

a462665df32dfd643231de261e638b57.ppt
- Количество слайдов: 36
 The Protocol At the time of discharge, death, or month’s end, each patient was reviewed and consensus reached on: ¶ The primary diagnosis: l the disease, syndrome or condition most responsible for the patient’s admission to hospital Centre for Evidence-Based Medicine
The Protocol At the time of discharge, death, or month’s end, each patient was reviewed and consensus reached on: ¶ The primary diagnosis: l the disease, syndrome or condition most responsible for the patient’s admission to hospital Centre for Evidence-Based Medicine
 · The Primary Intervention l l the treatment or other") The Protocol (cont. ) · The Primary Intervention l l the treatment or other manoeuvre that constituted our most important attempt to cure, alleviate, or care for the primary diagnosis traced into the literature to determine its basis in evidence – the Consultant’s “Instant Resource Book” – bibliographic data base searches Centre for Evidence-Based Medicine
The Protocol (cont. ) · The Primary Intervention l l the treatment or other manoeuvre that constituted our most important attempt to cure, alleviate, or care for the primary diagnosis traced into the literature to determine its basis in evidence – the Consultant’s “Instant Resource Book” – bibliographic data base searches Centre for Evidence-Based Medicine
 Primary Interventions were Classified by Level: ¶ Evidence from Randomised Control Trials (better yet: systematic reviews of all relevant, high-quality RCTs) · Convincing non-experimental evidence (unnecessary & unethical to randomise) ¸ Interventions without substantial evidence Centre for Evidence-Based Medicine
Primary Interventions were Classified by Level: ¶ Evidence from Randomised Control Trials (better yet: systematic reviews of all relevant, high-quality RCTs) · Convincing non-experimental evidence (unnecessary & unethical to randomise) ¸ Interventions without substantial evidence Centre for Evidence-Based Medicine
 Conclusions from E-B oriented General Medicine: 82% of our patients received evidencebased care. ¶ treatments for 53% were justified by RCTs or systematic reviews of RCTs. è Of 28 relevant RCTs and SRs, 21 were accessible within seconds. · treatments for 29% were justified by convincing non-experimental evidence l Centre for Evidence-Based Medicine
Conclusions from E-B oriented General Medicine: 82% of our patients received evidencebased care. ¶ treatments for 53% were justified by RCTs or systematic reviews of RCTs. è Of 28 relevant RCTs and SRs, 21 were accessible within seconds. · treatments for 29% were justified by convincing non-experimental evidence l Centre for Evidence-Based Medicine
 36% had Cardiovascular diagnoses: » Ischaemic heart disease 17%") Evidence from RCTs l (53%) 36% had Cardiovascular diagnoses: » Ischaemic heart disease 17% » Heart failure 6% » Arrhythmia 2% » Thromboembolism 3% » Cerebrovascular 8% Centre for Evidence-Based Medicine
Evidence from RCTs l (53%) 36% had Cardiovascular diagnoses: » Ischaemic heart disease 17% » Heart failure 6% » Arrhythmia 2% » Thromboembolism 3% » Cerebrovascular 8% Centre for Evidence-Based Medicine
 7% had taken poison l 5% received chemotherapy or analgesia") Evidence from RCTs (53%) 7% had taken poison l 5% received chemotherapy or analgesia for cancer l 3 % had gastrointestinal disorders l 2% had obstructive airways disease l Centre for Evidence-Based Medicine
Evidence from RCTs (53%) 7% had taken poison l 5% received chemotherapy or analgesia for cancer l 3 % had gastrointestinal disorders l 2% had obstructive airways disease l Centre for Evidence-Based Medicine
 Infections 15% l Cardiac disorders 7% l Miscellany (non-compliance, drug") Convincing non-experimental evidence (29%) Infections 15% l Cardiac disorders 7% l Miscellany (non-compliance, drug reactions, bowel or bladder neck obstruction, dehydration, micturition syncope) 7% l Centre for Evidence-Based Medicine
Convincing non-experimental evidence (29%) Infections 15% l Cardiac disorders 7% l Miscellany (non-compliance, drug reactions, bowel or bladder neck obstruction, dehydration, micturition syncope) 7% l Centre for Evidence-Based Medicine
 l Specific symptomatic and supportive care for mild poisoning,") Interventions without substantial evidence (18%) l Specific symptomatic and supportive care for mild poisoning, non-cardiac chest pain, viral (non-herpetic) meningitis, terminal CNS disease, confusion, and food poisoning. Centre for Evidence-Based Medicine
Interventions without substantial evidence (18%) l Specific symptomatic and supportive care for mild poisoning, non-cardiac chest pain, viral (non-herpetic) meningitis, terminal CNS disease, confusion, and food poisoning. Centre for Evidence-Based Medicine
 Better Outcomes for Patients When EBM Is Practised E-B practise vs. Outcome in stroke (US): l When cared for by E-B neurologists, patients were 44% more likely to receive warfarin, and much more likely to be placed in a stroke care unit, l And were 22% less likely to die in the next 90 days. l (Mitchell et al: stroke 1996; 27: 1937 -43) Centre for Evidence-Based Medicine
Better Outcomes for Patients When EBM Is Practised E-B practise vs. Outcome in stroke (US): l When cared for by E-B neurologists, patients were 44% more likely to receive warfarin, and much more likely to be placed in a stroke care unit, l And were 22% less likely to die in the next 90 days. l (Mitchell et al: stroke 1996; 27: 1937 -43) Centre for Evidence-Based Medicine
 Centres for Evidence-Based Surgery l E-B General/Vascular Unit in Liverpool: » 95% received evidence-based Rx l l l 24% Level 1 71% Level 2 E-B Paediatric Unit in Liverpool: » 77% received evidence-based Rx l l 11% Level 1 66% Level 2 Centre for Evidence-Based Medicine
Centres for Evidence-Based Surgery l E-B General/Vascular Unit in Liverpool: » 95% received evidence-based Rx l l l 24% Level 1 71% Level 2 E-B Paediatric Unit in Liverpool: » 77% received evidence-based Rx l l 11% Level 1 66% Level 2 Centre for Evidence-Based Medicine
 Worse Outcomes for Patients When EBM Is Not Practised: l l l In a city-wide study of E-B practise vs. Outcome in carotid stenosis: Generated E-B indications for endarterectomy and reviewed 291 pts. Found the surgical indications: » Appropriate in 33% » Questionable in 49% » Inappropriate in 18% Centre for Evidence-Based Medicine
Worse Outcomes for Patients When EBM Is Not Practised: l l l In a city-wide study of E-B practise vs. Outcome in carotid stenosis: Generated E-B indications for endarterectomy and reviewed 291 pts. Found the surgical indications: » Appropriate in 33% » Questionable in 49% » Inappropriate in 18% Centre for Evidence-Based Medicine
 Worse Outcomes for Patients When EBM Is Not Practised Stroke or death within the next 30 days: l Expected (if left alone): 0. 5% l Expected (if properly selected and operated): 1. 5% l Observed among operated patients (2/3 operated for questionable or inappropriate reasons): >5% l Wong et al. Stroke 1997; 28: 891 -8. Centre for Evidence-Based Medicine
Worse Outcomes for Patients When EBM Is Not Practised Stroke or death within the next 30 days: l Expected (if left alone): 0. 5% l Expected (if properly selected and operated): 1. 5% l Observed among operated patients (2/3 operated for questionable or inappropriate reasons): >5% l Wong et al. Stroke 1997; 28: 891 -8. Centre for Evidence-Based Medicine
 »") Evidence-Based Ambulatory Paediatrics l 54% of manoeuvres were evidencebased (“experts” had predicted <20%) » 77% of diagnostic manoeuvres » 67% of treatments » 59% of health promotion Centre for Evidence-Based Medicine
Evidence-Based Ambulatory Paediatrics l 54% of manoeuvres were evidencebased (“experts” had predicted <20%) » 77% of diagnostic manoeuvres » 67% of treatments » 59% of health promotion Centre for Evidence-Based Medicine
 » 67% treated on the basis of") Centres for Evidence-Based Psychiatry l In-Patients (Oxford) » 67% treated on the basis of RCTs l Out-Patient » >80% received evidence-based Rx Centre for Evidence-Based Medicine
Centres for Evidence-Based Psychiatry l In-Patients (Oxford) » 67% treated on the basis of RCTs l Out-Patient » >80% received evidence-based Rx Centre for Evidence-Based Medicine
 practice. l 81%") Evidence-Based General Practice 122 consecutive consultations in a suburban (Leeds, UK) practice. l 81% evidence-based: » 31% based on RCTs or overviews » 50% based on convincing non-experimental evidence » 19% without substantial evidence (Gill et al, BMJ 1996; 312: 819 -21) Centre for Evidence-Based Medicine
Evidence-Based General Practice 122 consecutive consultations in a suburban (Leeds, UK) practice. l 81% evidence-based: » 31% based on RCTs or overviews » 50% based on convincing non-experimental evidence » 19% without substantial evidence (Gill et al, BMJ 1996; 312: 819 -21) Centre for Evidence-Based Medicine
 Can we get evidence to the bedside? Need it within seconds if it is to be incorporated into busy clinical rounds l Our initial attempts to bring the best evidence to a busy clinical team caring for 200+ admissions per month l Centre for Evidence-Based Medicine
Can we get evidence to the bedside? Need it within seconds if it is to be incorporated into busy clinical rounds l Our initial attempts to bring the best evidence to a busy clinical team caring for 200+ admissions per month l Centre for Evidence-Based Medicine
 Searching for Evidence in the Month Before the Cart: Expected searches = 98 l Identified searching needs = 72 l Only 19 searches (26%) carried out. l Centre for Evidence-Based Medicine
Searching for Evidence in the Month Before the Cart: Expected searches = 98 l Identified searching needs = 72 l Only 19 searches (26%) carried out. l Centre for Evidence-Based Medicine
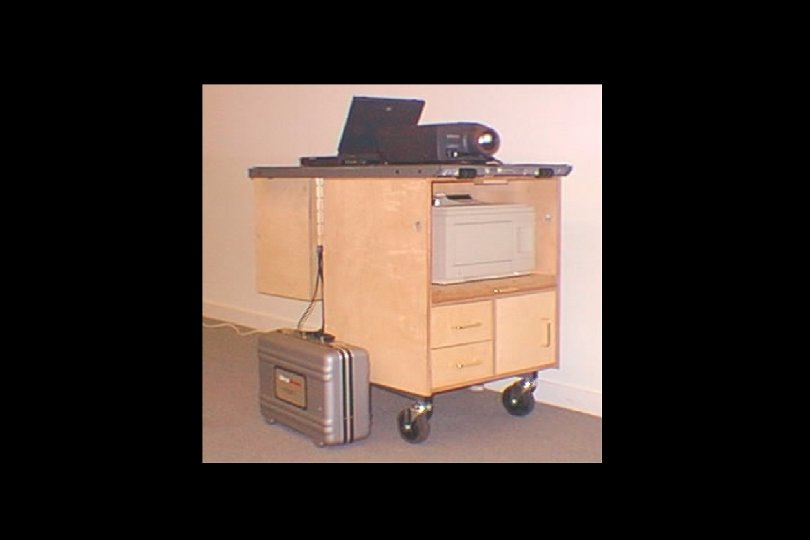
 Contents of the Cart: l l Infra-red simultaneous stethoscope with 12 remote receivers. Physical diagnosis text book and reprints (JAMA Rational Clinical Exam). Notebook computer, computer projector, and pop-out screen. Rapid printer. Centre for Evidence-Based Medicine
Contents of the Cart: l l Infra-red simultaneous stethoscope with 12 remote receivers. Physical diagnosis text book and reprints (JAMA Rational Clinical Exam). Notebook computer, computer projector, and pop-out screen. Rapid printer. Centre for Evidence-Based Medicine
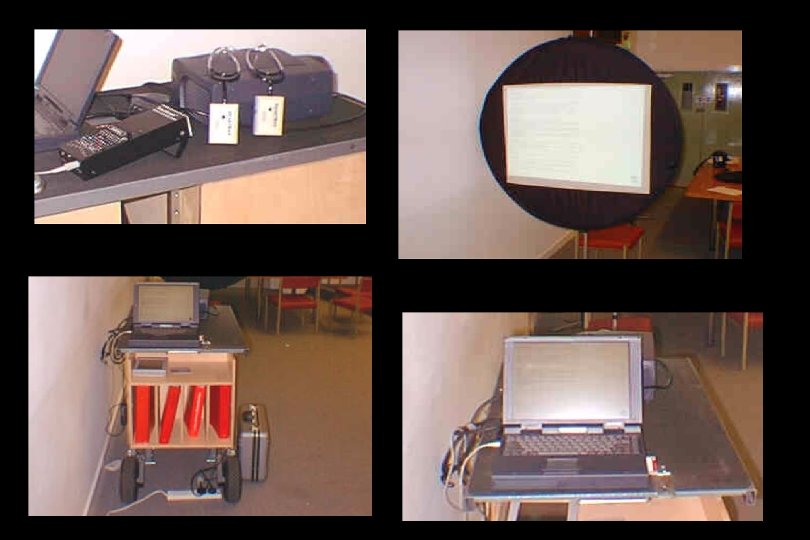
: Library Round-Trip = 7 min l 125 summaries (1") Contents of the Cart (cont): Library Round-Trip = 7 min l 125 summaries (1 -3 pp) of evidence previously appraised and summarised by Side A teams (in the form of “Redbook” entries or Critically-Appraised Topics : “CATs”). Access Time to the “bottom line” = 12 sec. Centre for Evidence-Based Medicine
Contents of the Cart (cont): Library Round-Trip = 7 min l 125 summaries (1 -3 pp) of evidence previously appraised and summarised by Side A teams (in the form of “Redbook” entries or Critically-Appraised Topics : “CATs”). Access Time to the “bottom line” = 12 sec. Centre for Evidence-Based Medicine


: Library Round-Trip = 7 min l CD of Best") Contents of the Cart (cont): Library Round-Trip = 7 min l CD of Best Evidence Access Time to the “bottom line” = 26 sec. l CD of Win. SPIRS (5 -year clinical subsets) Access Time to useful abstract = 90 sec. (so used for filling Educational Rx after rounds) l CD of the Cochrane Library (used for filling Educational Rx after rounds) Centre for Evidence-Based Medicine
Contents of the Cart (cont): Library Round-Trip = 7 min l CD of Best Evidence Access Time to the “bottom line” = 26 sec. l CD of Win. SPIRS (5 -year clinical subsets) Access Time to useful abstract = 90 sec. (so used for filling Educational Rx after rounds) l CD of the Cochrane Library (used for filling Educational Rx after rounds) Centre for Evidence-Based Medicine
 Usefulness of the Cart: l 81% of searches were for evidence that could affect diagnostic and/or treatment decisions. l 90% of these searches were successful in finding useful evidence. * Centre for Evidence-Based Medicine
Usefulness of the Cart: l 81% of searches were for evidence that could affect diagnostic and/or treatment decisions. l 90% of these searches were successful in finding useful evidence. * Centre for Evidence-Based Medicine
:") Of the successful searches (from the perspective of the most junior responsible team member): l 52% confirmed diagnostic and/or management decisions l 23% led to changes in existing decisions l 25% led to additional decisions Centre for Evidence-Based Medicine
Of the successful searches (from the perspective of the most junior responsible team member): l 52% confirmed diagnostic and/or management decisions l 23% led to changes in existing decisions l 25% led to additional decisions Centre for Evidence-Based Medicine
 Searching for Evidence in a 3 day period after the Cart: Expected searches = 10 l Identified searching needs = 41 l Only 5 searches (12%) carried out. l Centre for Evidence-Based Medicine
Searching for Evidence in a 3 day period after the Cart: Expected searches = 10 l Identified searching needs = 41 l Only 5 searches (12%) carried out. l Centre for Evidence-Based Medicine
 Can we get evidence to the bedside? Yes, and it will improve patient care. l But can we provide it in a less cumbersome form? l Centre for Evidence-Based Medicine
Can we get evidence to the bedside? Yes, and it will improve patient care. l But can we provide it in a less cumbersome form? l Centre for Evidence-Based Medicine
 EBM and Purchasing In harmony: Ê When we clinicians stop doing things that are useless or harmful Ë When we use just-as-good but less expensive treatments, carers, and sites for care. Centre for Evidence-Based Medicine
EBM and Purchasing In harmony: Ê When we clinicians stop doing things that are useless or harmful Ë When we use just-as-good but less expensive treatments, carers, and sites for care. Centre for Evidence-Based Medicine
 What we could save in Oxford by switching from: LASIX êfrusemide: £ 90, 000 simvastatin êcerivastatin: £ 500, 000 TENORMIN êatenolol: £ 700, 000 diclofenac êibuprofen: £ 1, 000 Total: £ 2, 290, 000 l how many hips would these savings purchase? Centre for Evidence-Based Medicine
What we could save in Oxford by switching from: LASIX êfrusemide: £ 90, 000 simvastatin êcerivastatin: £ 500, 000 TENORMIN êatenolol: £ 700, 000 diclofenac êibuprofen: £ 1, 000 Total: £ 2, 290, 000 l how many hips would these savings purchase? Centre for Evidence-Based Medicine
 EBM and Purchasing Still in harmony: Ì When we spend now to save later. Centre for Evidence-Based Medicine
EBM and Purchasing Still in harmony: Ì When we spend now to save later. Centre for Evidence-Based Medicine
 EBM and Purchasing In grudging collaboration: Í Waiting lists, once we understand the opportunity costs of shortening them: » it’s not about money » it’s about what else we won’t be able to do if we shorten them Centre for Evidence-Based Medicine
EBM and Purchasing In grudging collaboration: Í Waiting lists, once we understand the opportunity costs of shortening them: » it’s not about money » it’s about what else we won’t be able to do if we shorten them Centre for Evidence-Based Medicine
 EBM and Purchasing In conflict: Î When we identify so strongly with a dying patient’s short-term goals that we use resources that we know would “add more QALYs” if used for other patients. Centre for Evidence-Based Medicine
EBM and Purchasing In conflict: Î When we identify so strongly with a dying patient’s short-term goals that we use resources that we know would “add more QALYs” if used for other patients. Centre for Evidence-Based Medicine