367f12f3c6b1c845be311b6e0a48c028.ppt
- Количество слайдов: 30



The contribution of DPHs and teams to world class commissioning A regional perspective 11 September 2009 Dr Paul Cosford
 1. Are recognised as the local leader of the NHS 2.")
The competencies (1/2) 1. Are recognised as the local leader of the NHS 2. Work collaboratively with community partners to commission services that optimise health gains and reductions in health inequalities 3. Proactively seek and build continuous and meaningful engagement with the public and patients, to shape services and improve health 4. Lead continuous and meaningful engagement with clinicians to inform strategy and drive quality, service design and resource utilisation 5. Manage knowledge and undertake robust and regular needs assessments that establish a full understanding of current and future local health needs and requirements
 6. Prioritise investment according to local needs, service requirements and the")
The competencies (2/2) 6. Prioritise investment according to local needs, service requirements and the values of the NHS 7. Effectively stimulate the market to meet demand secure required clinical and health and well-being outcomes 8. Promote and specify continuous improvements in quality and outcomes through clinical and provider innovation and configuration 9. Secure procurement skills that ensure robust and viable contracts 10. Effectively manage systems and work in partnership with providers to ensure contract compliance and continuous improvements in quality and outcomes 11. Make sound financial investments to ensure sustainable delivery of priority outcomes

What do I hope for from the DPH and their teams? • Source of objective advice – Based on agreed policy objectives, needs assessment and evidence • Promotion of the wider health agenda – As a role for the NHS – As a role for local authorities – Illustrating the need to work across the public sector • Monitoring effectiveness • Taking responsibility for delivering health outcomes • Corporacy – able to deliver through current priority programmes (eg QIPP) • Able to react effectively to new problems (eg swine flu)

What do I hope for from the DPH and their teams? • Source of objective advice – Based on agreed policy objectives, needs assessment and evidence • Promotion of the wider health agenda – As a role for the NHS – As a role for local authorities – Illustrating the need to work across the public sector • Monitoring effectiveness • Taking responsibility for delivering health outcomes • Corporacy – able to deliver through current priority programmes (eg QIPP) • Able to react effectively to new problems (eg swine flu)

The context – policy underpinning commissioning

Survival in 20244 healthy men and women 40 -79 years EPIC-Norfolk 1993 -2006 by health behaviour score P<0. 0001 Score 0 -4 Equivalent 14 years 1 Non smoker 1 Alcohol >0 <14 units/wk 1 Not inactive 1 Blood vitamin C >50 umol/l (5 servings fruit and vegetables daily) Khaw et al PLo. S Med 2008 Jan 8; 5(1): e 12.

Example – pre-op smoking cessation Costs across East of England: 72, 000 elective admissions are smokers Costs of Nicotine Replacement Therapy £ 300, 000 Cost of staff time £ 430, 000 Total for East of England £ 790, 000 Cost per admission £ 3

Benefits of pre-op smoking cessation 10% Quit rate Episodes Cost saved prevente d 30 % Quit rate Episodes prevente d Cost saved Healthcare acquired Infection 790 £ 2. 3 m 2400 £ 6. 9 m Thromboembolism 95 £ 0. 3 m 280 £ 0. 9 m 885 £ 2. 6 m 2680 £ 7. 9 m Total

What do I hope for from the DPH and their teams? • Source of objective advice – Based on agreed policy objectives, needs assessment and evidence • Promotion of the wider health agenda – As a role for the NHS – As a role for local authorities – Illustrating the need to work across the public sector • Monitoring effectiveness • Taking responsibility for delivering health outcomes • Corporacy – able to deliver through current priority programmes (eg QIPP) • Able to react effectively to new problems (eg swine flu)

Example – implementation of NICE falls guidance East of England data, if achieves 15% reduction in falls: Falls prevented 52, 000 Admissions prevented 2, 900 Costs saved £ 14 m Fractured neck of femur prevented 820 Bed days saved 21, 500 Costs saved £ 3. 6 m

What do I hope for from the DPH and their teams? • Source of objective advice – Based on agreed policy objectives, needs assessment and evidence • Promotion of the wider health agenda – As a role for the NHS – As a role for local authorities – Illustrating the need to work across the public sector • Monitoring effectiveness • Taking responsibility for delivering health outcomes • Corporacy – able to deliver through current priority programmes (eg QIPP) • Able to react effectively to new problems (eg swine flu)

Monitor the life expectancy gap
 rd s M hir C id am E e")
Smoking Prevalence in adults (%) rd s M hir C id am E e br sse id x g Be es df hir e or W dsh es ir t E e ss e Su x W ffo es G lk re t H Lu at er Y tfo ton ar rd m sh ou ir th a N e nd or W fol k Pe av en So te ut rbo ey h ro u N Ea or st gh E th So Ea ss ex ut s h t E W s es sex t E ss ex tfo er H or th N & st Ea Smoking prevalence - most deprived 20% vs other 80% by PCT 35 30 25 20 15 10 20% most deprived in PCT 5 0 PCT Source: East of England Lifestyle Survey 2008 80% least deprived in PCT

What do I hope for from the DPH and their teams? • Source of objective advice – Based on agreed policy objectives, needs assessment and evidence • Promotion of the wider health agenda – As a role for the NHS – As a role for local authorities – Illustrating the need to work across the public sector • Monitoring effectiveness • Taking responsibility for delivering health outcomes • Corporacy – able to deliver through current priority programmes (eg QIPP) • Able to react effectively to new problems (eg swine flu)

Focus on delivery

What do I hope for from the DPH and their teams? • Source of objective advice – Based on agreed policy objectives, needs assessment and evidence • Promotion of the wider health agenda – As a role for the NHS – As a role for local authorities – Illustrating the need to work across the public sector • Monitoring effectiveness • Taking responsibility for delivering health outcomes • Corporacy – able to deliver through current priority programmes (eg QIPP) • Able to react effectively to new problems (eg swine flu)

QIPP proposals Headline / Title: NHS Prevention A systematic referral and service delivery system to address the four key lifestyle factors for Short description: health ( smoking, alcohol, diet & physical activity), and mental wellbeing. This would be available for referral by GPs & primary care professionals, clinicians in acute & mental health trusts, & healthy workplace leads within the NHS, wider public sector and private employers QIPP elements * Making it happen • Estimated quality impact** • Practitioners do not know where to refer for effective interventions. This provides quality assured services & simple means of referral. • Estimated productivity impact • Reduced demand for healthcare interventions. • Reduced NHS sickness absence. • Increased productivity for whole economy. • Is it linked to the prevention agenda (if at all)? • Systematises NHS prevention role • Underpins health at work for NHS, public & private sector employers • Potential to improve lifestyle & reduce dependency in older people • What innovation is required (if any)? • Are there additional effects on the system? • Links all clinical & social services, & health at work programmes to personalised assessment of lifestyle support needs & directory of approved lifestyle & IAPT services • Supports culture of NHS as health as well as sickness service • Delivers part of health and employment programme • Impacts across NHS, public & private sector * QIPP = Quality, innovation, productivity, and prevention ** Initiatives should be quality-neutral or have a positive impact on quality • What are the main barriers for implementation? • What needs to be in place in order to implement? • What clinical engagement will be required? • Is anyone doing it already? • Lack of health & wellbeing advisors with consistent training (could be part of current role eg 2 nurses on a ward may take on this role for patients & peers) • Inconsistent provision of effective services for all 4 lifestyle factors & IAPT • Consistent definition & training for health advisers in primary & secondary care & within workplaces, inc behavioural psychology • Directory of local approved services inc. IAPT, quitting support, alcohol brief interventions, free swimming etc • Clinical support in primary & secondary care • Occupational health support • Social care support • No – this is an innovative & systematic development/alteration of health trainer role CONFIDENTIAL AND PROPRIETARY Any use of this material without specific permission of Mc. Kinsey & Company is strictly prohibited

Falls prevention Headline / Title: Falls prevention Short description: Systematic implementation of NICE falls prevention guidance, with implementation co-ordinated between health and social care. QIPP elements * • Estimated quality impact** Making it happen • Improves quality of life & reduces disability/dependency for older people • Quality of health & social care interventions improved by attending to risks of wider harm to patients • Estimated productivity impact • Potential 15% reduction in falls, preventing 2, 900 admissions, 820 fractures & 21, 500 bed days in Eo. E. • Potential £ 17 m cost savings • Is it linked to the prevention agenda (if at all)? • Prevents exacerbation of ill health & maintains mobility & quality of life. • What innovation is required (if any)? • This is doing what we already know works but we don’t systematically implement. • Innovation may be in engaging across health, social & third sectors to implement programmes. • Are there additional effects on the system? • Reductions in costs of social care, attendance allowances, impact on carers and other support requirements * QIPP = Quality, innovation, productivity, and prevention ** Initiatives should be quality-neutral or have a positive impact on quality • What are the main barriers for implementation? • What needs to be in place in order to implement? • What clinical engagement will be required? • Is anyone doing it already? • Recognition of the potential impact • Prioritisation of reducing disability in older people • Leadership within PCT & co-ordination of approach across health & social care • Training & capacity for falls risk assessments of community health & social care professionals • Relevant clinical programme boards • Physicians in care of elderly • GPs, community nurses, social care professionals • SW Essex PCT & some others • Not systematic across all our services. CONFIDENTIAL AND PROPRIETARY Any use of this material without specific permission of Mc. Kinsey & Company is strictly prohibited
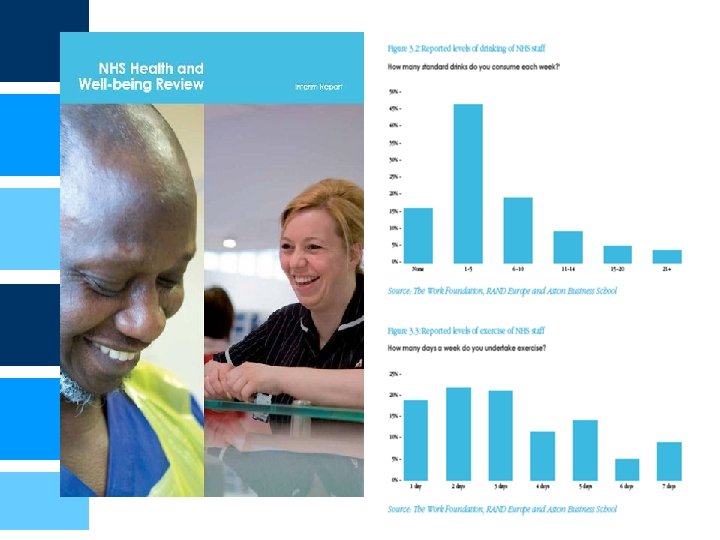

Benefits of improving health & wellbeing at work

31 While most of the potential comes from GPs and pharmacies, there are large discrepancies in the performance of individual players GPs - Nr of referrals to PSSS and in-house service /Nr smokers in practice in 2008, Percent Top quartile Average today is 7% Bottom 3 quartile Bottom of first quartile is 10% If all reached bottom first quartile, average would be 12% 14/05/0 14/05/0 14/05/0 14/05/0 14/05/0 14/05/0 14/05/0 9 9 9 9 9 9 9 Pharmacies - Nr of smokers setting a quit date/Full time advisor over 12 months Average today is 33 Bottom of first quartile is 37 If all reached bottom first quartile, average would be 45 14/05/0 14/05/0 14/05/0 14/05/0 14/05/0 14/05/0 14/05/0 9 9 9 9 9 9 9 24 SOURCE: PSSS data: practice and pharmacy profiles, Smoking. Cessation 2008, Team Analysis

328 There is a real opportunity to increase the number of quitters by engaging selected staff populations and improving the quality of the interventions Potential to increase the number of quitters per year, Peterborough Bases for impact calculation: ▪ GP practices: all reach minimum referrals levels achieved by practices in first quartile ▪ Pharmacy staff : all reach minimum ‘set quit date/advisor’ levels achieved by pharmacies in first quartile ▪ Midwives: refer 1 smoking mother out of 2 to the local stop smoking service (vs. less than 1 in 4 today) ▪ Nurses on other hospital wards: refer 40% of smoking patients to Stop smoking service, i. e. 8 patient per month per 25 bed ward or ~1 referral per staff per quarter (vs. 0. 5 referral per staff per year today) ▪ Stop Smoking Service: Self referrals increasing by 50% (from 30 to 45 referrals per month) due to increased public awareness (halo effect) 14/05/09 Today 4 weeks quitters 14/05/09 GPs 14/05/09 Hospitals* Increase Quality of Interven Increase Quantity -tions of interventions Pharmacies Potential 4 weeks quitters * Includes midwifes, staff on in-patient wards and self referrals to local stop smoking service SOURCE: Team analysis based on Peterborough Stop Smoking Service data 25

Eo. E FREE OF DEBT

What do I hope for from the DPH and their teams? • Source of objective advice – Based on agreed policy objectives, needs assessment and evidence • Promotion of the wider health agenda – As a role for the NHS – As a role for local authorities – Illustrating the need to work across the public sector • Monitoring effectiveness • Taking responsibility for delivering health outcomes • Corporacy – able to deliver through current priority programmes (eg QIPP) • Able to react effectively to new problems (eg swine flu)

Able to manage a programme of change
 • • Create")
Key elements of our approach 8 steps leading to change (Kotter) • • Create a sense of urgency Develop a vision for the future Develop a powerful “guiding coalition” Communicate the vision Share the problem widely Empower people to act Get some short term wins Institutionalise the change

How can we do better? • Better co-ordination of evidence & policy at central government level (IST model) • New framework for integrated commissioning at a PCT/LA level • NHS culture change to a stronger health as well as sickness treatment service • New vision for primary care & general practice • Incentives need better alignment • Use of language

367f12f3c6b1c845be311b6e0a48c028.ppt