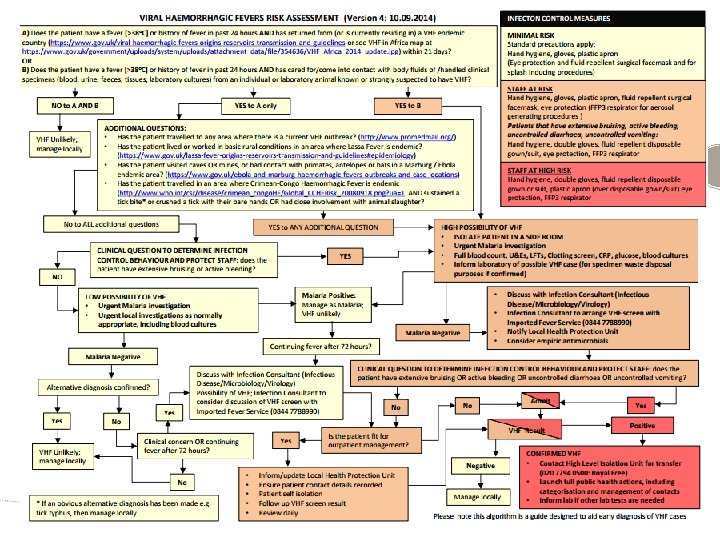

Viral haemorrhagic fevers • • • The most important diseases are endemic in West and Central Africa. – Marburg, Ebola, Lassa, Congo-Crimea HF A very difficult diagnosis for a GP outside of the current Ebola epidemic. Other VHFs don’t transmit person-to-person – Junin, Machupo, Guanarito, Sabia and Dengue

Current Ebola epidemic in 2014 • Outbreak in Guinea, Sierra Leone and Liberia • >20, 000 cases so far • Probably 10, 000 deaths • Largest outbreak ever

Viral haemorrhagic fevers; clinical manifestations • • • Incubation is around 2 -21 days. Prodrome: fever, headache, myalgia, sore throat, cough, vomiting. Haemorrhagic phase: petechiae, bruising, intestinal haemorrhage, bleeding from eyes, nose, mouth, gums, lungs, uterus plus encephalopathy and multi-organ failure.

Viral haemorrhagic fevers; transmission • • Contaminated blood and body fluids are source Transmission: – Contact with non-intact skin. – Mucus membrane contact. – Sexual contact. – Airborne transmission does not occur.

Case 3 • • • A 25 -year-old man presents with a 7 -day history of diarrhoea. He returned from a holiday in Turkey 3 days ago. What investigations would you perform? What would you do if the investigations were negative.

Investigations for travellers diarrhoea • • • Look at the stool (fluid? , blood? ) Stool for routine culture (Salmonella, Shigella, Campylobacter, Yersinia, E coli O 157 and Cryptosporidia) Stool for ova, cysts and parasites

Persistent symptoms beyond 4 weeks • • • Consider trial of metronidazole Check faecal calprotectin If positive refer for gastroenterology opinion

Case 4 • An 18 -year-old man presented with a 3 -day history of cough. He was a chinese student who had spent his summer holiday in Hong Kong. He had returned one week previously. Community-acquired pneumonia and avian influenza were considered. • What features are used to grade the severity of community acquired pneumonia ? • What do you know about avian influenza ? (mode of transmission , relevant contact history, timing of travel history, Xray findings, treatment) Spend 5 minutes discussing in pairs or small groups.

Pneumonia and avian influenza risk assessment • Determine if he meets the criteria for severe communityacquired pneumonia. Admit to hospital if he does. • Decide if he meets the criteria for avian influenza H 5 N 1 or H 7 N 9. You need to do this irrespective of whether or not hospital admission is needed.

Criteria for severe community-acquired pneumonia • • • Confusion Urea > 7 mmol/L Resp rate ≥ 30 per minute BP systolic <90 mm. Hg or diastolic ≤ 60 mm. Hg Age ≥ 65 years 2 or more points is severe

Avian influenza A H 5 N 1 • • For H 5 N 1: 393 deaths in 668 cases since 2003. Limited human-to-human transmission. 16 countries affected. Bad news for domestic poultry.

Millions of birds have died

Avian influenza A H 5 N 1 : current case definition • • Fever ≥ 38°C and Clinical or CXR findings of consolidation or ARDS and Travel to an affected country in 7 days before illness onset and Close contact with live, dying or dead domestic poultry (or human with severe unexplained respiratory illness).

Avian influenza A H 5 N 1: countries with human cases to date • • Azerbaijan Bangladesh Cambodia Canada China Djibouti Egypt Indonesia • • Iraq Lao PDR Myanmar Nigeria Pakistan Thailand Turkey Vietnam
 affected")
Avian influenza A H 7 N 9 • 175 deaths in 453 (39%) affected people Case definition: • Patient has visited China in the 10 days before onset of symptoms and • Fever ≥ 38°C and • Clinical or CXR findings of consolidation or ARDS

Avian influenza: what to do if you suspect it • • • Isolate patient at home or in hospital. Keep a contact list of all HCWs. Start oseltamivir. Notify PHE. Contact virology laboratory to discuss testing

Case 5 • A 54 -year-old man presented with a 3 -day history of cough. He had recently travelled throughout Saudi Arabia and had visited Mecca during the Hajj. He had returned one week previously. • • How would you assess him? What investigations would you perform? Spend 5 minutes discussing in pairs or small groups.

MERS coronavirus risk assessment • Determine if he meets the criteria for severe communityacquired pneumonia. Admit to hospital if he does. • Decide if he meets the criteria for MERS coronavirus infection. You need to do this irrespective of whether or not hospital admission is needed.

MERS-Co. V • • • First identified 24/09/2012 by Dr Zaki in Saudi Arabia Incubation period of 12 days Pneumonia and acute kidney disease Currently does not spread in a sustained person-toperson way, but could mutate Betacoronaviruses circulate in bats but origin of MERSCo. V is unproved 355 deaths in first 894 confirmed cases (40%)

MERS-Co. V: case definitions • Patient under investigation: – Any person with fever ≥ 38°C or history of fever and – Cough and – Clinical or radiological evidence of pneumonia and – Not explained by other cause and – Relevant travel history in 14 days before symptom onset or relevant contact history

MERS-Co. V: relevant travel • • Bahrain Iraq Israel Jordan Saudi Arabia Kuwait Lebanon • • • Occupied Palestinian territories Oman Qatar Syria UAE Yemen

Hajj could spread MERS-Co. V

MERS-coronavirus: what to do if you suspect it • • • Isolate patient at home or in hospital. Keep a contact list of all exposed persons. No treatment shown to be beneficial. Notify PHE. Contact virology laboratory to discuss testing

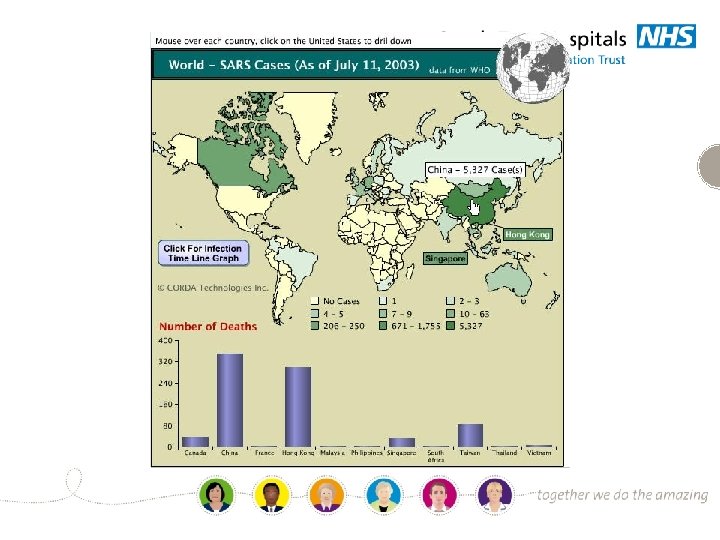
Why be concerned about recognition of these infections? • • • They are high priority in public health terms. You only get one chance to get it right or wrong. If the diagnosis is delayed hundreds of people can become exposed. Prompt identification can save many lives. Remember what happened with SARS.

Summary • Always ask for a travel history. • Remember to consider VHF/Ebola as well as malaria. • Look out for potential avian flu and MERS-Co. V • Prompt recognition could make a huge difference for outbreak control.
3ae48a055f4cbfa1ffe4af9dffc1e2f2.ppt