

ceb83d63cd2fb4684a9086ffd40f762d.ppt
- Количество слайдов: 39
 The potential impact of ICT on Service Planning for Health Services Craig Guscott Andrew P. Howard Manager, South East Metropolitan Service & Capital Planning, Department of Health Chief Information Officer, Department of Health
The potential impact of ICT on Service Planning for Health Services Craig Guscott Andrew P. Howard Manager, South East Metropolitan Service & Capital Planning, Department of Health Chief Information Officer, Department of Health
 Presentation Content Setting the Picture Advances in Information Communication Technology Potential ICT Impacts on: Preventing presentations to the Health System Delivery of Health services during intervention Preventing re-admission Potential Qualitative Benefits of ICT on Service Delivery Potential Quantitative Impacts of ICT on Service Delivery
Presentation Content Setting the Picture Advances in Information Communication Technology Potential ICT Impacts on: Preventing presentations to the Health System Delivery of Health services during intervention Preventing re-admission Potential Qualitative Benefits of ICT on Service Delivery Potential Quantitative Impacts of ICT on Service Delivery
 Advances in Information Communication Technology
Advances in Information Communication Technology
 New communication devices are a frequent event
New communication devices are a frequent event

 Whilst some in the health field are finding the transition to new technology difficult……
Whilst some in the health field are finding the transition to new technology difficult……
 Others are pushing into the future…
Others are pushing into the future…
 The Ever-Present Need and Future-pressing Need Demand on health service provision growths yearly Innovative and effective mitigation strategies are needed to be developed to meet this current and projected need Effective ICT solutions are essential if the system is to respond to the known factors of increasing: • Presentations (demand) • Chronic disease (complexity) • Transparency & clinical governance • Community expectations • Workforce shortages
The Ever-Present Need and Future-pressing Need Demand on health service provision growths yearly Innovative and effective mitigation strategies are needed to be developed to meet this current and projected need Effective ICT solutions are essential if the system is to respond to the known factors of increasing: • Presentations (demand) • Chronic disease (complexity) • Transparency & clinical governance • Community expectations • Workforce shortages
 Possible impact of ICT on meeting bed demand How can current ICT technology assist the State/Nation in meeting current and growing health service provision demand? When planning for the future, what can the Service Planner safely assume? When planning for the future, what should the Service Planner be advocating for as a strategy to mitigate demand? What can be done to reduce the need to build more beds, reduce recurrent costs all while meeting demand for health service provision?
Possible impact of ICT on meeting bed demand How can current ICT technology assist the State/Nation in meeting current and growing health service provision demand? When planning for the future, what can the Service Planner safely assume? When planning for the future, what should the Service Planner be advocating for as a strategy to mitigate demand? What can be done to reduce the need to build more beds, reduce recurrent costs all while meeting demand for health service provision?
 Context of Disussion Looking at four of the main types of presentations to the health system which can be impacted positively by current ICT enablers Ambulatory Care Sensitive Conditions • Vaccine Preventable ACSC’s • Acute ACSC’s • Chronic ACSC’s Acute Multiday presentations
Context of Disussion Looking at four of the main types of presentations to the health system which can be impacted positively by current ICT enablers Ambulatory Care Sensitive Conditions • Vaccine Preventable ACSC’s • Acute ACSC’s • Chronic ACSC’s Acute Multiday presentations
 Potential ICT Impacts on: Preventing presentations to the Health System Can ICT enablers reduce the number of original/first presentations? What Preventable illnesses/diseases/injuries can be prevented by ICT enablers?
Potential ICT Impacts on: Preventing presentations to the Health System Can ICT enablers reduce the number of original/first presentations? What Preventable illnesses/diseases/injuries can be prevented by ICT enablers?
 Lifestyle Disease Lifestyle disease: A disease associated with the way a person or group of people lives. Lifestyle diseases include: • atherosclerosis, heart disease, and stroke; • obesity and type 2 diabetes; • diseases associated with smoking and alcohol and drug abuse, such as cirrhosis, cancer, COPD,
Lifestyle Disease Lifestyle disease: A disease associated with the way a person or group of people lives. Lifestyle diseases include: • atherosclerosis, heart disease, and stroke; • obesity and type 2 diabetes; • diseases associated with smoking and alcohol and drug abuse, such as cirrhosis, cancer, COPD,
 Ambulatory Care Sensitive Condition’s Vaccine Preventable ACSC’s • prevention of disease occurence • influenza, bacterial pneumonia, tetanus, mumps, rubella, pertussis, polio • For these conditions, it is the actual condition that is deemed preventable rather than the hospitalisation. Acute ACSC’s • avoidable hospitalization for acute disease • gastro, kidney infection, perforated ulcer, cellulitis, PID, ENT infections, dental conditions • These conditions may not be preventable in themselves but theoretically should not result in hospitalisation if adequate and timely primary care is received.
Ambulatory Care Sensitive Condition’s Vaccine Preventable ACSC’s • prevention of disease occurence • influenza, bacterial pneumonia, tetanus, mumps, rubella, pertussis, polio • For these conditions, it is the actual condition that is deemed preventable rather than the hospitalisation. Acute ACSC’s • avoidable hospitalization for acute disease • gastro, kidney infection, perforated ulcer, cellulitis, PID, ENT infections, dental conditions • These conditions may not be preventable in themselves but theoretically should not result in hospitalisation if adequate and timely primary care is received.
 Main Potential Impact Education Public Awareness Communication Monitoring
Main Potential Impact Education Public Awareness Communication Monitoring
 Vaccine Preventable ACSC’s In Victoria 2009 -2010 All MD Separations = 3, 026 for 27, 532 Bed-days at 9. 1 av. ALOS Equates to 89 beds occupied 365 days/yr at 85% efficiency (Interestingly HITH = 88 seps for 1, 903 bed-days at 21. 63 av. ALOS) Possible Impact of ICT enablers if: 1% reduction in MD separations = 1 bed 1% reduction in av. LOS = 1 bed 1 day reduction in av. LOS = 10 beds
Vaccine Preventable ACSC’s In Victoria 2009 -2010 All MD Separations = 3, 026 for 27, 532 Bed-days at 9. 1 av. ALOS Equates to 89 beds occupied 365 days/yr at 85% efficiency (Interestingly HITH = 88 seps for 1, 903 bed-days at 21. 63 av. ALOS) Possible Impact of ICT enablers if: 1% reduction in MD separations = 1 bed 1% reduction in av. LOS = 1 bed 1 day reduction in av. LOS = 10 beds
 Acute ACSC’s In Victoria 2009/10 All MD Separations: 32, 773 seps for 141, 093 bed-days at 4. 31 av. LOS Equates to 455 beds occupied 365 days/yr at 85% efficiency Possible impact of ICT enablers if: • 1% reduction in separations = 4 beds • 1% reduction in av. LOS = 4 beds • 1 day reduction in av. LOS = 105 beds
Acute ACSC’s In Victoria 2009/10 All MD Separations: 32, 773 seps for 141, 093 bed-days at 4. 31 av. LOS Equates to 455 beds occupied 365 days/yr at 85% efficiency Possible impact of ICT enablers if: • 1% reduction in separations = 4 beds • 1% reduction in av. LOS = 4 beds • 1 day reduction in av. LOS = 105 beds
 Potential ICT Impacts on: Delivery of Health services during intervention How can ICT assist in reducing Length of Stay (LOS) during a Multiday intervention?
Potential ICT Impacts on: Delivery of Health services during intervention How can ICT assist in reducing Length of Stay (LOS) during a Multiday intervention?
 Today’s Hospital Vs the Hospital of the Future – Facility Design Hospital of Today Hospital of the Future Centralised nurses stations Care provided in ‘physical’ hospital Queuing and waiting – large waiting areas • De-centralised nurses stations • ‘Virtual’ hospital in the community • Improved patient flow – JIT approach – smaller waiting areas • JIT stock control – less storage areas • Acuity adaptable / flexible rooms – patients stay in same bed • Quiet hospital – sound absorbing materials, direct messaging, • Information booths – interactive, printed maps • Staff off-site (e. g. video-conferencing, mobile technologies, etc. ) Supplies stockpiled – lots of storage req’d Specific purpose rooms – patients moved as condition changes Noisy hospital – nurse call, pagers, phones, alarms, overhead announcements Wayfinding - fixed signage, confusing, outof-date information Staff in situ
Today’s Hospital Vs the Hospital of the Future – Facility Design Hospital of Today Hospital of the Future Centralised nurses stations Care provided in ‘physical’ hospital Queuing and waiting – large waiting areas • De-centralised nurses stations • ‘Virtual’ hospital in the community • Improved patient flow – JIT approach – smaller waiting areas • JIT stock control – less storage areas • Acuity adaptable / flexible rooms – patients stay in same bed • Quiet hospital – sound absorbing materials, direct messaging, • Information booths – interactive, printed maps • Staff off-site (e. g. video-conferencing, mobile technologies, etc. ) Supplies stockpiled – lots of storage req’d Specific purpose rooms – patients moved as condition changes Noisy hospital – nurse call, pagers, phones, alarms, overhead announcements Wayfinding - fixed signage, confusing, outof-date information Staff in situ
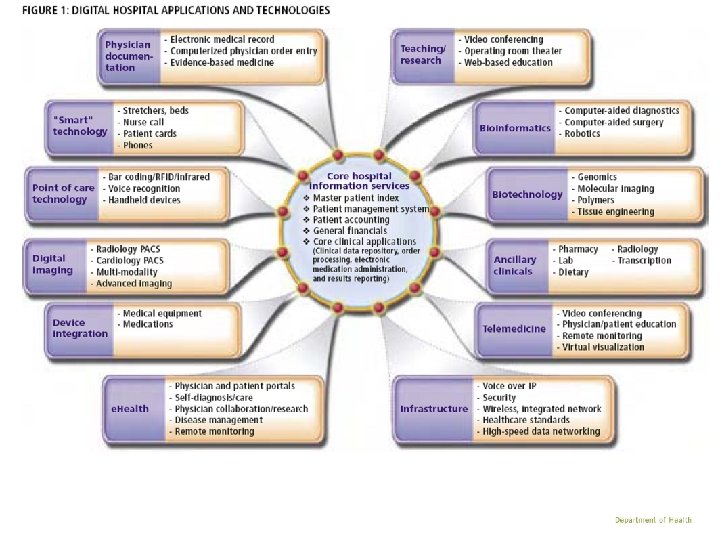
 Today’s Hospital Vs the Hospital of the Future Hospital of Today Hospital of the Future Paper-based medical records Manual or non-integrated ICT systems for: • Patient registration • Patients bookings • Discharge forms • Referral forms • Paper prescriptions • Clinical decision support • Alert (allergy) management • Equipment control • Ward stock control • Menu ordering Electronic Medical Record ICT enabled systems for: • On-line patient registration and bookings • Electronic discharge summaries • e-ordering - pathology, imaging, etc. • e. Prescribing • Electronic Clinical Decision Support • Allergy alerts • RFID tracking for equipment & stock control • Electronic menu ordering from patient bedside monitor
Today’s Hospital Vs the Hospital of the Future Hospital of Today Hospital of the Future Paper-based medical records Manual or non-integrated ICT systems for: • Patient registration • Patients bookings • Discharge forms • Referral forms • Paper prescriptions • Clinical decision support • Alert (allergy) management • Equipment control • Ward stock control • Menu ordering Electronic Medical Record ICT enabled systems for: • On-line patient registration and bookings • Electronic discharge summaries • e-ordering - pathology, imaging, etc. • e. Prescribing • Electronic Clinical Decision Support • Allergy alerts • RFID tracking for equipment & stock control • Electronic menu ordering from patient bedside monitor
 All Acute Multiday Presentations In Victoria 2009 -10 All separations = 867, 041 for 3, 888, 676 bed-days at 4. 48 av. LOS Equates to 12, 534 beds occupied 365 days/yr at 85% efficiency Possible impact of ICT enablers if: • Reduce av. LOS by 1% = 139 beds • Reduce av. LOS by 1 day = 2, 808 beds
All Acute Multiday Presentations In Victoria 2009 -10 All separations = 867, 041 for 3, 888, 676 bed-days at 4. 48 av. LOS Equates to 12, 534 beds occupied 365 days/yr at 85% efficiency Possible impact of ICT enablers if: • Reduce av. LOS by 1% = 139 beds • Reduce av. LOS by 1 day = 2, 808 beds
 Potential ICT Impacts on: Preventing re-admission Can ICT assist in preventing patients from requiring additional multiday stays in our acute hospitals?
Potential ICT Impacts on: Preventing re-admission Can ICT assist in preventing patients from requiring additional multiday stays in our acute hospitals?
 Potential ICT Impacts on: Preventing re-admission Chronic ACSCs Chronic conditions are usually not self-limiting and can lead to extensive use of medical services. This category includes avoidable hospitalisation for selected chronic disease, for example, diabetes, asthma, angina, hypertension, congestive heart failure, chronic obstructive pulmonary disease (COPD). In this case, although these conditions may be preventable through behaviour modification and lifestyle change, they can also be managed effectively through primary care in order to prevent deterioration and hospitalisation.
Potential ICT Impacts on: Preventing re-admission Chronic ACSCs Chronic conditions are usually not self-limiting and can lead to extensive use of medical services. This category includes avoidable hospitalisation for selected chronic disease, for example, diabetes, asthma, angina, hypertension, congestive heart failure, chronic obstructive pulmonary disease (COPD). In this case, although these conditions may be preventable through behaviour modification and lifestyle change, they can also be managed effectively through primary care in order to prevent deterioration and hospitalisation.
 Chronic Disease Management Patient Portals for • ICT can help prevent hospital admissions through improved monitoring of the patient Study found 83% decrease in admission rate for CHF patients 1 86% lower readmission costs (US$5, 850 vs US$44, 479)1 Fewer CHF related emergency department visits 2 • Tele-health and Home health – home monitoring & ability to link distant patient & provider Example: Kaiser Permanente Home Health Program Study of 212 patients (102 on telehealth) Av. cost of care – US$1, 948 intervention vs US$2, 674 control with difference attributed to hospitalisation costs Improved patient satisfaction in intervention group 3 1 Roglieri et al, 1997 2 Jerant et al, 2001 3 Johnston et al, 2000
Chronic Disease Management Patient Portals for • ICT can help prevent hospital admissions through improved monitoring of the patient Study found 83% decrease in admission rate for CHF patients 1 86% lower readmission costs (US$5, 850 vs US$44, 479)1 Fewer CHF related emergency department visits 2 • Tele-health and Home health – home monitoring & ability to link distant patient & provider Example: Kaiser Permanente Home Health Program Study of 212 patients (102 on telehealth) Av. cost of care – US$1, 948 intervention vs US$2, 674 control with difference attributed to hospitalisation costs Improved patient satisfaction in intervention group 3 1 Roglieri et al, 1997 2 Jerant et al, 2001 3 Johnston et al, 2000
 Issue • Multi-disciplinary and community-based care provides") Chronic Heart failure Assessment by Telephone (CHAT) Issue • Multi-disciplinary and community-based care provides substantial benefit to patients with chronic heart failure (CHF) • However, models may not be ideally suited to the care of the rural and remote CHF patient where there are issues of access to these services • Telephone support of the CHF patient may help overcome problems of access Study Aims • To determine whether automated telephone support will improve quality of life and reduce death & hospital admissions for rural and remote CHF patients • To test this system of care as an exemplar of a novel chronic disease management strategy in areas remote from access to multi-disciplinary care • To determine the cost effectiveness of this intervention
Chronic Heart failure Assessment by Telephone (CHAT) Issue • Multi-disciplinary and community-based care provides substantial benefit to patients with chronic heart failure (CHF) • However, models may not be ideally suited to the care of the rural and remote CHF patient where there are issues of access to these services • Telephone support of the CHF patient may help overcome problems of access Study Aims • To determine whether automated telephone support will improve quality of life and reduce death & hospital admissions for rural and remote CHF patients • To test this system of care as an exemplar of a novel chronic disease management strategy in areas remote from access to multi-disciplinary care • To determine the cost effectiveness of this intervention
 Key Findings Automated telephone support to the") Chronic Heart failure Assessment by Telephone (CHAT) Key Findings Automated telephone support to the rural & remote CHF patient resulted in: • No change in the Packer clinical composite score • Significant reduction in risk of: • All-cause death & hospitalisation • All-cause hospitalisation • Non-significant reduction in risk of: • HF hospitalisation • No difference in all-cause mortality Still to be determined is the impact of telephone support to these patients on ACE inhibitor use & dose, cost-efficacy and plasma NT-pro BNP levels Significant beneficial impacts were observed on some (but not all) relevant clinical outcome parameters
Chronic Heart failure Assessment by Telephone (CHAT) Key Findings Automated telephone support to the rural & remote CHF patient resulted in: • No change in the Packer clinical composite score • Significant reduction in risk of: • All-cause death & hospitalisation • All-cause hospitalisation • Non-significant reduction in risk of: • HF hospitalisation • No difference in all-cause mortality Still to be determined is the impact of telephone support to these patients on ACE inhibitor use & dose, cost-efficacy and plasma NT-pro BNP levels Significant beneficial impacts were observed on some (but not all) relevant clinical outcome parameters
 Chronic ACSC’s In Victoria 2009 -2010 All MD Separations = 83, 580 for 663, 052 Bed-days at 7. 93 av. ALOS Equates to 2, 137 beds occupied 365 days/yr at 85% efficiency Possible Impact of ICT enablers if: 1% reduction in MD separations = 22 beds Reduce av. LOS by 1% = 22 beds 1 day reduction in av. LOS = 270 beds
Chronic ACSC’s In Victoria 2009 -2010 All MD Separations = 83, 580 for 663, 052 Bed-days at 7. 93 av. ALOS Equates to 2, 137 beds occupied 365 days/yr at 85% efficiency Possible Impact of ICT enablers if: 1% reduction in MD separations = 22 beds Reduce av. LOS by 1% = 22 beds 1 day reduction in av. LOS = 270 beds
 Potential Qualitative Benefits of ICT on Service Delivery
Potential Qualitative Benefits of ICT on Service Delivery
 Benefits of ICT To the Patient To the Health System • Improved quality of care • Improved access to reliable health information when & where it is needed • More patient focused integrated care • Improved cost effectiveness • Improved patient safety • Improved access to healthcare • Improved continuity of care • Close the gap between rural and remote healthcare providers & patients • Lives saved through better decision support, increased access to information & reduced adverse events. • Improved healthcare planning by ensuring resources directed to where most needed • Enhanced shared care for complex medical problems & chronic disease • Encourage innovation to deliver improvements in health sector productivity • Reduced burden on health sector through better health management (e. g. reduced duplication of tests, visits, procedures & capital expenditure)
Benefits of ICT To the Patient To the Health System • Improved quality of care • Improved access to reliable health information when & where it is needed • More patient focused integrated care • Improved cost effectiveness • Improved patient safety • Improved access to healthcare • Improved continuity of care • Close the gap between rural and remote healthcare providers & patients • Lives saved through better decision support, increased access to information & reduced adverse events. • Improved healthcare planning by ensuring resources directed to where most needed • Enhanced shared care for complex medical problems & chronic disease • Encourage innovation to deliver improvements in health sector productivity • Reduced burden on health sector through better health management (e. g. reduced duplication of tests, visits, procedures & capital expenditure)
 Hours spent by Medical Staff in Direct Patient Care Number of hours of direct patient care is decreasing across all medical specialties
Hours spent by Medical Staff in Direct Patient Care Number of hours of direct patient care is decreasing across all medical specialties
 Potential Quantitative Impacts of ICT on Service Delivery
Potential Quantitative Impacts of ICT on Service Delivery
 ICT in the Clinical Setting Clinical Decision Support More efficient work flow Fewer adverse events – alert system Improved patient outcomes Decreased length of stay Fewer re-admissions
ICT in the Clinical Setting Clinical Decision Support More efficient work flow Fewer adverse events – alert system Improved patient outcomes Decreased length of stay Fewer re-admissions
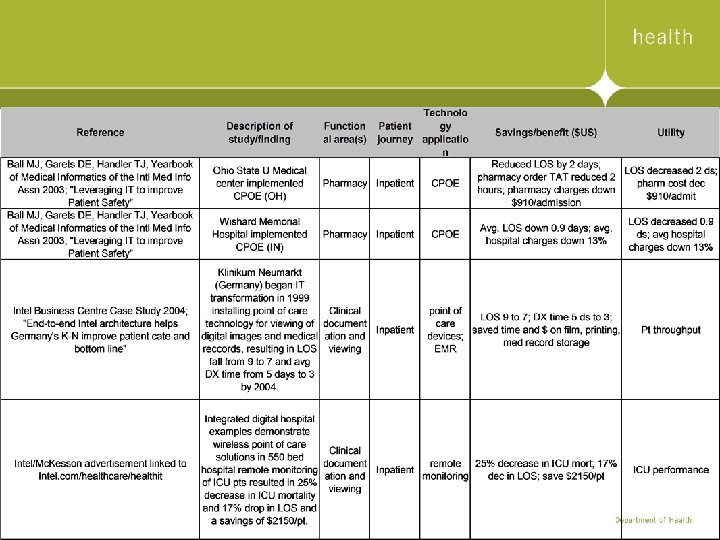
 ICT Benefits Some of the healthcare delivery improvements documented by organizations include: • Using wireless point-of-care solutions has resulted in reductions in nursing staff administrative workload of up to two hours per nurse, per shift, allowing for more time in direct patient care. • At a 550 -bed hospital, remote monitoring of ICU patients has led to a 25 percent decrease in hospital mortality rates for ICU patients, a 17 percent decrease in ICU length of stay, and a savings of $2, 150 per patient. • More than 50 hospitals using automated medication administration solutions prevented more than 29, 000 adverse drug events (ADE) weekly. Source: Mc. Kesson corporation, 2005
ICT Benefits Some of the healthcare delivery improvements documented by organizations include: • Using wireless point-of-care solutions has resulted in reductions in nursing staff administrative workload of up to two hours per nurse, per shift, allowing for more time in direct patient care. • At a 550 -bed hospital, remote monitoring of ICU patients has led to a 25 percent decrease in hospital mortality rates for ICU patients, a 17 percent decrease in ICU length of stay, and a savings of $2, 150 per patient. • More than 50 hospitals using automated medication administration solutions prevented more than 29, 000 adverse drug events (ADE) weekly. Source: Mc. Kesson corporation, 2005
 ICT Benefits Up to 88% reduction in drug errors (Brigham & Womens Hospital; Montefiore Medical Center; Peace. Health Community, ) Reduced staffing need(Indiana Heart Hospital; Tiantan Hospital, Beijing) Productivity increases up to 35% (Peace. Health Community; Tiantan Hospital, Beijing) Reduced ALOS by between 0. 9 – 2 days Source: Mc. Kesson corporation, 2005
ICT Benefits Up to 88% reduction in drug errors (Brigham & Womens Hospital; Montefiore Medical Center; Peace. Health Community, ) Reduced staffing need(Indiana Heart Hospital; Tiantan Hospital, Beijing) Productivity increases up to 35% (Peace. Health Community; Tiantan Hospital, Beijing) Reduced ALOS by between 0. 9 – 2 days Source: Mc. Kesson corporation, 2005
 Conclusion ICT investment in the health system can facilitate: • improved patient outcomes • improved patient & work flow • enhanced chronic disease management • reduce the need for additional resources Reduce the growth in recurrent expense Reduce the growth of capital expense
Conclusion ICT investment in the health system can facilitate: • improved patient outcomes • improved patient & work flow • enhanced chronic disease management • reduce the need for additional resources Reduce the growth in recurrent expense Reduce the growth of capital expense