

09d65a74a5edac481f303cd3585b71a8.ppt
- Количество слайдов: 47
 The Nexfin HD Potential Applications Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESCTAIC Amsterdam 2010
The Nexfin HD Potential Applications Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESCTAIC Amsterdam 2010
 Disclosure The speaker cooperates with the following companies BMEYE PULSION
Disclosure The speaker cooperates with the following companies BMEYE PULSION
 Monitor wizards can be dangerous Robin ED, Mc. Cauley RF. Chest 1998; 114: 1511 What Is the Best Way To Measure Cardiac Output ? Who Cares, Anyway ? Caruso LJ et al. Chest. 2002; 122: 771 -774
Monitor wizards can be dangerous Robin ED, Mc. Cauley RF. Chest 1998; 114: 1511 What Is the Best Way To Measure Cardiac Output ? Who Cares, Anyway ? Caruso LJ et al. Chest. 2002; 122: 771 -774
 I have a suspicion that even the medical device manufacturers realize that CO is not an important variable in the critical care arena. …PPV alone is the best way to predict volume responsiveness. Therefore, it is less clear why we want to know the CO in the first place. This explains why all of the recently marketed devices purport a slew of other data (e. g. , stroke volume variance, EVLW, blood velocity), although many of these measurements are derived from CO determination to begin with.
I have a suspicion that even the medical device manufacturers realize that CO is not an important variable in the critical care arena. …PPV alone is the best way to predict volume responsiveness. Therefore, it is less clear why we want to know the CO in the first place. This explains why all of the recently marketed devices purport a slew of other data (e. g. , stroke volume variance, EVLW, blood velocity), although many of these measurements are derived from CO determination to begin with.
 The monitoring of. Bodiesis two Air France CO of considered passengers found to be very useful for CNN. COM Junedecision proper 6, 2009 The airline had failed to replace a part that monitors speed, recommended by -making in critically ill andashigh-risk the manufacturer, based on technological developments and surgical patients. improvements. The fact that this statement is not supported by EBM tells us more about the shortcomings of EBM than those of the measurement of CO.
The monitoring of. Bodiesis two Air France CO of considered passengers found to be very useful for CNN. COM Junedecision proper 6, 2009 The airline had failed to replace a part that monitors speed, recommended by -making in critically ill andashigh-risk the manufacturer, based on technological developments and surgical patients. improvements. The fact that this statement is not supported by EBM tells us more about the shortcomings of EBM than those of the measurement of CO.
 uses a non -invasive, continuous blood pressure (BP)") The Nexfin HD device (BMEYE, Amsterdam) uses a non -invasive, continuous blood pressure (BP) measurement (based on the Finapres method) to measure cardiac output continuously.
The Nexfin HD device (BMEYE, Amsterdam) uses a non -invasive, continuous blood pressure (BP) measurement (based on the Finapres method) to measure cardiac output continuously.
 Stover JF, et al. BMC Anesthesiology 2009: 9: 6
Stover JF, et al. BMC Anesthesiology 2009: 9: 6
 Stover JF, et al. BMC Anesthesiology 2009: 9: 6 Importantly, there were no clinical signs of disturbed microcirculation of the fingers in these patients during application of the finger cuff, indicating a safe use of the Nexfin HD system. The noninvasiveness of this technique allows to avoid complications related to more invasive techniques. This new system is very easy to use and quickly to install within minutes…could offer a quick initial hemodynamic overview…. on trend of MAP and CO. This would allow to bridge the time until a longer lasting invasive monitoring can be installed in the case of a deteriorating patient.
Stover JF, et al. BMC Anesthesiology 2009: 9: 6 Importantly, there were no clinical signs of disturbed microcirculation of the fingers in these patients during application of the finger cuff, indicating a safe use of the Nexfin HD system. The noninvasiveness of this technique allows to avoid complications related to more invasive techniques. This new system is very easy to use and quickly to install within minutes…could offer a quick initial hemodynamic overview…. on trend of MAP and CO. This would allow to bridge the time until a longer lasting invasive monitoring can be installed in the case of a deteriorating patient.
 Comparison of Nexfin HD CO to Pi. CCO intermittent TTD CO
Comparison of Nexfin HD CO to Pi. CCO intermittent TTD CO
 Pre CPB
Pre CPB
 Post CPB
Post CPB
 Why do we need real-time CCO? Intermittent TD CO measurements have a well known intrinsic limited reproducibility. This limitation makes them inferior to continuously measured real-time CO in assessing the response to therapeutic or diagnostic events with short time constants. Ø Fluid loading (e. g. , periop. optimization) Ø Passive leg raising, end-exp. occlusion. Ø Immediate response to inotropes
Why do we need real-time CCO? Intermittent TD CO measurements have a well known intrinsic limited reproducibility. This limitation makes them inferior to continuously measured real-time CO in assessing the response to therapeutic or diagnostic events with short time constants. Ø Fluid loading (e. g. , periop. optimization) Ø Passive leg raising, end-exp. occlusion. Ø Immediate response to inotropes
 Nexfin HD Applications Syncope diagnostics - tilt table testing
Nexfin HD Applications Syncope diagnostics - tilt table testing
 declined by a mean of 1. 4 L/min. Conclusions:") Upon standing postoperatively, CO (Modelflow) declined by a mean of 1. 4 L/min. Conclusions: The early postoperative postural cardiovascular response is impaired after radical prostatectomy with a risk of orthostatic intolerance, limiting early postoperative mobilization.
Upon standing postoperatively, CO (Modelflow) declined by a mean of 1. 4 L/min. Conclusions: The early postoperative postural cardiovascular response is impaired after radical prostatectomy with a risk of orthostatic intolerance, limiting early postoperative mobilization.
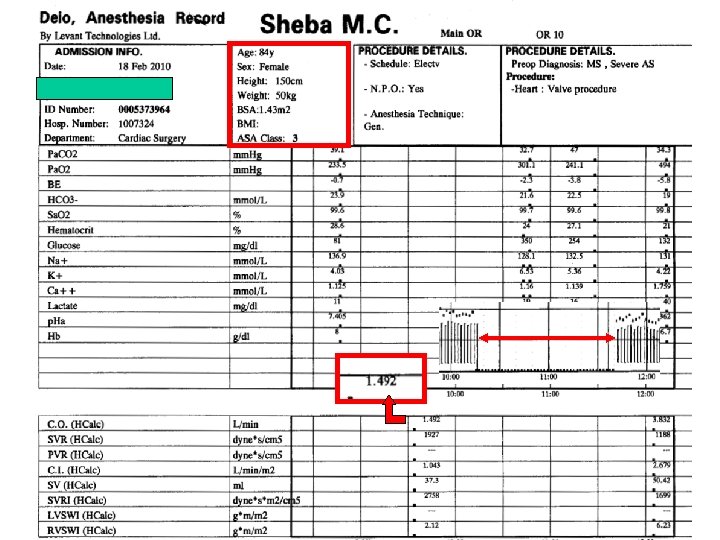
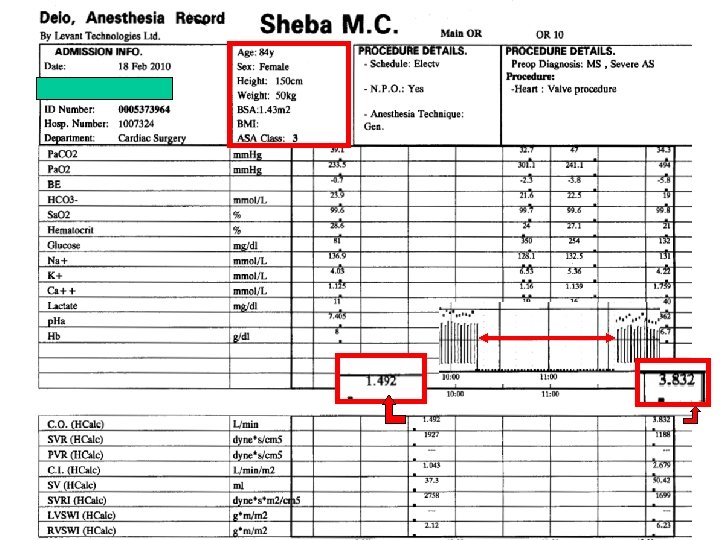
 “Will my patient respond to fluids? ” Yes. Give 1735 ml over 30 minutes. Will my patient respond to fluids?
“Will my patient respond to fluids? ” Yes. Give 1735 ml over 30 minutes. Will my patient respond to fluids?
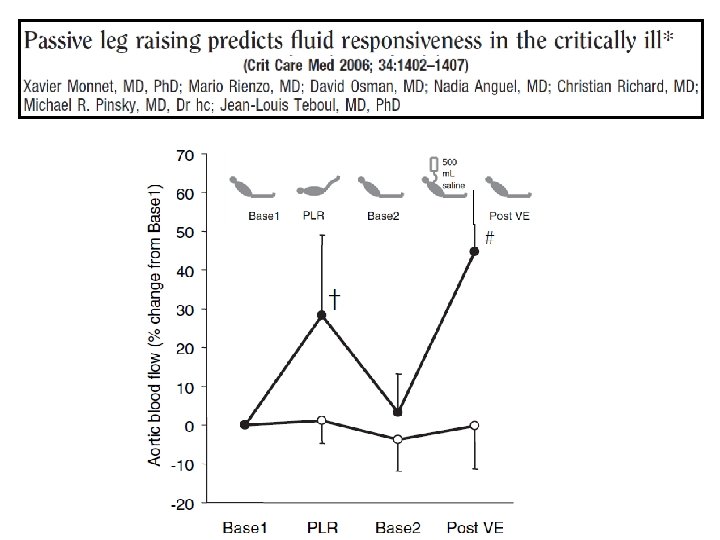
 Passive leg raising-induced changes in CO can reliably predict fluid responsiveness regardless of ventilation mode and cardiac rhythm. Passive leg raising-induced changes in CO have a significantly higher predictive value than passive leg raising-induced changes in arterial pulse pressure.
Passive leg raising-induced changes in CO can reliably predict fluid responsiveness regardless of ventilation mode and cardiac rhythm. Passive leg raising-induced changes in CO have a significantly higher predictive value than passive leg raising-induced changes in arterial pulse pressure.
 The hemodynamic response to a 15 second endexpiratory occlusion can predict volume responsiveness in mechanically ventilated patients.
The hemodynamic response to a 15 second endexpiratory occlusion can predict volume responsiveness in mechanically ventilated patients.
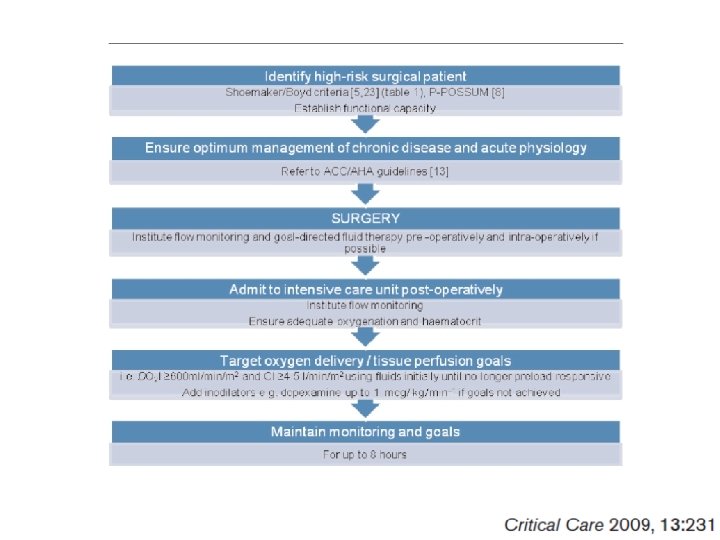
 The accumulation of evidence showing that increasing DO 2 in high-risk surgical patients may reduce morbidity and save lives has led Boyd and Bennett to claim that it may be considered unethical not to use goal-directed perioperative therapy once patient identification and the methods to be used in treating them are refined.
The accumulation of evidence showing that increasing DO 2 in high-risk surgical patients may reduce morbidity and save lives has led Boyd and Bennett to claim that it may be considered unethical not to use goal-directed perioperative therapy once patient identification and the methods to be used in treating them are refined.
 Unlike approaches that adopt a specific clinical practice, like liberal or restrictive fluid regimen, goal-directed approaches employ various monitoring techniques and interventions in order to achieve specific end-points for selected parameters. Ø Cardiac index (CI) Ø Stroke volume (SV) Ø Oxygen delivery (DO 2) Ø Mixed venous (Sv. O 2) or central venous (Scv. O 2) oxygen saturation Ø Lactate concentration Ø p. Hi
Unlike approaches that adopt a specific clinical practice, like liberal or restrictive fluid regimen, goal-directed approaches employ various monitoring techniques and interventions in order to achieve specific end-points for selected parameters. Ø Cardiac index (CI) Ø Stroke volume (SV) Ø Oxygen delivery (DO 2) Ø Mixed venous (Sv. O 2) or central venous (Scv. O 2) oxygen saturation Ø Lactate concentration Ø p. Hi
 Optimization – when and how? Ø A bolus of 200 ml colloid (e. g. , 6% HES 130/0. 4) is administered over 2 min, and 5 min later the SV is assessed. Ø The procedure is repeated if there was an increase in SV of >10%. When the fluid bolus does not result in a SV increment >10%, optimization is regarded as achieved and surgery commenced. Intermittent TD CO measurements have a well known intrinsic limited reproducibility which makes them inferior to continuously measured real-time CO in the process of perioperative optimization.
Optimization – when and how? Ø A bolus of 200 ml colloid (e. g. , 6% HES 130/0. 4) is administered over 2 min, and 5 min later the SV is assessed. Ø The procedure is repeated if there was an increase in SV of >10%. When the fluid bolus does not result in a SV increment >10%, optimization is regarded as achieved and surgery commenced. Intermittent TD CO measurements have a well known intrinsic limited reproducibility which makes them inferior to continuously measured real-time CO in the process of perioperative optimization.
 Optimization – when and how? Ø Transesophageal Doppler ultrasound v Patient needs to be anesthetized Ø The Vigileo system v Patient needs to have an arterial line Ø The Nexfin HD v Totally non-invasive
Optimization – when and how? Ø Transesophageal Doppler ultrasound v Patient needs to be anesthetized Ø The Vigileo system v Patient needs to have an arterial line Ø The Nexfin HD v Totally non-invasive
 NEXFIN
NEXFIN
 and oxygen transport goals (DO 2") Ø CO (CI > 4. 5 L/min/m 2) and oxygen transport goals (DO 2 I ≥ 600 ml/min/m 2) are important so direct flow monitoring should be implemented. Ø Fluids should be given to increase CO, and inodilators, such as dopexamine and dobutamine, added once the patient is no longer fluid (preload) responsive or not achieving the goals.
Ø CO (CI > 4. 5 L/min/m 2) and oxygen transport goals (DO 2 I ≥ 600 ml/min/m 2) are important so direct flow monitoring should be implemented. Ø Fluids should be given to increase CO, and inodilators, such as dopexamine and dobutamine, added once the patient is no longer fluid (preload) responsive or not achieving the goals.
 It is essential that the present individualized GDT approach includes optimization of flow-related parameters, such as cardiac stroke volume, within the limit of the individual patient’s cardiac capacity. The concept is therefore different from the original Shoemaker concept for optimization, which used predetermined supra-physiologic values of cardiac index and DO 2 as therapeutic goals.
It is essential that the present individualized GDT approach includes optimization of flow-related parameters, such as cardiac stroke volume, within the limit of the individual patient’s cardiac capacity. The concept is therefore different from the original Shoemaker concept for optimization, which used predetermined supra-physiologic values of cardiac index and DO 2 as therapeutic goals.
 The perioperative fluid management strategy determines the monitoring modality!
The perioperative fluid management strategy determines the monitoring modality!
 The Nexfin HDA truly noninvasive CCO monitor THANK YOU!
The Nexfin HDA truly noninvasive CCO monitor THANK YOU!

 Ø Blood volume after fasting is normal, and a fluidconsuming third space has never been reliably shown. Ø The endothelial glycocalyx plays a key role and is destroyed not only by ischemia and surgery, but also by acute hypervolemia. Ø Undifferentiated fluid handling may increase the shift toward the interstitial space, the consequence being a positive fluid balance and weight gain of up to 10 kg, which may be related to severe complications. Optimization ≠ Maximization
Ø Blood volume after fasting is normal, and a fluidconsuming third space has never been reliably shown. Ø The endothelial glycocalyx plays a key role and is destroyed not only by ischemia and surgery, but also by acute hypervolemia. Ø Undifferentiated fluid handling may increase the shift toward the interstitial space, the consequence being a positive fluid balance and weight gain of up to 10 kg, which may be related to severe complications. Optimization ≠ Maximization
 National Confidential Enquiry into Patient Outcome and Death. 1999 Report: Extremes of Age. http: //www. ncepod. org. uk National Confidential Enquiry into Perioperative Death have highlighted over-hydration as a contributory cause in the genesis of postoperative problems leading to death. Carefully considered case histories have led to specific recommendations regarding careful fluid management (the implication being restriction) in vulnerable patients and those most at risk, such as the elderly.
National Confidential Enquiry into Patient Outcome and Death. 1999 Report: Extremes of Age. http: //www. ncepod. org. uk National Confidential Enquiry into Perioperative Death have highlighted over-hydration as a contributory cause in the genesis of postoperative problems leading to death. Carefully considered case histories have led to specific recommendations regarding careful fluid management (the implication being restriction) in vulnerable patients and those most at risk, such as the elderly.
 A variety of metabolic endpoints are surrogate flow measurements, such as lactate, Sv. O 2, Scv. O 2, which may be useful during resuscitation, but CO (CI > 4. 5 L/min/m 2) and oxygen transport goals (DO 2 I ≥ 600 ml/min/m 2) are important so direct flow monitoring should be implemented. Fluids should be given to increase CO, and inodilators such as dopexamine and dobutamine added once the patient is no longer fluid (preload) responsive or not achieving the goals.
A variety of metabolic endpoints are surrogate flow measurements, such as lactate, Sv. O 2, Scv. O 2, which may be useful during resuscitation, but CO (CI > 4. 5 L/min/m 2) and oxygen transport goals (DO 2 I ≥ 600 ml/min/m 2) are important so direct flow monitoring should be implemented. Fluids should be given to increase CO, and inodilators such as dopexamine and dobutamine added once the patient is no longer fluid (preload) responsive or not achieving the goals.
 A variety of metabolic endpoints are surrogate flow measurements, such as lactate, Sv. O 2, Scv. O 2, which may be useful during resuscitation, but CO (CI > 4. 5 L/min/m 2) and oxygen transport goals (DO 2 I ≥ 600 ml/min/m 2) are important so direct flow monitoring should be implemented. Fluids should be given to increase CO, and inodilators such as dopexamine and dobutamine added once the patient is no longer fluid (preload) responsive or not achieving the goals.
A variety of metabolic endpoints are surrogate flow measurements, such as lactate, Sv. O 2, Scv. O 2, which may be useful during resuscitation, but CO (CI > 4. 5 L/min/m 2) and oxygen transport goals (DO 2 I ≥ 600 ml/min/m 2) are important so direct flow monitoring should be implemented. Fluids should be given to increase CO, and inodilators such as dopexamine and dobutamine added once the patient is no longer fluid (preload) responsive or not achieving the goals.
 This systematic review demonstrated a very poor relationship between CVP and blood volume as well as the inability of CVP / ΔCVP to predict the hemodynamic response to a fluid challenge. CVP should not be used to make clinical decisions regarding fluid management.
This systematic review demonstrated a very poor relationship between CVP and blood volume as well as the inability of CVP / ΔCVP to predict the hemodynamic response to a fluid challenge. CVP should not be used to make clinical decisions regarding fluid management.
 Overall, only 56 ± 16% of 803 patients that were included in the 24 studies responded to a fluid challenge.
Overall, only 56 ± 16% of 803 patients that were included in the 24 studies responded to a fluid challenge.
 Perioperative fluid optimization necessitates real-time CCO Intermittent TD CO measurements have a well known intrinsic limited reproducibility. This limitation makes them inferior to continuously measured real-time CO in assessing the response to therapeutic or diagnostic events with short time constants. Ø Fluid loading (e. g. , periop. optimization) Ø Passive leg raising, end-exp. occlusion. Ø Immediate response to inotropes
Perioperative fluid optimization necessitates real-time CCO Intermittent TD CO measurements have a well known intrinsic limited reproducibility. This limitation makes them inferior to continuously measured real-time CO in assessing the response to therapeutic or diagnostic events with short time constants. Ø Fluid loading (e. g. , periop. optimization) Ø Passive leg raising, end-exp. occlusion. Ø Immediate response to inotropes
 Ø Transesophageal Doppler ultrasound v Patient needs to be anesthetized Ø The Vigileo system v Patient needs to have an arterial line Ø The Nexfin HD v Totally non-invasive
Ø Transesophageal Doppler ultrasound v Patient needs to be anesthetized Ø The Vigileo system v Patient needs to have an arterial line Ø The Nexfin HD v Totally non-invasive
 Limitations 1. Duration of measurement is restricted to 8 hours 2. Peripheral vasoconstriction (age, cold, vasopressors) 3. Edematous fingers 4. Currently no PPV / SVV 5. GUI more suitable for a cardiology clinic
Limitations 1. Duration of measurement is restricted to 8 hours 2. Peripheral vasoconstriction (age, cold, vasopressors) 3. Edematous fingers 4. Currently no PPV / SVV 5. GUI more suitable for a cardiology clinic
 Limitations 1. Duration of measurement is restricted to 8 hours 2. Peripheral vasoconstriction (age, cold, vasopressors) 3. Edematous fingers 4. Currently no PPV / SVV 5. GUI more suitable for a cardiology clinic Additional benefits 1. Semi-disposable finger cuff 2. Touch screen 3. Instant data retrieval with DOK
Limitations 1. Duration of measurement is restricted to 8 hours 2. Peripheral vasoconstriction (age, cold, vasopressors) 3. Edematous fingers 4. Currently no PPV / SVV 5. GUI more suitable for a cardiology clinic Additional benefits 1. Semi-disposable finger cuff 2. Touch screen 3. Instant data retrieval with DOK
 Prediction of volume responsiveness by using passive leg raising Boulain T, et al. Chest 2002; 121: 1245– 52 Monnet X, et al. Crit Care Med 2006; 34: 1402 -7 Lafanechere A, et al. Crit Care 2006; 10: R 132 Lamia B, et al. Intensive Care Med 2007; 33: 1125– 32 Maizel J, et al. Intensive Care Med 2007; 33: 1133– 8 Caille V, et al. Intensive Care Med 2008; 34: 1239– 45 Thiel SW, et al. Crit Care 2009; 13: R 111 Biais M, et al. Crit Care 2009, 13: R 195
Prediction of volume responsiveness by using passive leg raising Boulain T, et al. Chest 2002; 121: 1245– 52 Monnet X, et al. Crit Care Med 2006; 34: 1402 -7 Lafanechere A, et al. Crit Care 2006; 10: R 132 Lamia B, et al. Intensive Care Med 2007; 33: 1125– 32 Maizel J, et al. Intensive Care Med 2007; 33: 1133– 8 Caille V, et al. Intensive Care Med 2008; 34: 1239– 45 Thiel SW, et al. Crit Care 2009; 13: R 111 Biais M, et al. Crit Care 2009, 13: R 195
 Changes in stroke volume, radial pulse pressure, and peak velocity of femoral artery flow induced by passive leg raising are accurate and interchangeable indices for predicting fluid responsiveness in nonintubated patients with severe sepsis or acute pancreatitis.
Changes in stroke volume, radial pulse pressure, and peak velocity of femoral artery flow induced by passive leg raising are accurate and interchangeable indices for predicting fluid responsiveness in nonintubated patients with severe sepsis or acute pancreatitis.
 13 patients were studied within 2 h of arrival in the ICU following CABG or mitral valve reconstruction. Cardiac output (CO) was evaluated using the Flo. Trac (COed), the modified Modelflow (COmf ), and the ultrasound Hemo. Sonic system (COhs), and compared with thermodilution (COtd) as the reference (triplicate, automated system under computer control, equally spread measurements over the ventilatory cycle). 104 paired CO values were assessed before, during and after four interventions: (i) an increase of tidal volume by 50%; (ii) a 10 cm H 2 O increase in PEEP; (iii) passive leg raising; (iv) head up position.
13 patients were studied within 2 h of arrival in the ICU following CABG or mitral valve reconstruction. Cardiac output (CO) was evaluated using the Flo. Trac (COed), the modified Modelflow (COmf ), and the ultrasound Hemo. Sonic system (COhs), and compared with thermodilution (COtd) as the reference (triplicate, automated system under computer control, equally spread measurements over the ventilatory cycle). 104 paired CO values were assessed before, during and after four interventions: (i) an increase of tidal volume by 50%; (ii) a 10 cm H 2 O increase in PEEP; (iii) passive leg raising; (iv) head up position.
 and smallest range of the limits of") COmf has best precision (0. 69 l/min) and smallest range of the limits of agreement (-1. 08– 1. 68 l/min), 26%, compared with the COed and COhs ( -1. 47– 2. 13), 34%, and (-2. 62– 1. 80 l/min), 44%, respectively. Flo. Trac–Vigileo (COed) Modified Modelflow method (COmf) Hemo. Sonic 100 ultrasound system (COhs)
COmf has best precision (0. 69 l/min) and smallest range of the limits of agreement (-1. 08– 1. 68 l/min), 26%, compared with the COed and COhs ( -1. 47– 2. 13), 34%, and (-2. 62– 1. 80 l/min), 44%, respectively. Flo. Trac–Vigileo (COed) Modified Modelflow method (COmf) Hemo. Sonic 100 ultrasound system (COhs)
") Our main finding is that only he modified Modelflow yields limits of agreement (26%) that are below the 30% criteria for a theoretically acceptable alternative to thermodilution cardiac output. Monitoring changes or trends in cardiac output can be performed reasonably well with the Modelflow and the Hemo. Sonic, while the Flo. Trac performs less well in this regard. Encouraged by the simplicity of setup procedure and advantage for the patient, we suggest future work focuses on the Modelflow system.
Our main finding is that only he modified Modelflow yields limits of agreement (26%) that are below the 30% criteria for a theoretically acceptable alternative to thermodilution cardiac output. Monitoring changes or trends in cardiac output can be performed reasonably well with the Modelflow and the Hemo. Sonic, while the Flo. Trac performs less well in this regard. Encouraged by the simplicity of setup procedure and advantage for the patient, we suggest future work focuses on the Modelflow system.