83523e6eead1a5e59a04c98bef6eb2d3.ppt
- Количество слайдов: 18



The relationship between gastrointestinal symptoms and ultrasound findings in women with suspected endometriosis Lee Cohen Mentor: Dr. Vered Eisenberg Arrow project June 2017

Endometriosis‐ Definition One of the most common benign gynecological conditions. Defined as the presence of endometrial‐like tissue outside the uterus, which induces a chronic inflammatory reaction.

Endometriosis‐ Prevalence The reported prevalence of endometriosis in literature is 1 of 10 women. An epidemiologic study from Israel, based on population enrolled in MHS between 1998‐ 2015, found that 1. 1% of women were diagnosed with endometriosis. These results correspond with other worldwide published database studies (UK, German, Italy) in low risk populations. Eisenberg, V. H. , Weil, C. , Chodick, G. , & Shalev, V. (2017). Epidemiology of endometriosis: a large population‐based database study in a 2‐million‐member health care provider. BJOG: An International Journal of Obstetrics & Gynaecology.

Symptoms Cyclic pelvic pain, chronic pelvic pain Dysmenorrhea Dyspareunia Dysuria Dyschezia Lower back or abdominal discomfort Subfertility Symptoms often worsening over time

Diagnosis Can be difficult because the presentation is variable and there is considerable overlap with other conditions, such as irritable bowel syndrome and pelvic inflammatory disease. Delay of several years between symptom onset and definitive diagnosis (10 years). A confirmed diagnosis of endometriosis is generally made at surgery.

Diagnosis‐ What’s the delay? A study that was done to investigate the reasons for the delay found two main reasons: 1. Delaying the diagnosis at an individual patient level: Difficulty to distinguish between normal and “abnormal” pain, embarrassment and comparison of their condition to a close person (“my mother suffered too”). 2. Delaying the diagnosis at a medical level: Pain normalized by family doctors and suppression of pain by hormones (OCT). Ballard, K. , Lowton, K. , & Wright, J. (2006). What’s the delay? A qualitative study of women’s experiences of reaching a diagnosis of endometriosis. Fertility and sterility, 86(5), 1296‐ 1301.
 (abdominal pain, bloating,")
Hypothesis and aims Women with endometriosis often have gastrointestinal complaints (GIC) (abdominal pain, bloating, constipation, diarrhea). Many women come to our clinic following a full gastrointestinal investigation (e. g. blood tests, gastroscopy, colonoscopy) which is normal. Taking notice of GI symptoms may reduce the delay in diagnosis in these patients. The aim of our study was to evaluate the relationship between GIC and findings on transvaginal ultrasound (TVUS).

Methods A prospective observational study. Women completed a self‐reported clinical data survey, gastrointestinal symptom questionnaire (Rome 3 and PFDI 20) and underwent 2 D/3 D TVUS. Endometriosis was diagnosed based on the presence of ovarian endometriomas, endometriotic nodules, signs of pelvic adhesions, or tubal disease. A symptom score was calculated based on reported gastrointestinal symptoms and pelvic pain symptoms. Statistical analysis ‐ SPSS
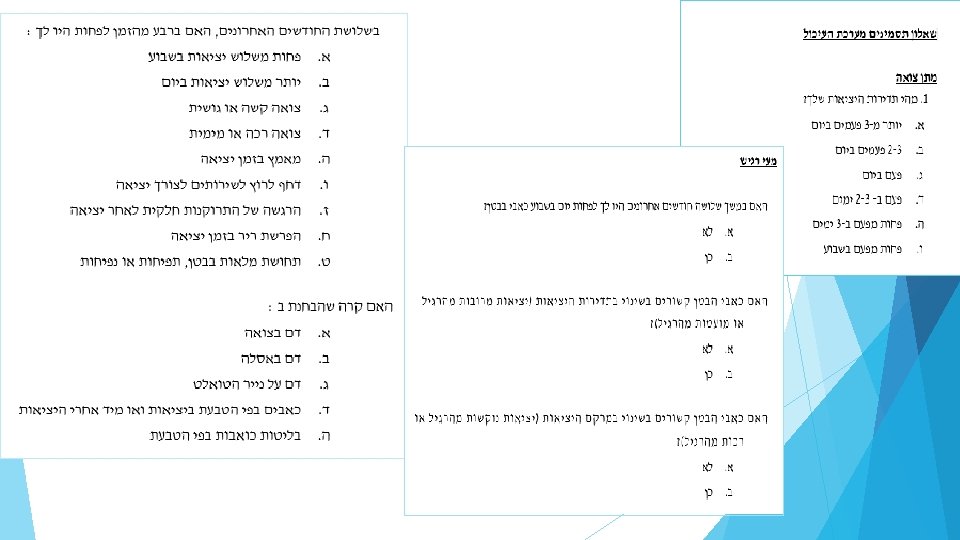

Methods A prospective observational study. Women completed a self‐reported clinical data survey, gastrointestinal symptom questionnaire (Rome 3 and PFDI 20) and underwent 2 D/3 D TVUS. Endometriosis was diagnosed based on the presence of ovarian endometriomas, endometriotic nodules, signs of pelvic adhesions, or tubal disease. A symptom score was calculated based on reported gastrointestinal symptoms and pelvic pain symptoms. Statistical analysis ‐ SPSS

Results ‐ demographics 192 women Age 33. 2± 7. 5 years BMI 23. 3± 4. 6 kg/m² Nulliparous 56. 8%

Results ‐ symptoms Dysmenorrhea 89% Chronic pelvic pain 77. 5% Dyspareunia 75. 4% Dyschezia 65. 4% Hematochezia 15. 7% Analgesic use 70. 7%
, left (22. 9%) Adhesions: right (42. 7%), left")
TVUS findings Endometrioma: right (14. 6%), left (22. 9%) Adhesions: right (42. 7%), left (43. 7%) Kissing ovaries (4. 2%) Uterosacral ligaments (27. 1%) Retro‐cervical nodules (12%) Recto‐sigmoid nodules (10. 9%) Pouch of Douglas obliteration (17. 2%) Bladder nodule (1%)

Correlations‐ GIC and TVUS Dyschezia‐ Uterosacral ligament involvement, Recto‐ Sigmoid nodule and Pouch of Douglas obliteration. Abdominal pain (which related stool frequency)‐ Pouch of Douglas obliteration. Feeling of rectal bulge‐ Recto‐sigmoid nodule and Deep intestinal nodules. Constipation‐ Deep intestinal nodules.

Conclusion We observed a high prevalence of GIC in women referred to a dedicated ultrasound at an endometriosis center. GIC were associated with findings on TVUS. The presence of GIC should prompt an earlier consideration, evaluation, and tertiary referral to an endometriosis center, which may potentially reduce the delay in diagnosis in these patients.

Strengths and limitations Strengths Prospective observational study Validated questionnaires Several TVUS investigators Limitations Single center study Short follow up

Future…. . Women who suffer from GIC will be referred earlier for evaluation for endometriosis. Gynecologists, gastroenterologists and general practitioners and pediatricians will be more aware of the connection between GIC and endometriosis and this way, help to reduce the delay in diagnosis.

Thank You for Listening!
83523e6eead1a5e59a04c98bef6eb2d3.ppt