

d27f33c30823eef5341665e255198982.ppt
- Количество слайдов: 41
 The Eradication of VAP in Scotland Martin Hughes Nov 2010
The Eradication of VAP in Scotland Martin Hughes Nov 2010
 Plan • • Definition Diagnosis Importance Strategies to reduce VAP Why don’t they work? What does work? Eradication in Scotland
Plan • • Definition Diagnosis Importance Strategies to reduce VAP Why don’t they work? What does work? Eradication in Scotland
 Definition • Inflammation of lung parenchyma > 48 hours post intubation, due to organisms not present or incubating at the time mechanical ventilation was commenced. • Early onset within first 4 days: usually due to antibiotic sensitive • Late onset > 5 days: commonly multi-drug resistant pathogens.
Definition • Inflammation of lung parenchyma > 48 hours post intubation, due to organisms not present or incubating at the time mechanical ventilation was commenced. • Early onset within first 4 days: usually due to antibiotic sensitive • Late onset > 5 days: commonly multi-drug resistant pathogens.
 Pathophysiology • Aspiration of pathogenic organisms from the oropharynx. • Normal flora replaced by pathogenic organisms (S. aureus, P. aeruginosa, H. influenzae, and Enterobacteriaceae (e. g. E. coli, Proteus, Enterobacter, Klebsiella, Serratia) • This change directly related to the severity of illness • Mixed infection in 50% • ‘Endotracheal tube associated pneumonia’
Pathophysiology • Aspiration of pathogenic organisms from the oropharynx. • Normal flora replaced by pathogenic organisms (S. aureus, P. aeruginosa, H. influenzae, and Enterobacteriaceae (e. g. E. coli, Proteus, Enterobacter, Klebsiella, Serratia) • This change directly related to the severity of illness • Mixed infection in 50% • ‘Endotracheal tube associated pneumonia’
 Temperature Leucocyte (cells/µL) Pa. O") Diagnosis • • • Clinical Pulmonary Infection Score (CPIS) Temperature Leucocyte (cells/µL) Pa. O 2/Fi. O 2 (mm. Hg) CXR Tracheal secretions Culture 89% sensitive; 47% specific Rx CPIS > 6, stop if < 6 at day 3.
Diagnosis • • • Clinical Pulmonary Infection Score (CPIS) Temperature Leucocyte (cells/µL) Pa. O 2/Fi. O 2 (mm. Hg) CXR Tracheal secretions Culture 89% sensitive; 47% specific Rx CPIS > 6, stop if < 6 at day 3.
 Diagnosis • BAL, PSB, PCS • BAL cultures have a high sensitivity and specificity, resulting in a high positive predictive value. • 104 CFU/m. L is usual threshold for BAL cultures. • More expensive • Complications • Less Antibiotics?
Diagnosis • BAL, PSB, PCS • BAL cultures have a high sensitivity and specificity, resulting in a high positive predictive value. • 104 CFU/m. L is usual threshold for BAL cultures. • More expensive • Complications • Less Antibiotics?
 Diagnosis • No gold standard • A Randomized Trial of Diagnostic Techniques for Ventilator-Associated Pneumonia. The Canadian Critical Care Trials Group. N Engl J Med 2006; 355: 2619 -2630, 2006 • No difference in mortality or antibiotic use • Excluded known MRSA/pseudomonas
Diagnosis • No gold standard • A Randomized Trial of Diagnostic Techniques for Ventilator-Associated Pneumonia. The Canadian Critical Care Trials Group. N Engl J Med 2006; 355: 2619 -2630, 2006 • No difference in mortality or antibiotic use • Excluded known MRSA/pseudomonas
 Importance • Incidence 9 – 28% • Risk per day: 3% day 5, 2% day 10, 1% day 15 • Prolonged ventilation and ICU stay • 50% antibiotics in ICU for respiratory infections • Attributable mortality debated • Common sense?
Importance • Incidence 9 – 28% • Risk per day: 3% day 5, 2% day 10, 1% day 15 • Prolonged ventilation and ICU stay • 50% antibiotics in ICU for respiratory infections • Attributable mortality debated • Common sense?
, 90 pts,") Strategies to reduce VAP • Elevation of bed • One study (1+), 90 pts, 1999. NNT of 4 -5 to prevent one VAP • Daily sedation break • One study (1+), 150 pts, 2000. 2. 4 vent days, 3. 5 ICU days saved • More recently – sedation break + weaning assessment. http: //www. sicsebm. org. uk
Strategies to reduce VAP • Elevation of bed • One study (1+), 90 pts, 1999. NNT of 4 -5 to prevent one VAP • Daily sedation break • One study (1+), 150 pts, 2000. 2. 4 vent days, 3. 5 ICU days saved • More recently – sedation break + weaning assessment. http: //www. sicsebm. org. uk
 Evidence • Sub-glottic ETT: • One review, 4 studies, Grade A recommendation, NNT 12 to prevent one VAP • Chlorhexidine oral care: • One meta- analysis. NNT 14 to prevent one VAP.
Evidence • Sub-glottic ETT: • One review, 4 studies, Grade A recommendation, NNT 12 to prevent one VAP • Chlorhexidine oral care: • One meta- analysis. NNT 14 to prevent one VAP.
") Evidence • Weaning trial: – In combination with sedation holiday – One study (1+) 336 patients. Daily sedation holiday and weaning trial. • NNT Death (1 yr) 7 • Reduced ICU & hospital stay
Evidence • Weaning trial: – In combination with sedation holiday – One study (1+) 336 patients. Daily sedation holiday and weaning trial. • NNT Death (1 yr) 7 • Reduced ICU & hospital stay
 Others • NIV – avoiding intubation • Kinetic beds – no evidence • HME vs Heated Water Humidification – equally effective • SDD?
Others • NIV – avoiding intubation • Kinetic beds – no evidence • HME vs Heated Water Humidification – equally effective • SDD?
 Bundles • Structured way of improving the processes of care and patient outcomes • Small, straightforward set of evidence-based practices • Three to five in set - when performed collectively and reliably, have been proven to improve patient outcomes
Bundles • Structured way of improving the processes of care and patient outcomes • Small, straightforward set of evidence-based practices • Three to five in set - when performed collectively and reliably, have been proven to improve patient outcomes
 Bundles • • • Every patient, every time. ‘All necessary and all sufficient’ Level 1 evidence All-or-nothing measurement of elements At a specific place and time Success means the whole bundle
Bundles • • • Every patient, every time. ‘All necessary and all sufficient’ Level 1 evidence All-or-nothing measurement of elements At a specific place and time Success means the whole bundle
 Timely: reduce waits and delays for those who receive and give care Effective: evidence based and applied to all who could benefit Safe: safety is a system property Efficient: avoid waste Quality In ICU Equitable: care does not vary in quality Patient Centered: care that is respectful and responsive to individual patient preferences and needs
Timely: reduce waits and delays for those who receive and give care Effective: evidence based and applied to all who could benefit Safe: safety is a system property Efficient: avoid waste Quality In ICU Equitable: care does not vary in quality Patient Centered: care that is respectful and responsive to individual patient preferences and needs
 SRI Experience – Nov 2005 • VAP Prevention Bundle • 30 - 45 o positioning • daily sedation holiday • daily weaning assessment • chlorhexidine mouthwash • subglottic aspiration tube • tubing management – appropriate humidification – avoidance of contamination
SRI Experience – Nov 2005 • VAP Prevention Bundle • 30 - 45 o positioning • daily sedation holiday • daily weaning assessment • chlorhexidine mouthwash • subglottic aspiration tube • tubing management – appropriate humidification – avoidance of contamination
 Additionally • S/C enoxaparin pre-printed • Ranitidine pre-printed • Enteral feeding encouraged – if tolerated ranitidine cessation considered.
Additionally • S/C enoxaparin pre-printed • Ranitidine pre-printed • Enteral feeding encouraged – if tolerated ranitidine cessation considered.
 SRI experience • At launch – Consultant buy in – Laminated charts by every bed space – Unit posters – Surveillance programme (Helics) – Ahead of the game nationally
SRI experience • At launch – Consultant buy in – Laminated charts by every bed space – Unit posters – Surveillance programme (Helics) – Ahead of the game nationally
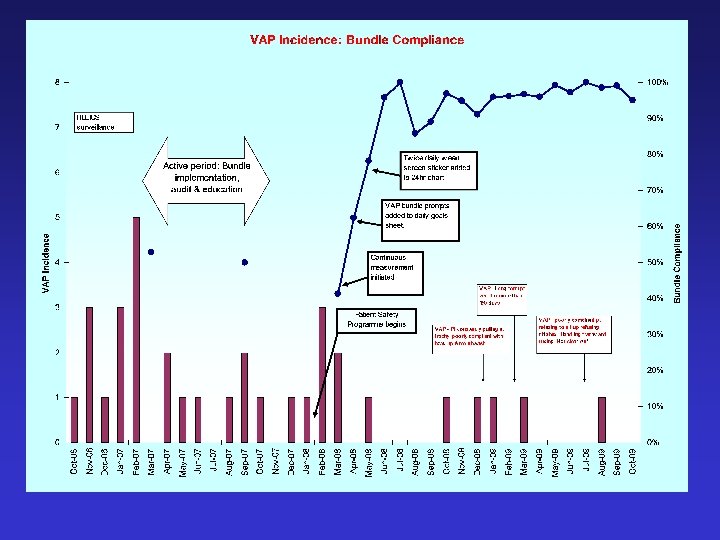
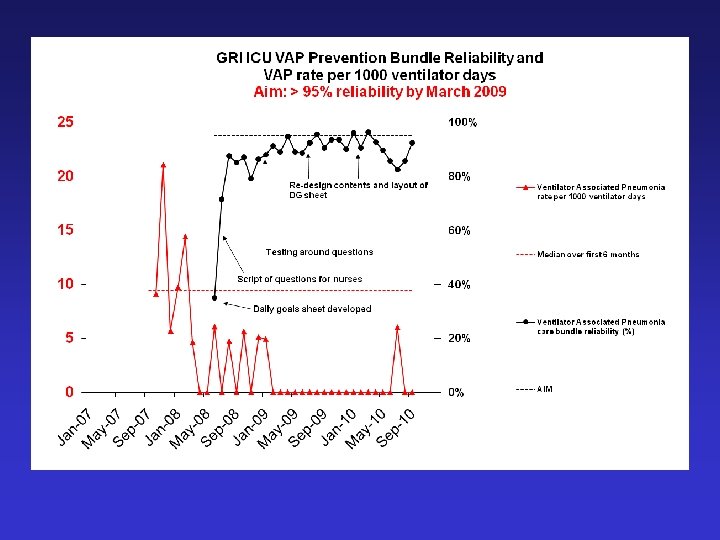
 Job done? • What is the VAP rate? • What is the bundle compliance? • Hawe, Ellis, Cairns, Longmate ICM, 2009
Job done? • What is the VAP rate? • What is the bundle compliance? • Hawe, Ellis, Cairns, Longmate ICM, 2009
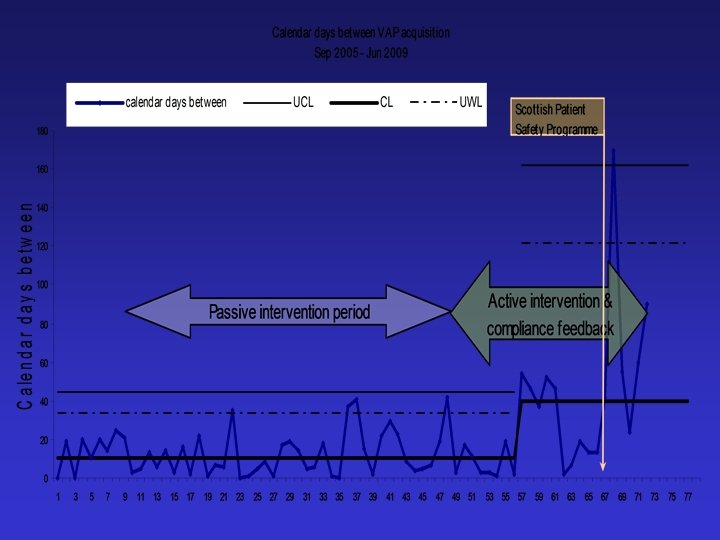
 Upper warning line Centreline (mean)") G chart Upper control limit (3 SDs) Upper warning line Centreline (mean)
G chart Upper control limit (3 SDs) Upper warning line Centreline (mean)
 * Patient at 30 -45 Chi-squared p") Process Postinterventions FV VAP Bundle (*SICS Bundle) * Patient at 30 -45 Chi-squared p value (Nov 2006 vs Oct 2007) Nov 2006 May 2007 Oct 2007 54% 80% 94% <0. 001 Subglottic ETDT 72% 92% <0. 001 * Oral chlorhex 8% 94% 100% <0. 001 Tubing/HMEF 98% 100% 0. 31 * Daily weaning plan * Sedation stop 52% 72% 0. 039 72% 86% 82% 0. 23 All elements 0% 48% 54% <0. 0001 o o
Process Postinterventions FV VAP Bundle (*SICS Bundle) * Patient at 30 -45 Chi-squared p value (Nov 2006 vs Oct 2007) Nov 2006 May 2007 Oct 2007 54% 80% 94% <0. 001 Subglottic ETDT 72% 92% <0. 001 * Oral chlorhex 8% 94% 100% <0. 001 Tubing/HMEF 98% 100% 0. 31 * Daily weaning plan * Sedation stop 52% 72% 0. 039 72% 86% 82% 0. 23 All elements 0% 48% 54% <0. 0001 o o
 Problem? • Passive interventions don’t work • Educational interventions to reduce VAP • Structure, Process, Outcome
Problem? • Passive interventions don’t work • Educational interventions to reduce VAP • Structure, Process, Outcome
 Active Implementation • Education: workshops: definition, epidemiology, pathogenesis, risk factors, consequences of VAP, evidence-base for the bundle. • Written material distributed. • Over 90% of the unit’s medical and nursing staff by April 2007. • Repeat cycles of process and outcome measurement and feedback.
Active Implementation • Education: workshops: definition, epidemiology, pathogenesis, risk factors, consequences of VAP, evidence-base for the bundle. • Written material distributed. • Over 90% of the unit’s medical and nursing staff by April 2007. • Repeat cycles of process and outcome measurement and feedback.
 * Patient at 30 -45") Sequential Process Measurements Baseline FV VAP Bundle (*SICS Bundle) * Patient at 30 -45 Postinterventions Chi-squared p value (Nov 2006 vs Oct 2007) Nov 2006 May 2007 Oct 2007 54% 80% 94% <0. 001 Subglottic ETDT 72% 92% <0. 001 * Oral chlorhex 8% 94% 100% <0. 001 Tubing/HMEF 98% 100% 0. 31 * Daily weaning plan * Sedation stop 52% 72% 0. 039 72% 86% 82% 0. 23 All elements 0% 48% 54% <0. 0001 o o
Sequential Process Measurements Baseline FV VAP Bundle (*SICS Bundle) * Patient at 30 -45 Postinterventions Chi-squared p value (Nov 2006 vs Oct 2007) Nov 2006 May 2007 Oct 2007 54% 80% 94% <0. 001 Subglottic ETDT 72% 92% <0. 001 * Oral chlorhex 8% 94% 100% <0. 001 Tubing/HMEF 98% 100% 0. 31 * Daily weaning plan * Sedation stop 52% 72% 0. 039 72% 86% 82% 0. 23 All elements 0% 48% 54% <0. 0001 o o
 Study Period
Study Period
 Passive Sept 2005 - Feb 2007 patients ventilated for > 48 hrs Active March – Dec 2007 374 215 2556 1327 episodes of VAP 49 10 VAP/1000 vent days 19. 17 7. 5 4. 5 5. 0 (112/374) 30% (49/215) 23% Vent days Median LOS Mortality rd=11. 6 99% CI 2. 3 -21. 0 rr=0. 39 99% CI 0. 16, 0. 96) p=0. 06
Passive Sept 2005 - Feb 2007 patients ventilated for > 48 hrs Active March – Dec 2007 374 215 2556 1327 episodes of VAP 49 10 VAP/1000 vent days 19. 17 7. 5 4. 5 5. 0 (112/374) 30% (49/215) 23% Vent days Median LOS Mortality rd=11. 6 99% CI 2. 3 -21. 0 rr=0. 39 99% CI 0. 16, 0. 96) p=0. 06
 Lessons • Passive implementation of the VAP prevention bundle failed. • Compliance improved during an active multimodal implementation. • This was associated with a significant reduction in the occurrence of VAP.
Lessons • Passive implementation of the VAP prevention bundle failed. • Compliance improved during an active multimodal implementation. • This was associated with a significant reduction in the occurrence of VAP.
 Since then………………. . The Scottish Patient Safety Programme
Since then………………. . The Scottish Patient Safety Programme
 VAP Prevention Bundle Sedation reviewed and stopped if appropriate Y N Exclusion Patient assessed for weaning and extubation Y N Exclusion Supine position avoided Y N Exclusion Chlorhexidine 1 -2% QID Y N Exclusion Use of subglottic drainage ETT Y N Exclusion
VAP Prevention Bundle Sedation reviewed and stopped if appropriate Y N Exclusion Patient assessed for weaning and extubation Y N Exclusion Supine position avoided Y N Exclusion Chlorhexidine 1 -2% QID Y N Exclusion Use of subglottic drainage ETT Y N Exclusion
 Post spsp improvements
Post spsp improvements
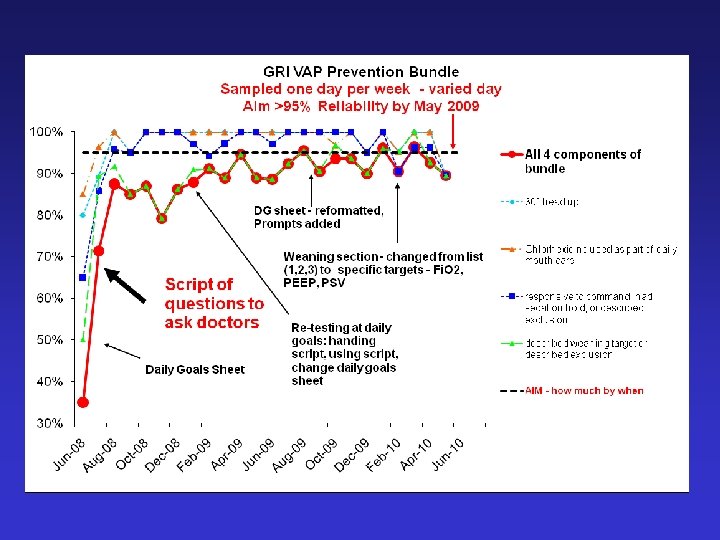
 VAP – Key points • Evidence is the starting point • Implementation is difficult – efficacy vs effectiveness • Process measure identifies failings • SPSP methodology leads to sustained process improvement
VAP – Key points • Evidence is the starting point • Implementation is difficult – efficacy vs effectiveness • Process measure identifies failings • SPSP methodology leads to sustained process improvement
 VAP – key points • • • Education Feedback Process measurement / management You need the correct clinicians The result is outcome improvement Resources – without the above, bundles are “futile”
VAP – key points • • • Education Feedback Process measurement / management You need the correct clinicians The result is outcome improvement Resources – without the above, bundles are “futile”
 VAP - eliminated • VAP still here • So rare that we can now discuss the reasons for individual cases • Huge reduction in the problem • Scottish ICU clinicians and SPSP/IHI • Effective healthcare does not need to cost more
VAP - eliminated • VAP still here • So rare that we can now discuss the reasons for individual cases • Huge reduction in the problem • Scottish ICU clinicians and SPSP/IHI • Effective healthcare does not need to cost more