

efa44c069675fdf57bf36cc59553334c.ppt
- Количество слайдов: 77
 The Endocrine System
The Endocrine System
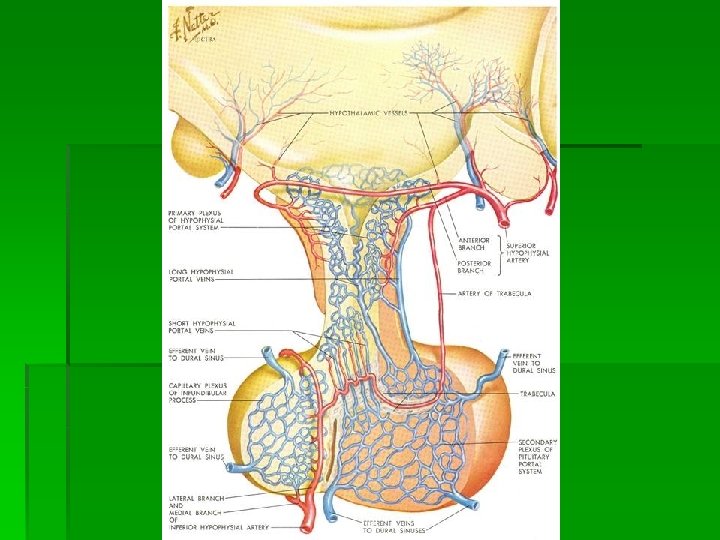
 Hypophyseal-Pituitary Axis § § § Site of Neural – Hormonal interaction Sets temporal release of hormones Responsible for stress reaction of hormones
Hypophyseal-Pituitary Axis § § § Site of Neural – Hormonal interaction Sets temporal release of hormones Responsible for stress reaction of hormones
 The Hypothalamus & the Pituitary Gland-- Master Endocrine Glands! The Hypothalamus: § Located in the brain, this region controls most endocrine secretions § Mainly regulatory hormones are released here. Most control the pituitary gland The Pituitary Gland § Descending from the hypothalamus, this gland has two halves: anterior & posterior § The anterior half secretes mainly regulatory hormones § The posterior half secretes hormones, but manufactures none
The Hypothalamus & the Pituitary Gland-- Master Endocrine Glands! The Hypothalamus: § Located in the brain, this region controls most endocrine secretions § Mainly regulatory hormones are released here. Most control the pituitary gland The Pituitary Gland § Descending from the hypothalamus, this gland has two halves: anterior & posterior § The anterior half secretes mainly regulatory hormones § The posterior half secretes hormones, but manufactures none
 SS (somatostatin,") Hormones secreted by the Hypothalamus & Anterior Pituitary Gland Hypothalamus GHRH (GH-releasing) SS (somatostatin, GH-inhib) CRH (corticotropin-rel) Gn. RH (gonadotropin-rel) hormone) “ PRH (PRL-releasing) PIH (PRL rel-inhibiting) Anterior Pituitary GH (growth hormone) “ ACTH (adrenocorticotropic) LH (luteinizing FSH (follicle-stimulating) PRL (prolactin) “
Hormones secreted by the Hypothalamus & Anterior Pituitary Gland Hypothalamus GHRH (GH-releasing) SS (somatostatin, GH-inhib) CRH (corticotropin-rel) Gn. RH (gonadotropin-rel) hormone) “ PRH (PRL-releasing) PIH (PRL rel-inhibiting) Anterior Pituitary GH (growth hormone) “ ACTH (adrenocorticotropic) LH (luteinizing FSH (follicle-stimulating) PRL (prolactin) “
 What do these anterior pituitary hormones do? Growth Hormone: § stimulates cells to grow and divide § increases amino acid transport rate and protein synthesis § increases fat metabolism Typically, GH is secreted during sleep. GH secretion increases when malnourished GH influences bone growth via somatomedin: GH in blood GH arrives in liver secretes somatomedin cartilage divides bones grow!
What do these anterior pituitary hormones do? Growth Hormone: § stimulates cells to grow and divide § increases amino acid transport rate and protein synthesis § increases fat metabolism Typically, GH is secreted during sleep. GH secretion increases when malnourished GH influences bone growth via somatomedin: GH in blood GH arrives in liver secretes somatomedin cartilage divides bones grow!
 Problems with GH § Too much GH in children leads to gigantism § Too much GH in adults leads to acromegaly § Too little GH in children leads to dwarfism
Problems with GH § Too much GH in children leads to gigantism § Too much GH in adults leads to acromegaly § Too little GH in children leads to dwarfism
 Other Anterior Pituitary Hormone Functions ACTH: LH & FSH: § works on the cortex of the adrenal gland, influencing the release of cortisol § stress can increase CRH secretion which will increase ACTH secretion § negative feedback when adrenal cortex hormones in blood decrease CRH § LH in females and in males leads to sex hormone secretion § FSH in females causes growth and development of egg cellcontaining follicles in the ovary, and causes estrogen secretion § FSH in males instigates sperm production § both hormones are regulated by Gn. RH, which is not significant in concentration
Other Anterior Pituitary Hormone Functions ACTH: LH & FSH: § works on the cortex of the adrenal gland, influencing the release of cortisol § stress can increase CRH secretion which will increase ACTH secretion § negative feedback when adrenal cortex hormones in blood decrease CRH § LH in females and in males leads to sex hormone secretion § FSH in females causes growth and development of egg cellcontaining follicles in the ovary, and causes estrogen secretion § FSH in males instigates sperm production § both hormones are regulated by Gn. RH, which is not significant in concentration
 More Anterior Pituitary Hormone Functions PRL: TSH: § In females, PRL § promotes lactation § In males, PRL decreases LH secretion (note that § too much PRL would then decrease androgen levels and cause sterility) § § Controlled by both PRH and PIH § works on thyroid gland to either cause or inhibit its secretion of hormones works on thyroid gland to affect its growth (too much TSH leads to a goiter) negative feedback via thyroid hormones in blood stress or cold temperatures can change TSH secretion
More Anterior Pituitary Hormone Functions PRL: TSH: § In females, PRL § promotes lactation § In males, PRL decreases LH secretion (note that § too much PRL would then decrease androgen levels and cause sterility) § § Controlled by both PRH and PIH § works on thyroid gland to either cause or inhibit its secretion of hormones works on thyroid gland to affect its growth (too much TSH leads to a goiter) negative feedback via thyroid hormones in blood stress or cold temperatures can change TSH secretion
 The Posterior Pituitary Lobe No hormones are made here. They are made in the hypothalamus and just released here. Two peptide hormones are released from the posterior pituitary lobe (the neurohypophysis): § ADH (antidiuretic hormone or
The Posterior Pituitary Lobe No hormones are made here. They are made in the hypothalamus and just released here. Two peptide hormones are released from the posterior pituitary lobe (the neurohypophysis): § ADH (antidiuretic hormone or
 Function of Posterior Pituitary Lobe Hormones ADH: OT: § as an “antidiuretic, ” ADH decreases urine formation by having kidneys conserve water § also can contract smooth muscle cells, as found in blood vessels-- this causes an increase in blood pressure § ADH release triggered by osmoreceptors and inhibited by stretch receptors in blood § In females, contracts the uterine wall smooth muscles § In females, helps to eject milk when lactating § No known function in males, although in both males and females, OT can have some antidiuretic effects
Function of Posterior Pituitary Lobe Hormones ADH: OT: § as an “antidiuretic, ” ADH decreases urine formation by having kidneys conserve water § also can contract smooth muscle cells, as found in blood vessels-- this causes an increase in blood pressure § ADH release triggered by osmoreceptors and inhibited by stretch receptors in blood § In females, contracts the uterine wall smooth muscles § In females, helps to eject milk when lactating § No known function in males, although in both males and females, OT can have some antidiuretic effects
 SS (somatostatin, GH-inhib) CRH (corticotropin-rel) Gn. RH") Hypothalamus & Anterior Pituitary Hypothalamus GHRH (GH-releasing) SS (somatostatin, GH-inhib) CRH (corticotropin-rel) Gn. RH (gonadotropin-rel) Anterior Pituitary GH (growth hormone) “ ACTH (adrenocorticotropic) LH (luteinizing hormone) “ PRH (PRL-releasing) PIH (PRL rel-inhibiting) FSH (follicle-stimulating) PRL (prolactin) “
Hypothalamus & Anterior Pituitary Hypothalamus GHRH (GH-releasing) SS (somatostatin, GH-inhib) CRH (corticotropin-rel) Gn. RH (gonadotropin-rel) Anterior Pituitary GH (growth hormone) “ ACTH (adrenocorticotropic) LH (luteinizing hormone) “ PRH (PRL-releasing) PIH (PRL rel-inhibiting) FSH (follicle-stimulating) PRL (prolactin) “
 Your book’s review diagram:
Your book’s review diagram:
 HPA Basics § Hypophysis § Third Ventricle § GRH, TRH, CRH, Gn. RH, Dopamine, Somatostatin § Neurohypophysis § Derived from Hypophysis § ADH, Oxytocin § Adenohypophysis § Derived from Rathke’s pouch § ACTH, LH, FSH, TSH, GH, PRL
HPA Basics § Hypophysis § Third Ventricle § GRH, TRH, CRH, Gn. RH, Dopamine, Somatostatin § Neurohypophysis § Derived from Hypophysis § ADH, Oxytocin § Adenohypophysis § Derived from Rathke’s pouch § ACTH, LH, FSH, TSH, GH, PRL
 Pituitary Diseases § Primary Tumors § § Metastasis Empty Sella § § Sheehand’s syndrome Hyperfunction § § Surgical, post-Sheehand’s Hemorrhage § § Adenomas Craniopharyngioma Prolactin Insufficiency
Pituitary Diseases § Primary Tumors § § Metastasis Empty Sella § § Sheehand’s syndrome Hyperfunction § § Surgical, post-Sheehand’s Hemorrhage § § Adenomas Craniopharyngioma Prolactin Insufficiency
 The Endocrine Glands and Their Hormones § Pituitary Gland § A marble-sized gland at the base of the brain § Controlled by the hypothalamus or other neural mechanisms and therefore the middle man. § Posterior Lobe § Antidiuretic hormone: responsible for fluid retention § Oxytocin: contraction of the uterus
The Endocrine Glands and Their Hormones § Pituitary Gland § A marble-sized gland at the base of the brain § Controlled by the hypothalamus or other neural mechanisms and therefore the middle man. § Posterior Lobe § Antidiuretic hormone: responsible for fluid retention § Oxytocin: contraction of the uterus
 The Endocrine Glands and their Hormones § Pituitary Gland § Exercise appears to be a strong stimulant to the hypothalamus for the release of all anterior pituitary hormones § Anterior Lobe § Adrenocorticotropin § Growth hormone * § Thyropin § Follicle-stimulating hormone § Luteinizing hormone * § Prolactin
The Endocrine Glands and their Hormones § Pituitary Gland § Exercise appears to be a strong stimulant to the hypothalamus for the release of all anterior pituitary hormones § Anterior Lobe § Adrenocorticotropin § Growth hormone * § Thyropin § Follicle-stimulating hormone § Luteinizing hormone * § Prolactin
 The Endocrine Glands and Their Hormones § Thyroid Gland § Located along the midline of the neck § Secretes two nonsteroid hormones § Triiodothyronine (T 3) § Thyroxine (T 4) § Regulates metabolism § increases protein synthesis § promotes glycolysis, gluconeogenesis, glucose uptake § Calcitonin: calcium metabolism
The Endocrine Glands and Their Hormones § Thyroid Gland § Located along the midline of the neck § Secretes two nonsteroid hormones § Triiodothyronine (T 3) § Thyroxine (T 4) § Regulates metabolism § increases protein synthesis § promotes glycolysis, gluconeogenesis, glucose uptake § Calcitonin: calcium metabolism
 Thyroid
Thyroid
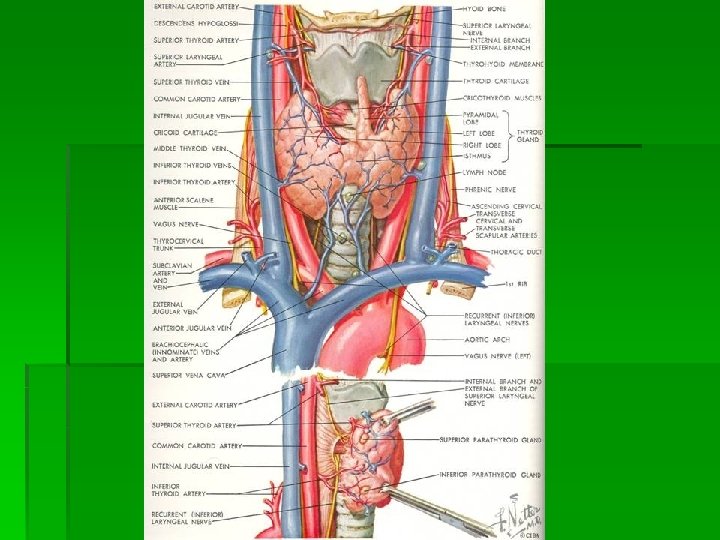
 Thyroid § Largest Endocrine organ in the body § Involved in production, storage, and release of thyroid hormone § Function influenced by § § Central axis (TRH) Pituitary function (TSH) Comorbid diseases (Cirrhosis, Graves, etc. ) Environmental factors (iodine intake)
Thyroid § Largest Endocrine organ in the body § Involved in production, storage, and release of thyroid hormone § Function influenced by § § Central axis (TRH) Pituitary function (TSH) Comorbid diseases (Cirrhosis, Graves, etc. ) Environmental factors (iodine intake)
 The Thyroid Gland Structure: This bilobed gland contains many follicles. A follicle is a group of cells encircling a lumen. The lumen contains material called colloid (a glycoprotein) within it. As hormones are produced by the cells, the hormones are either released into the colloid or directly into the blood. There also extrafollicular hormone-secreting cells, called C cells. These are found between lumina. Hormones Produced: § § § Thyroxine (T 4) Triiodotyronine (T 3) Calcitonin made in follicle made by C cells
The Thyroid Gland Structure: This bilobed gland contains many follicles. A follicle is a group of cells encircling a lumen. The lumen contains material called colloid (a glycoprotein) within it. As hormones are produced by the cells, the hormones are either released into the colloid or directly into the blood. There also extrafollicular hormone-secreting cells, called C cells. These are found between lumina. Hormones Produced: § § § Thyroxine (T 4) Triiodotyronine (T 3) Calcitonin made in follicle made by C cells
 About the Thyroid Hormones. . . T 3 and T 4: Calcitonin: § Function: metabolism regulation (break down carbohydrates and fats, synthesize proteins) § Can only be made by follicular cells when iodides are available § Somewhat hydrophobic and get carried by proteins in the blood. § Controlled by anterior pituitary lobe TSH § Function: decrease blood calcium levels and blood phosphate levels (by helping them get deposited in bone, and by stimulating excretion of them by kidneys) § Controlled by blood calcium levels and digestive chemicals
About the Thyroid Hormones. . . T 3 and T 4: Calcitonin: § Function: metabolism regulation (break down carbohydrates and fats, synthesize proteins) § Can only be made by follicular cells when iodides are available § Somewhat hydrophobic and get carried by proteins in the blood. § Controlled by anterior pituitary lobe TSH § Function: decrease blood calcium levels and blood phosphate levels (by helping them get deposited in bone, and by stimulating excretion of them by kidneys) § Controlled by blood calcium levels and digestive chemicals
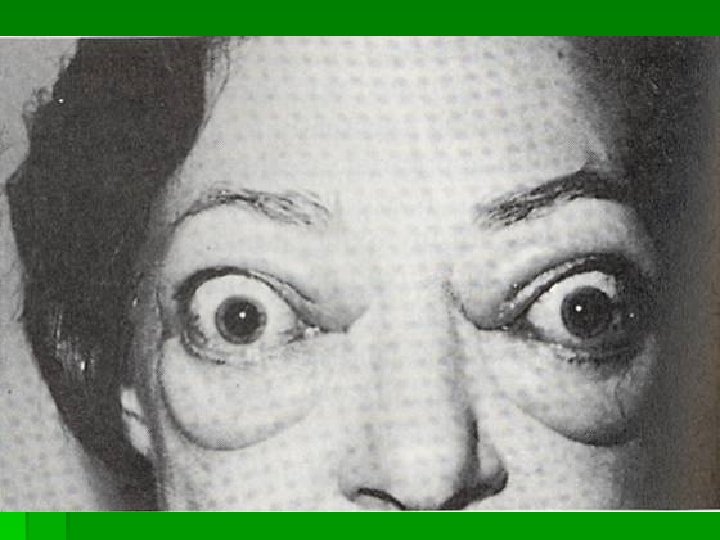
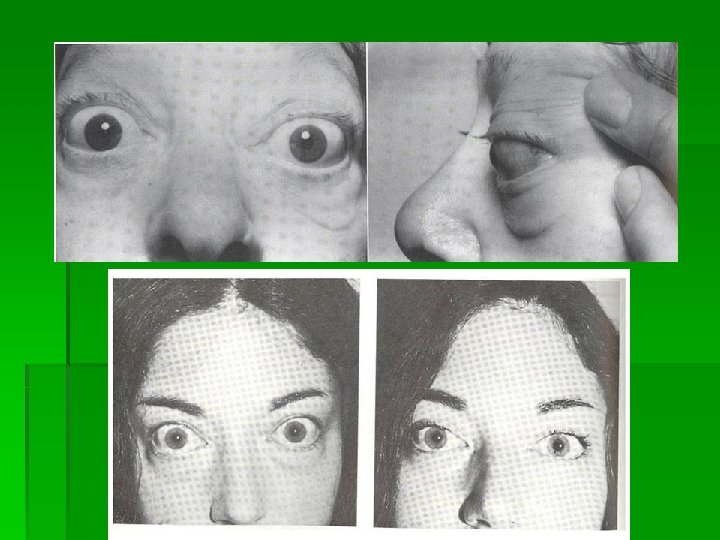
 Problems with the Thyroid Gland Hyperthyroidism: § high metabolic rate, hyperactivity, sensitivity to heat, protruding eyes § Grave’s disease: when hyperthyroidism is due to an autoimmune problem (TSH is mimicked by autoantibodies) Hypothyroidism: § in the adult: low metabolic rate, sensitivity to cold, sluggishness § in an infant: cretinism-- stunted growth, mental retardation, abnormal bone formation § Hashimoto’s disease: when hypothyroidism is due to an autoimmune problem (autoantibodies attack and destroy follicular cells)
Problems with the Thyroid Gland Hyperthyroidism: § high metabolic rate, hyperactivity, sensitivity to heat, protruding eyes § Grave’s disease: when hyperthyroidism is due to an autoimmune problem (TSH is mimicked by autoantibodies) Hypothyroidism: § in the adult: low metabolic rate, sensitivity to cold, sluggishness § in an infant: cretinism-- stunted growth, mental retardation, abnormal bone formation § Hashimoto’s disease: when hypothyroidism is due to an autoimmune problem (autoantibodies attack and destroy follicular cells)
 § § § § Regulates basal metabolic rate Improves cardiac contractility Increases") Thyroid (cont) § § § § Regulates basal metabolic rate Improves cardiac contractility Increases the gain of catecholamines Increases bowel motility Increases speed of muscle contraction Decreases cholesterol (LDL) Required for proper fetal neural growth
Thyroid (cont) § § § § Regulates basal metabolic rate Improves cardiac contractility Increases the gain of catecholamines Increases bowel motility Increases speed of muscle contraction Decreases cholesterol (LDL) Required for proper fetal neural growth
 Thyroid Physiology § § § § Uptake of Iodine by thyroid Coupling of Iodine to Thyroglobulin Storage of MIT / DIT in follicular space Re-absorption of MIT / DIT Formation of T 3, T 4 from MIT / DIT Release of T 3, T 4 into serum Breakdown of T 3, T 4 with release of Iodine
Thyroid Physiology § § § § Uptake of Iodine by thyroid Coupling of Iodine to Thyroglobulin Storage of MIT / DIT in follicular space Re-absorption of MIT / DIT Formation of T 3, T 4 from MIT / DIT Release of T 3, T 4 into serum Breakdown of T 3, T 4 with release of Iodine
 Iodine uptake § Na+/I- symport protein controls serum Iuptake § Based on Na+/K+ antiport potential § Stimulated by TSH § Inhibited by Perchlorate
Iodine uptake § Na+/I- symport protein controls serum Iuptake § Based on Na+/K+ antiport potential § Stimulated by TSH § Inhibited by Perchlorate
 Secretion of Thyroid Hormone § Stimulated by TSH § Endocytosis of colloid on apical membrane § Coupling of MIT & DIT residues § § § Catalyzed by TPO MIT + DIT = T 3 DIT + DIT = T 4 § Hydrolysis of Thyroglobulin § Release of T 3, T 4 § Release inhibited by Lithium
Secretion of Thyroid Hormone § Stimulated by TSH § Endocytosis of colloid on apical membrane § Coupling of MIT & DIT residues § § § Catalyzed by TPO MIT + DIT = T 3 DIT + DIT = T 4 § Hydrolysis of Thyroglobulin § Release of T 3, T 4 § Release inhibited by Lithium
 Thyroid Hormones
Thyroid Hormones
 Thyroid Hormone § Majority of circulating hormone is T 4 § § 98. 5% T 4 1. 5% T 3 § Total Hormone load is influenced by serum binding proteins (TBP, Albumin, ? ? ) § § § Thyroid Binding Globulin 70% Albumin 15% Transthyretin 10% § Regulation is based on the free component of thyroid hormone
Thyroid Hormone § Majority of circulating hormone is T 4 § § 98. 5% T 4 1. 5% T 3 § Total Hormone load is influenced by serum binding proteins (TBP, Albumin, ? ? ) § § § Thyroid Binding Globulin 70% Albumin 15% Transthyretin 10% § Regulation is based on the free component of thyroid hormone
 Hormone Binding Factors § Increased TBG § § § Decreased TBG § § § High estrogen states (pregnancy, OCP, HRT, Tamoxifen) Liver disease (early) Androgens or anabolic steroids Liver disease (late) Binding Site Competition § § § NSAID’s Furosemide IV Anticonvulsants (Phenytoin, Carbamazepine)
Hormone Binding Factors § Increased TBG § § § Decreased TBG § § § High estrogen states (pregnancy, OCP, HRT, Tamoxifen) Liver disease (early) Androgens or anabolic steroids Liver disease (late) Binding Site Competition § § § NSAID’s Furosemide IV Anticonvulsants (Phenytoin, Carbamazepine)
 by 5’") Hormone Degredation § § T 4 is converted to T 3 (active) by 5’ deiodinase T 4 can be converted to r. T 3 (inactive) by 5 deiodinase T 3 is converted to r. T 2 (inactive)by 5 deiodinase r. T 3 is inactive but measured by serum tests
Hormone Degredation § § T 4 is converted to T 3 (active) by 5’ deiodinase T 4 can be converted to r. T 3 (inactive) by 5 deiodinase T 3 is converted to r. T 2 (inactive)by 5 deiodinase r. T 3 is inactive but measured by serum tests
 Thyroid Hormone Control
Thyroid Hormone Control
 TRH § § Produced by Hypothalamus Release is pulsatile, circadian Downregulated by T 4, T 3 Travels through portal venous system to adenohypophysis § Stimulates TSH formation
TRH § § Produced by Hypothalamus Release is pulsatile, circadian Downregulated by T 4, T 3 Travels through portal venous system to adenohypophysis § Stimulates TSH formation
 TSH § § Produced by Adenohypophysis Thyrotrophs Upregulated by TRH Downregulated by T 4, T 3 Travels through portal venous system to cavernous sinus, body. § Stimulates several processes § § § Iodine uptake Colloid endocytosis Growth of thyroid gland
TSH § § Produced by Adenohypophysis Thyrotrophs Upregulated by TRH Downregulated by T 4, T 3 Travels through portal venous system to cavernous sinus, body. § Stimulates several processes § § § Iodine uptake Colloid endocytosis Growth of thyroid gland
 TSH Response
TSH Response
 Iodine states § Normal Thyroid § Inactive Thyroid § Hyperactive Thyroid
Iodine states § Normal Thyroid § Inactive Thyroid § Hyperactive Thyroid
 Hypothyroid § Symptoms – fatigability, coldness, weight gain, constipation, low voice § Signs – Cool skin, dry skin, swelling of face/hands/legs, slow reflexes, myxedema § Newborn – Retardation, short stature, swelling of face/hands, possible deafness § Types of Hypothyroidism § § Primary – Thyroid gland failure Secondary – Pituitary failure Tertiary – Hypothalamic failure Peripheral resistance
Hypothyroid § Symptoms – fatigability, coldness, weight gain, constipation, low voice § Signs – Cool skin, dry skin, swelling of face/hands/legs, slow reflexes, myxedema § Newborn – Retardation, short stature, swelling of face/hands, possible deafness § Types of Hypothyroidism § § Primary – Thyroid gland failure Secondary – Pituitary failure Tertiary – Hypothalamic failure Peripheral resistance
 Hypothyroid § Cause is determined by geography § Diagnosis § Low FT 4, High TSH (Primary, check for antibodies) § Low FT 4, Low TSH (Secondary or Tertiary, TRH stimulation test, MRI) § Treatment § Levothyroxine (T 4) due to longer half life § Treatment prevents bone loss, cardiomyopathy, myxedema
Hypothyroid § Cause is determined by geography § Diagnosis § Low FT 4, High TSH (Primary, check for antibodies) § Low FT 4, Low TSH (Secondary or Tertiary, TRH stimulation test, MRI) § Treatment § Levothyroxine (T 4) due to longer half life § Treatment prevents bone loss, cardiomyopathy, myxedema
 Goiter § Endemic goiter § Caused by dietary deficiency of Iodide § Increased TSH stimulates gland growth § Also results in cretinism § Goiter in developed countries § Hashimoto’s thryoiditis § Subacute thyroiditis § Other causes § Excess Iodide (Amiodarone, Kelp, Lithium) § Adenoma, Malignancy § Genetic / Familial hormone synthesis defects
Goiter § Endemic goiter § Caused by dietary deficiency of Iodide § Increased TSH stimulates gland growth § Also results in cretinism § Goiter in developed countries § Hashimoto’s thryoiditis § Subacute thyroiditis § Other causes § Excess Iodide (Amiodarone, Kelp, Lithium) § Adenoma, Malignancy § Genetic / Familial hormone synthesis defects
 Hyperthyroid § § § Symptoms – Palpitations, nervousness, fatigue, diarrhea, sweating, heat intolerance Signs – Thyroid enlargement (? ), tremor Lab workup § § TSH FT 4 RAIU Other Labs § § Anti-TSH-R Ab, Anti-TPO Ab, Anti-TBG Ab FT 3 FNA MRI, US
Hyperthyroid § § § Symptoms – Palpitations, nervousness, fatigue, diarrhea, sweating, heat intolerance Signs – Thyroid enlargement (? ), tremor Lab workup § § TSH FT 4 RAIU Other Labs § § Anti-TSH-R Ab, Anti-TPO Ab, Anti-TBG Ab FT 3 FNA MRI, US
 Hyperthyroid § Common Causes § § § *Graves Adenoma Multinodular Goiter *Subacute Thyroiditis *Hashimoto’s Thyroiditis § Rare Causes § Thyrotoxicosis factitia, struma ovarii, thyroid metastasis, TSH-secreting tumor, hamburger
Hyperthyroid § Common Causes § § § *Graves Adenoma Multinodular Goiter *Subacute Thyroiditis *Hashimoto’s Thyroiditis § Rare Causes § Thyrotoxicosis factitia, struma ovarii, thyroid metastasis, TSH-secreting tumor, hamburger
 The Endocrine Glands § Parathyroid Glands § Secretes parathyroid hormone § regulates plasma calcium (osteoclast activity) § regulates phosphate levels
The Endocrine Glands § Parathyroid Glands § Secretes parathyroid hormone § regulates plasma calcium (osteoclast activity) § regulates phosphate levels
 Calcium Regulation Parathyroid
Calcium Regulation Parathyroid
 Calcium § Required for muscle contraction, intracellular messenger systems, cardiac repolarization. § Exists in free and bound states § Albumin (40% total calcium) § Phosphate and Citrate (10% total calcium) § Concentration of i. Ca++ mediated by § § Parathyroid gland Parafollicular C cells Kidney Bone
Calcium § Required for muscle contraction, intracellular messenger systems, cardiac repolarization. § Exists in free and bound states § Albumin (40% total calcium) § Phosphate and Citrate (10% total calcium) § Concentration of i. Ca++ mediated by § § Parathyroid gland Parafollicular C cells Kidney Bone
 §") Parathyroid Gland § This gland only secretes one hormone: Parathyroid Hormone (or PTH) § PTH function (we began learning this when we studied bone): § increases blood calcium (Ca 2+) levels and decreases blood phosphate (PO 42 -
Parathyroid Gland § This gland only secretes one hormone: Parathyroid Hormone (or PTH) § PTH function (we began learning this when we studied bone): § increases blood calcium (Ca 2+) levels and decreases blood phosphate (PO 42 -
 § How does PTH work? § PTH causes Ca 2+ &") PTH function (continued) § How does PTH work? § PTH causes Ca 2+ & PO 42 - to be released from bone into blood (by increasing osteoclast activity) § PTH causes the kidneys to remove PO 42 - ions from the urine § PTH increases vitamin D production, so that you absorb more Ca 2+ during digestion § PTH is regulated by blood calcium levels-- not by other glands!
PTH function (continued) § How does PTH work? § PTH causes Ca 2+ & PO 42 - to be released from bone into blood (by increasing osteoclast activity) § PTH causes the kidneys to remove PO 42 - ions from the urine § PTH increases vitamin D production, so that you absorb more Ca 2+ during digestion § PTH is regulated by blood calcium levels-- not by other glands!
 Parathyroid Hormone § Produced by Parathyroid Chief cells § Secreted in response to low i. Ca++ § Stimulates renal conversion of 25 -(OH)D 3 to 1, 25 -(OH)2 D which increases intestinal Ca++ absorption § Directly stimulates renal Ca++ absorption and PO 43 - excretion § Stimulates osteoclastic resorption of bone
Parathyroid Hormone § Produced by Parathyroid Chief cells § Secreted in response to low i. Ca++ § Stimulates renal conversion of 25 -(OH)D 3 to 1, 25 -(OH)2 D which increases intestinal Ca++ absorption § Directly stimulates renal Ca++ absorption and PO 43 - excretion § Stimulates osteoclastic resorption of bone
 Calcitonin § Produced by Parafollicular C cells of Thyroid in response to increased i. Ca++ § Actions § Inhibit osteoclastic resorption of bone § Increase renal Ca++ and PO 43 - excretion § Non-essential hormone. Patients with total thyroidectomy maintain normal Ca++ concentrations § Useful in monitoring treatment of Medullary Thyroid cancer § Used in treatment of Pagets’, Osteoporosis
Calcitonin § Produced by Parafollicular C cells of Thyroid in response to increased i. Ca++ § Actions § Inhibit osteoclastic resorption of bone § Increase renal Ca++ and PO 43 - excretion § Non-essential hormone. Patients with total thyroidectomy maintain normal Ca++ concentrations § Useful in monitoring treatment of Medullary Thyroid cancer § Used in treatment of Pagets’, Osteoporosis
 Vitamin D § Sources § Food – Vitamin D 2 § UV light mediated cholesterol metabolism – D 3 § Metabolism § D 2 and D 3 are converted to 25(OH)-D by the liver § 25(OH)-D is converted to 1, 25(OH)2 -D by the Kidney § Function § Stimulation of Osteoblasts § Increases GI absorption of dietary Ca++
Vitamin D § Sources § Food – Vitamin D 2 § UV light mediated cholesterol metabolism – D 3 § Metabolism § D 2 and D 3 are converted to 25(OH)-D by the liver § 25(OH)-D is converted to 1, 25(OH)2 -D by the Kidney § Function § Stimulation of Osteoblasts § Increases GI absorption of dietary Ca++
 Hypocalcemia § Decreased PTH § § Resistance to PTH § § § Genetic disorders Bisphonates Vitamin D abnormalities § § § Surgery Hypomagnesemia Idiopathic Vitamin D deficiency Rickets (VDR or Renal hyroxylase abnormalities) Binding of Calcium § § Hyperphosphate states (Crush injury, Tumor lysis, etc. ) Blood Transfusion (Citrate)
Hypocalcemia § Decreased PTH § § Resistance to PTH § § § Genetic disorders Bisphonates Vitamin D abnormalities § § § Surgery Hypomagnesemia Idiopathic Vitamin D deficiency Rickets (VDR or Renal hyroxylase abnormalities) Binding of Calcium § § Hyperphosphate states (Crush injury, Tumor lysis, etc. ) Blood Transfusion (Citrate)
2") Hypercalcemia § Hyperparathyroidism § § § Malignancy § § Overproduction of 1, 25 (OH)2 D Drug-Induced § § § Humoral Hypercalcemia PTHr. P (Lung Cancer) Osteoclastic activity (Myeloma, Lymphoma) Granulomatous Diseases § § Primary, Secondary, Tertiary MEN Syndromes Thiazides Lithium Milk-Alkali Vitamin A, D Renal failure
Hypercalcemia § Hyperparathyroidism § § § Malignancy § § Overproduction of 1, 25 (OH)2 D Drug-Induced § § § Humoral Hypercalcemia PTHr. P (Lung Cancer) Osteoclastic activity (Myeloma, Lymphoma) Granulomatous Diseases § § Primary, Secondary, Tertiary MEN Syndromes Thiazides Lithium Milk-Alkali Vitamin A, D Renal failure
 Hypercalcemia § Signs & Symptoms § § § Medical Treatment § § § § Bones (Osteitis fibrosa cystica, osteoporosis, rickets) Stones (Renal stones) Groans (Constipation, peptic ulcer) Moans (Lethargy, depression, confusion) SERM’s (Evista) Bisphonates (Pamidronate) Calcitonin (for severe cases) Saline diuresis Glucocorticoids (for malignant/granulomatous diseases) Avoid thiazide diuretics Surgical Treatment § § Single vs. Double adenoma – simple excision Multiple Gland hyperplasia – total parathyroid with autotransplant vs. 3½ gland excision
Hypercalcemia § Signs & Symptoms § § § Medical Treatment § § § § Bones (Osteitis fibrosa cystica, osteoporosis, rickets) Stones (Renal stones) Groans (Constipation, peptic ulcer) Moans (Lethargy, depression, confusion) SERM’s (Evista) Bisphonates (Pamidronate) Calcitonin (for severe cases) Saline diuresis Glucocorticoids (for malignant/granulomatous diseases) Avoid thiazide diuretics Surgical Treatment § § Single vs. Double adenoma – simple excision Multiple Gland hyperplasia – total parathyroid with autotransplant vs. 3½ gland excision
 Primary Hyperparathyroidism § Diagnosis § § § Signs & Symptoms Elevated serum calcium Elevated PTH § Etiology § § § Solitary Adenoma (80 -85%) Double Adenomas (2 -4%) Muliple Gland Hyperplasia (10 -30%) Parathyroid Carcinoma (0. 5%) MEN syndromes (10% of MGH have MEN 1)
Primary Hyperparathyroidism § Diagnosis § § § Signs & Symptoms Elevated serum calcium Elevated PTH § Etiology § § § Solitary Adenoma (80 -85%) Double Adenomas (2 -4%) Muliple Gland Hyperplasia (10 -30%) Parathyroid Carcinoma (0. 5%) MEN syndromes (10% of MGH have MEN 1)
 Parathyroidectomy § 1990 NIH Guidelines § § § Serum Ca++ > 12 mg/dl Hypercalciuria > 400 mg/day Classic symptoms § § § § Nephrolithiasis Osteitis fibrosa cystica Neuromuscular disease Cortical bone loss with DEXA Z score < -2 Reduced creatinine clearance Age < 50 Other considerations § § § Vertebral osteopenia Vitamin D deficency Perimenopause
Parathyroidectomy § 1990 NIH Guidelines § § § Serum Ca++ > 12 mg/dl Hypercalciuria > 400 mg/day Classic symptoms § § § § Nephrolithiasis Osteitis fibrosa cystica Neuromuscular disease Cortical bone loss with DEXA Z score < -2 Reduced creatinine clearance Age < 50 Other considerations § § § Vertebral osteopenia Vitamin D deficency Perimenopause
 The Endocrine Glands § Adrenal Medulla § Situated directly atop each kidney and stimulated by the sympathetic nervous system § Secretes the catecholamines § Epinephrine: elicits a fight or flight response § Increase H. R. and B. P. § Increase respiration § Increase metabolic rate § Increase glycogenolysis § Vasodilation
The Endocrine Glands § Adrenal Medulla § Situated directly atop each kidney and stimulated by the sympathetic nervous system § Secretes the catecholamines § Epinephrine: elicits a fight or flight response § Increase H. R. and B. P. § Increase respiration § Increase metabolic rate § Increase glycogenolysis § Vasodilation
") The Endocrine Glands § Adrenal Cortex § Secretes over 30 different steroid hormones (corticosteroids) § Mineralocorticoids § Aldosterone: maintains electrolyte balance § Glucocorticoids § Cortisol: § Stimulates gluconeogenisis § Mobilization of free fatty acids § Glucose sparing § Anti-inflammatory agent
The Endocrine Glands § Adrenal Cortex § Secretes over 30 different steroid hormones (corticosteroids) § Mineralocorticoids § Aldosterone: maintains electrolyte balance § Glucocorticoids § Cortisol: § Stimulates gluconeogenisis § Mobilization of free fatty acids § Glucose sparing § Anti-inflammatory agent
 The Endocrine Glands § § § Pancrease: Located slightly behind the stomach Insulin: reduces blood glucose § Facilitates glucose transport into the cells § Promotes glycogenesis § Inhibits gluconeogensis § Glucagon: increases blood glucose
The Endocrine Glands § § § Pancrease: Located slightly behind the stomach Insulin: reduces blood glucose § Facilitates glucose transport into the cells § Promotes glycogenesis § Inhibits gluconeogensis § Glucagon: increases blood glucose
 = sex characteristics § muscle development") The Endocrine Glands § Gonads § testes (testosterone) = sex characteristics § muscle development and maturity § ovaries (estrogen) = sex characteristics § maturity and coordination § Kidneys (erythropoietin) § regulates red blood cell production
The Endocrine Glands § Gonads § testes (testosterone) = sex characteristics § muscle development and maturity § ovaries (estrogen) = sex characteristics § maturity and coordination § Kidneys (erythropoietin) § regulates red blood cell production
 The Endocrine Response to Exercise § Table 5. 3 Page 172
The Endocrine Response to Exercise § Table 5. 3 Page 172
 Regulation of Glucose Metabolism During Exercise § Glucagon secretion increases during exercise to promote liver glycogen breakdown (glycogenolysis) § Epinephrine and Norepinephrine further increase glycogenolysis § Cortisol levels also increase during exercise for protein catabolism for later gluconeogenesis. § Growth Hormone mobilizes free fatty acids § Thyroxine promotes glucose catabolism
Regulation of Glucose Metabolism During Exercise § Glucagon secretion increases during exercise to promote liver glycogen breakdown (glycogenolysis) § Epinephrine and Norepinephrine further increase glycogenolysis § Cortisol levels also increase during exercise for protein catabolism for later gluconeogenesis. § Growth Hormone mobilizes free fatty acids § Thyroxine promotes glucose catabolism
 Regulation of Glucose Metabolism During Exercise § As intensity of exercise increases, so does the rate of catecholamine release for glycogenolysis § During endurance events the rate of glucose release very closely matches the muscles need. (fig 5. 9, pg. 174) § When glucose levels become depleted, glucagon and cortisol levels rise significantly to enhance gluconeogenesis.
Regulation of Glucose Metabolism During Exercise § As intensity of exercise increases, so does the rate of catecholamine release for glycogenolysis § During endurance events the rate of glucose release very closely matches the muscles need. (fig 5. 9, pg. 174) § When glucose levels become depleted, glucagon and cortisol levels rise significantly to enhance gluconeogenesis.
 Regulation of Glucose Metabolism During Exercise § Glucose must not only be delivered to the cells, it must also be taken up by them. That job relies on insulin. § Exercise may enhance insulin’s binding to receptors on the muscle fiber. § Up-regulation (receptors) occurs with insulin after 4 weeks of exercise to increase its sensitivity (diabetic importance).
Regulation of Glucose Metabolism During Exercise § Glucose must not only be delivered to the cells, it must also be taken up by them. That job relies on insulin. § Exercise may enhance insulin’s binding to receptors on the muscle fiber. § Up-regulation (receptors) occurs with insulin after 4 weeks of exercise to increase its sensitivity (diabetic importance).
 Regulation of Fat Metabolism During Exercise § When low plasma glucose levels occur, the catecholamines are released to accelerate lypolysis. § Triglycerides are reduced to free fatty acids by lipase which is activated by: (fig. 5. 11, pg. 176) § Cortisol § Epinephrine § Norepinephrine § Growth Hormone
Regulation of Fat Metabolism During Exercise § When low plasma glucose levels occur, the catecholamines are released to accelerate lypolysis. § Triglycerides are reduced to free fatty acids by lipase which is activated by: (fig. 5. 11, pg. 176) § Cortisol § Epinephrine § Norepinephrine § Growth Hormone
 Hormonal Effects on Fluid and Electrolyte Balance § Reduced plasma volume leads to release of aldosterone which increases Na+ and H 2 O reabsorption by the kidneys and renal tubes. § Antidiuretic Hormone (ADH) is released from the posterior pituitary when dehydration is sensed by osmoreceptors, and water is then reabsorbed by the kidneys.
Hormonal Effects on Fluid and Electrolyte Balance § Reduced plasma volume leads to release of aldosterone which increases Na+ and H 2 O reabsorption by the kidneys and renal tubes. § Antidiuretic Hormone (ADH) is released from the posterior pituitary when dehydration is sensed by osmoreceptors, and water is then reabsorbed by the kidneys.
 Adrenal Glands An adrenal gland is found on top of each kidney. Each adrenal gland has two regions that carry out separate functions! • The adrenal medulla • The adrenal cortex We will cover each of these two regions separately in the next few slides.
Adrenal Glands An adrenal gland is found on top of each kidney. Each adrenal gland has two regions that carry out separate functions! • The adrenal medulla • The adrenal cortex We will cover each of these two regions separately in the next few slides.
 The Adrenal Medulla Acts very much like a part of the sympathetic nervous system (fight or flight) Secretes two amines: § norepinephrine (20%) § epinephrine (80%) Stimulated by preganglionic neurons directly, so controlled by the hypothalamus as if part of the autonomic nervous system, NOT by tropic hormones
The Adrenal Medulla Acts very much like a part of the sympathetic nervous system (fight or flight) Secretes two amines: § norepinephrine (20%) § epinephrine (80%) Stimulated by preganglionic neurons directly, so controlled by the hypothalamus as if part of the autonomic nervous system, NOT by tropic hormones
 The Adrenal Cortex Acts like a regular endocrine organ Secretes many hormones, but most importantly secretes the following steroids: § aldosterone § cortisol § sex hormones Aldosterone and cortisol require further explanation (while sex hormone production will be covered later this semester)
The Adrenal Cortex Acts like a regular endocrine organ Secretes many hormones, but most importantly secretes the following steroids: § aldosterone § cortisol § sex hormones Aldosterone and cortisol require further explanation (while sex hormone production will be covered later this semester)
 More about Adrenal Cortex Hormones Aldosterone: Cortisol: Considered a mineralocorticoid Regulates “mineral electrolyte” levels in the blood (for example: Na+ and K+ ions) How is aldosterone controlled? § blood plasma ion concentrations affect its secretion directly (but not always strongly) § kidney secretes renin in response to altered electrolyte levels, which triggers angiotensin activation in the blood, which leads to aldosterone secretion Considered a glucocorticoid Overall effect of cortisol: § Helps to keep blood glucose concentration within a normal range between meals Specific actions of cortisol: § increases amino acid concentration in the blood (by inhibiting protein synthesis in select tissues) § promotes use of fat for energy production in our bodies (rather than glucose) § stimulates the liver to synthesize glucose (not from carbohydrates, but from amino acids and
More about Adrenal Cortex Hormones Aldosterone: Cortisol: Considered a mineralocorticoid Regulates “mineral electrolyte” levels in the blood (for example: Na+ and K+ ions) How is aldosterone controlled? § blood plasma ion concentrations affect its secretion directly (but not always strongly) § kidney secretes renin in response to altered electrolyte levels, which triggers angiotensin activation in the blood, which leads to aldosterone secretion Considered a glucocorticoid Overall effect of cortisol: § Helps to keep blood glucose concentration within a normal range between meals Specific actions of cortisol: § increases amino acid concentration in the blood (by inhibiting protein synthesis in select tissues) § promotes use of fat for energy production in our bodies (rather than glucose) § stimulates the liver to synthesize glucose (not from carbohydrates, but from amino acids and
 The Pancreas § This gland has both endocrine and exocrine functions… we’ll only cover the endocrine portion now (exocrine is for digestion) § The endocrine portion of the gland contains three types of cells, each making a different hormone, arranged into groups called Islets of Langerhans § § § alpha cells: secrete glucagon beta cells: secrete insulin delta cells: secrete SS (somatostatin) § Note that these pancreatic hormones are involved in blood glucose regulation, and problems with them can lead to diabetes.
The Pancreas § This gland has both endocrine and exocrine functions… we’ll only cover the endocrine portion now (exocrine is for digestion) § The endocrine portion of the gland contains three types of cells, each making a different hormone, arranged into groups called Islets of Langerhans § § § alpha cells: secrete glucagon beta cells: secrete insulin delta cells: secrete SS (somatostatin) § Note that these pancreatic hormones are involved in blood glucose regulation, and problems with them can lead to diabetes.
 Blood Glucose Regulation by the Pancreas Glucagon: Insulin: It works on the liver to cause the production of glucose via: § glycogenolysis § gluconeogenesis It is regulated by blood glucose levels directly: It works on the liver to remove glucose from the blood via: § making glycogen § preventing gluconeogenesis § increasing glucose transport into cells § secreted when blood glucose drops (before next It is also regulated by blood glucose levels meal) directly Note: glucagon and insulin work in hyperglycemia Prevents opposition, and Prevents hypoglycemia their combined effects control blood glucose
Blood Glucose Regulation by the Pancreas Glucagon: Insulin: It works on the liver to cause the production of glucose via: § glycogenolysis § gluconeogenesis It is regulated by blood glucose levels directly: It works on the liver to remove glucose from the blood via: § making glycogen § preventing gluconeogenesis § increasing glucose transport into cells § secreted when blood glucose drops (before next It is also regulated by blood glucose levels meal) directly Note: glucagon and insulin work in hyperglycemia Prevents opposition, and Prevents hypoglycemia their combined effects control blood glucose
 Pineal Gland Secretes only one hormone: melatonin Involved in your circadian rhythm (your recognition of day and night times): § melatonin secretion decreases in the day § melatonin secretion increases at night Melatonin is also involved in longer rhythms, like monthly and seasonal… and is thought to be involved in the female menstrual cycle and maybe in the onset of puberty
Pineal Gland Secretes only one hormone: melatonin Involved in your circadian rhythm (your recognition of day and night times): § melatonin secretion decreases in the day § melatonin secretion increases at night Melatonin is also involved in longer rhythms, like monthly and seasonal… and is thought to be involved in the female menstrual cycle and maybe in the onset of puberty
 Other Endocrine Glands § Thymus Gland: secretes thymosins which are involved in white blood cell production § Reproductive glands (the gonads): the ovaries and the testes produce sex hormones § Others: too specific for now, we’ll get to them as we continue this semester.
Other Endocrine Glands § Thymus Gland: secretes thymosins which are involved in white blood cell production § Reproductive glands (the gonads): the ovaries and the testes produce sex hormones § Others: too specific for now, we’ll get to them as we continue this semester.
