the breast.ppt
- Количество слайдов: 71



THE BREAST Dr. JAMIL SAWAKED

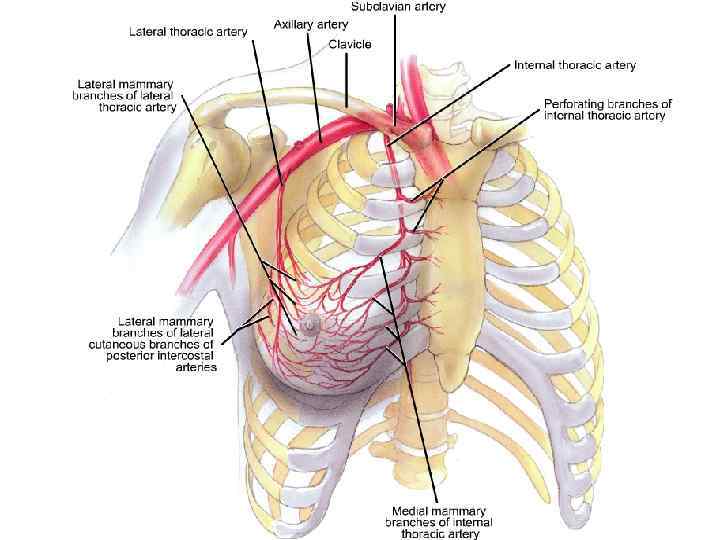
ANATOMY BREAST TAIL TERES MAJOR LATISSIMUS DORSI SERRATUS ANTER

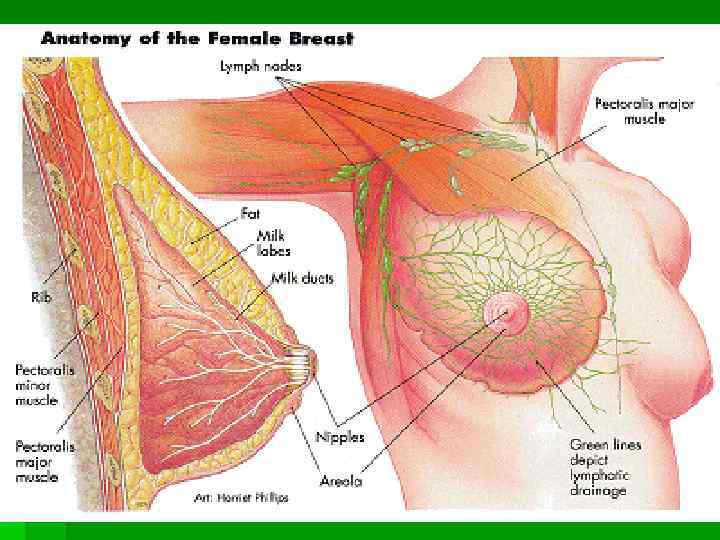
FAT LOBE MAJOR LACT. DUCT IS THE SITE OF DUCTAL CA. RIBS &intercost. m AMPULLA PECTORALIS MAJOR 20 MAJOR LACT. ORIFICES LACTOCYTE

THEIR CONTRACTION CAUSES SKIN DIMPLING PEAU d`ORANGE IS DUE TO OEDEMA OF SKIN LYMPHATIC

DUCT SYSTEM MAJOR DUCT Is the site of ductal Ca
![[MINOR] OR [ TERMINAL] MINOR DUCT IS THE SITE OF LOBULAR CARCINOMA](https://present5.com/presentation/196847023_164720123/image-6.jpg "[MINOR] OR [ TERMINAL] MINOR DUCT IS THE SITE OF LOBULAR CARCINOMA")
[MINOR] OR [ TERMINAL] MINOR DUCT IS THE SITE OF LOBULAR CARCINOMA
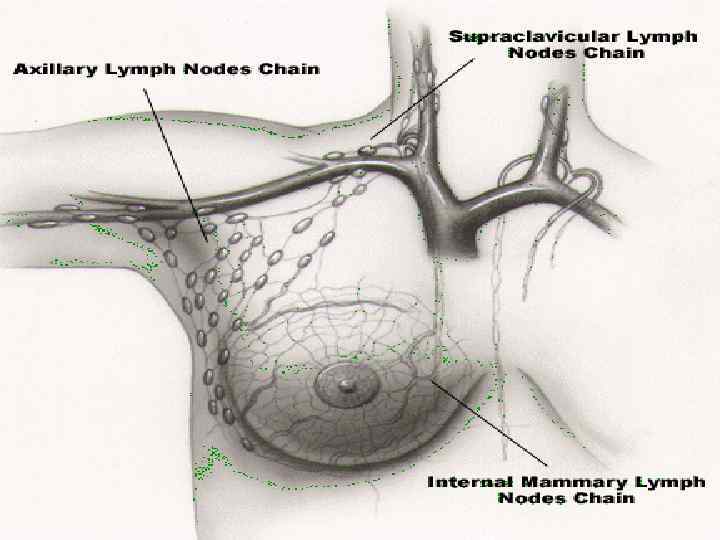

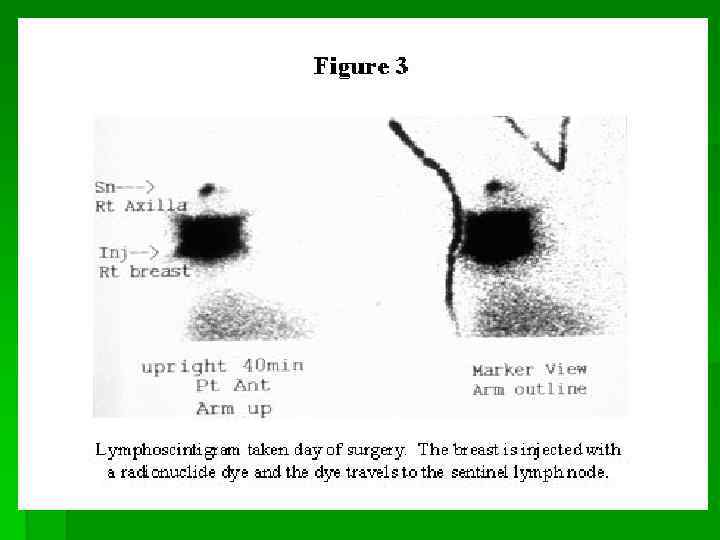
APICAL CENTRAL LATERAL SUBSCAP. V RPOSTERIO PECTORAL LAT. THOR. V SENTINEL L. N LONG THORACIC N 85% OF THE BREAST DRAIN INTO THE AXILLA SUPERIOR THORACIC V. INTERNAL MAMMARY L. N.

IF IT IS FILLED WITH MILK IT IS GALACTOCELE
![MASTITIS; PLUGGED DUCT OR CRACKED NIPPLE, [STAPHYLLOCOCCI] ABSCESS](https://present5.com/presentation/196847023_164720123/image-12.jpg "MASTITIS; PLUGGED DUCT OR CRACKED NIPPLE, [STAPHYLLOCOCCI] ABSCESS")
MASTITIS; PLUGGED DUCT OR CRACKED NIPPLE, [STAPHYLLOCOCCI] ABSCESS

60% OF MASTITIS IS IN LACTATIG WOMEN

TYPES OF MASTITIS § § § § MASTITIS NEONATORUM MASTITIS OF PUBERTY LACTATING MASTITIS SPECIFIC MASTITIS; 1 -T. B MASTITIS 2 -SYPHILITIC MASTITIS 3 -ACTINMYCOSIS

BENIGN BREAST DISEASE § § § FIBROADENOMA FIBROCYSTIC DIS DUCTECTASIA BENIGN CYSTS LIPOMA: VERY RARE [DANGEROUS TO DIAGNOSE LIPOMA]

FIBROADENOMA BREAST MOUSE SMALL ONES COULD BE LEFT ALONE

Giant fibroadenoma> 5 CM CAN BECOME MALIGNANT

DUCTECTASIA with milk fistula Treatment; like fistula in ano

WHEN A BENIGN BREAST DISEASE BECOMES WORRYING? § WHEN A PATHOLOGY SPECIMEN SHOWS ATYPICAL HYPERPLASIA § FLORID HYREPLASIA CARRIES AMILD RISK § NB; METAPLASIA AND MILD HYPERPLASIA CARRY NO RISK

CYSTS § BENIGN § MALIGNANT MANAGEMENT OF A CYST ASPIRATE & OPERATE OR CORE BIOPSY IF; 1 -BLOODY ASPIRATE 2 -DID NOT DISAPPEAR COMPLETELY AFTER ASPIRATION 3 -RECURES IN 6 WEEKS 4 -US SHOWS SOFT TISSUE INSIDE

NIPPLE DISCHARGE § I=NONBLOODY; 1 -FIBROCYSTIC DISEASE 2 -DUCTECTASIA § II=BLOODY; 1 -DUCT PAPILLOMA; MOST COMMON 2 -DUCT ECTASIA; VERY COMMON 3 -DUCT CARCINOMA; VERY RARE

BLOODY NIPPLE DISCHARGE

NORMAL DUCT PAPILLOMA

MICRODOCHECTOMY FOR BLEEDING NIPPLE BLEEDING SEGMENT IS REMOVED AND SUBMITTED TO HISTOPATHOLOGY PROBE DETERMINE FIRST WHICH ORIFICE OR SEGMENT IS BLEEDING BY PRESSING AROUND THE AREOLA
![BREAST CANCER 1. 2. 3. 4. 5. DUCTAL CARCINOMA [90%] LOBULAR CARCINOMA[<10%] PAGET`S DISEASE](https://present5.com/presentation/196847023_164720123/image-25.jpg "BREAST CANCER 1. 2. 3. 4. 5. DUCTAL CARCINOMA [90%] LOBULAR CARCINOMA[<10%] PAGET`S DISEASE")
BREAST CANCER 1. 2. 3. 4. 5. DUCTAL CARCINOMA [90%] LOBULAR CARCINOMA[<10%] PAGET`S DISEASE INTRACYSTIC PAPILLIFEROUS CA SARCOMA

What Are the Risk Factors for Breast Cancer? § 1 -Age; INCREASING AGE § 25: 1/20, 000. 45: 1/100. 50: 1/50. 55: 1/33. 60: 1/24. 80: 1/10. 2 -Race; WHITE++. RARE IN JAPAN, § 2 -Race; WHITE++. RAREhistory of breast cancer 3 -Individual or family IN JAPAN, § 3 -Individual or family history of breast cancer § 4 -A history of ovarian cancer § 4 -AA genetic predisposition (mutations to the BRCA 1 or § 5 - history of ovarian cancer § 5 -A genetic predispositionto 3% of all breast cancers) BRCA 2 genes cause 2% (mutations to the BRCA 1 or BRCA 2 genesexposure; MENARHE, MENOPAUSE § 6 -Estrogen cause 2% to 3% of all breast cancers) § 6 -Estrogen exposure; MENARHE, MENOPAUSE § 7 -Atypical hyperplasia of the breast § 8 -Lobular carcinoma in situ (LCIS) § 9 -Lifestyle factors (obesity, lack of exercise, alcohol use) § 10 -Radiation
![About 15%? [3 -15]of breast cancers are inherited Approximately 80% of hereditary breast cancer](https://present5.com/presentation/196847023_164720123/image-27.jpg "About 15%? [3 -15]of breast cancers are inherited Approximately 80% of hereditary breast cancer")
About 15%? [3 -15]of breast cancers are inherited Approximately 80% of hereditary breast cancer is caused by mutations in the BRCA 1 or BRCA 2 genes. P 53 has a role too Women who inherit a BRCA mutation have a 50% to 85% chance of developing breast cancer in their lifetime Women with especially strong family history may consider preventive surgery to remove breast tissue and/or chemoprevention Several other genetic syndromes can increase breast cancer risk

What Are the Symptoms of Breast Cancer? § New lumps or a thickening in the breast or under the arm § Nipple tenderness, discharge, or physical changes § Skin irritation or changes, such as puckers, dimples, scaliness, or new creases § Warm, red, swollen breasts with a rash resembling the skin of an orange § Pain in the breast (usually not a symptom of breast cancer, but should be reported to a doctor) No visible or obvious symptoms (asymptomatic)

SITES LT. BREAST 12% 60% 12% 6% 10% RT. LT. 60 60 6 6

MODE OF SPREAD OF DUCTAL CARCINOMA § LOCAL § LYMPHATIC § BLOOD; BONE 1 -LUMBER V. 2 -FEMUR 3 -THORAC V. 4 -RIBS 5 -SKULL SOFT TISSUE 1 -LIVER 2 -LUNG 3 -BRAIN 4 -KIDNEY 5 -ADRENALS

DIAGNOSIS § § § TRIPLE ASSESSMENT 1 -CLINICAL: A-AGE. B-EXAMINATION 2 -IMAGING : A-US. B-MAMMOGRAM 3 -PATHOLOGY: A-FNA. B-CORECUT
![FNA & CORECUT § FNA [CYTOLOGY EXAMINATION] HAS 5% FALSE –VE MOSTLY DUE TO](https://present5.com/presentation/196847023_164720123/image-32.jpg "FNA & CORECUT § FNA [CYTOLOGY EXAMINATION] HAS 5% FALSE –VE MOSTLY DUE TO")
FNA & CORECUT § FNA [CYTOLOGY EXAMINATION] HAS 5% FALSE –VE MOSTLY DUE TO SAMPLING ERROR § CORECUT [TRUCUT] IS A TISSUE HISTOPATHOLOGY THAT IS MORE ACCURATE AND TELLS YOU ABOUT THE GRADE & INVASIVENESS; INSITU OR INVASIVE
![MAMMOGRAM MALIGNANT § 1 -CALCIFICATION; CLUSTER[5 -6] OF BRANCHED FINE MICROCALCIFICATION § 2 -ARCHITECTURAL](https://present5.com/presentation/196847023_164720123/image-33.jpg "MAMMOGRAM MALIGNANT § 1 -CALCIFICATION; CLUSTER[5 -6] OF BRANCHED FINE MICROCALCIFICATION § 2 -ARCHITECTURAL")
MAMMOGRAM MALIGNANT § 1 -CALCIFICATION; CLUSTER[5 -6] OF BRANCHED FINE MICROCALCIFICATION § 2 -ARCHITECTURAL CHANGES; SPIKY DENSE IRREGULAR MASS BENIGN WELL DEFINED ROUNDED MASS WITH HALO SIGN; CYST, FIBROADENOMA

MAMMOGRAM CONVENTIONAL & DIGITAL § IT IS NON USED FOR YOUNGER WOMEN<35 YEARS, BECAUSE THEIR DENSE BREAST TISSUE GIVES FALSE POSITIVE RESULTS § BUT IT IS GOOD FOR THE SOFT BREASTS; BECAUSE THE GLANDULAR TISSUE IS SEPERATED BY FAT PLANES

Ca. breast with peau d`orange

CA BREAST; MAMMOGRAM

FIBROADENOMA ON MAMMOGRAM

MRI IS THE MOST SENSITIVE 1 - CAN PICK UP CARCINOMA IN-SITU 2 - DIFFERENTIATES BETWEEN LOCAL RECURRENCE AND FIBROSIS

MRI § NO RADIATION BUT MAGNETIC FIELD § 1 -CAN VISUALIZE A PALPAPABLE MASS WHICH IS NOT Seen ON US OR MAMMOGRAM § 2 -CAN BE USEFUL IN YOUNG WOMEN § 3 -CAN LOCATE BREAST CANCER WITH AXILLARY L. N. METS BUT BREAST FREE ON US OR MAMMOGRAM § 4 -CAN DETECT MULTICENTRIC LESION § 5 -CAN DIFFERENTIATE BETWEEN RECURRENCE AND FIBROUS TISSUE § 6 -CAN DETECT SILICON LEAK § DISADVANTAGES § 1 -CANNOT DETECT CALCIFICATIONS § UBOS: UNIDETIFIED BRIGHT OBJECTS § DISLODGE CERTAIN METALS; PACEMAKER § EXPENSIVE
![POSITRON EMISSION MAMMOGRAM SHOWS [MULTIFOCAL LESION]](https://present5.com/presentation/196847023_164720123/image-40.jpg "POSITRON EMISSION MAMMOGRAM SHOWS [MULTIFOCAL LESION]")
POSITRON EMISSION MAMMOGRAM SHOWS [MULTIFOCAL LESION]

RETRACTED BREAST

SWOLLEN BREAST WITH NIPPLE RETRACTION

MULTIPLE LOCAL RECURRENCE CANCER EN-CUIRASSE ﺩﺭﻉ ﺍﻟﻤﺤﺎﺭﺏ


HOEDEMA CAN BE COMPLICATED BY LYMPHANGIOSARCOMA MBINATION OF SURGERY &RADIOTHERAPY ON THE AXILLA CAN CAUSE THIS

Axillary venous thrombosis in ca. breast

DIFF. DIAGNOSIS OF MASTITIS & MASTITIS CARCINOMATOSA § § § § § MASTITIS CARCINOMATOSA [INFLAMMATORY CARCINOMA] IS THE MOST MALIGNANT OF ALL BR. CA. MASTECTOMY IS RARELY INDICATED BECAUSE IT IS LATE NO CONSTITUTIONAL SYMPTOMS NO FEVER NO LEUCOCYTOSIS SKIN OEDEMA > 1/3 OF THE BREAST IN BOTH ; THE BREAST IS WARM, TENDER BOTH OCCUR IN CHILD BEARING PERIOD DIFFICULT TO DISTINGUISH SOMETIMES EXCEPT BY CORECUT BIOPSY. US & MAMMOGRAM ARE USELESS BECAUSE THERE IS NO MASS

DIFF. DIAGNOSIS OF PAGET`S DISEASE &ECZEMA OF THE NIPPLE § § § PAGET`S DISEASE THERE IS AN UNDERLYING BREAST CANCER UNILATERAL NIPPLE DESTRUCTION BOUNDRIES OF THE LESION IS WELL DEMARKATED DOES NOT RESPOND TO STEROID LOCAL THERAPY

PAGET`S DISEASE OF THE BREAST

PAGET`S DISEASE OF THE BREAST

LOBULAR CARCINOMA • ARISE FROM THE TERMINAL DUCTS • COULD BE MULTIFOCAL & BILATERAL IN 20% OF CASES • IN UNILATERAL CASES ALWAYS WATCH THE OTHER BREAST • LCIS DOES NOT NEED FURTHER ACTION EXCEPT CAREFUL F. U

Carcinoma in pregnancy § § § THEY ARE DIAGNOSED LATE THEY BEHAVE THE SAME AS NON-PREGN. THEY ARE TREATED THE SAME NO BREAST CONSERVING SURGERY NO RADIOTHERAPY; TERATOGENIC NO CHEMOTHERAPY IN THE FIRST TRIMESTER § NO HORMONAL THERAPY; BECAUSE THEY ARE HORMONE RECEPT. -VE

STAGES OF CA. BREAST CIS I I II III STAGE 0 CARCINOMA TU CONFINED TO BASEMENT MEMBRANE. MASS<2 CM. MASS 2 -5 CM. MOB. L. N NO L. N. MASS 5 -10 CM. FIX. L. N OR MASS FIXED TO CHEST WALL NON INVASIVE. CLINICALLY; IMPALPABLE IV SUPRACLAV. L. N. OR DISTANT METS
![INVESTIGATIONS FOR DISTANT METASTASIS § BLOOD S. ALK. PHOSPHATASE GGT[Gamma Glutamin Transferase] § RADIOLOGY](https://present5.com/presentation/196847023_164720123/image-54.jpg "INVESTIGATIONS FOR DISTANT METASTASIS § BLOOD S. ALK. PHOSPHATASE GGT[Gamma Glutamin Transferase] § RADIOLOGY")
INVESTIGATIONS FOR DISTANT METASTASIS § BLOOD S. ALK. PHOSPHATASE GGT[Gamma Glutamin Transferase] § RADIOLOGY CXR US; Liver § NUCLEAR ISOTOPE BONE SCAN

WHAT DOES STAGING MEAN § STAGE I & II : EARLY BREAST CANCER [POTENTIALLY CURABLE DISEASE] § STAGE III & IV : ADVANCED CANCER [INCURABLE DISEASE]

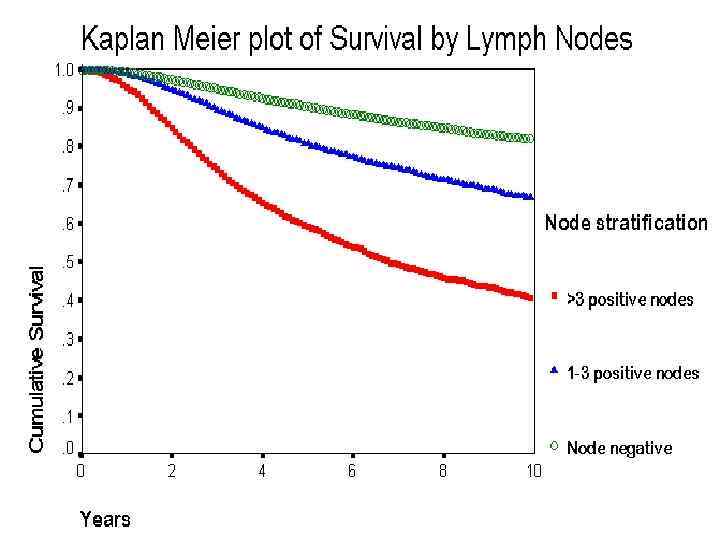
WHAT IS THE MOST SIGNIFICANT PROGNOSTIC FACTOR ? § AXILLARY LYMPH NODES INVOLVEMENT & NUMBER; IS THE MOST § NO L. N; 85% 5 -YEAR SURVIVAL § 3 L. N. ; 50% § >3 L. N. : 25 -40% § OTHER FACTORS § GRADE, -VE HORMONE RECEPTORS, SIZE, VASCULAR&LYMPH. INVASION, HER 2; EPIDERMAL GROWTH FACTOR RECEPTOR

MANAGEMENT OF EARLY BREAST CANCER § BREAST CONSERVING SURGERY: WIDE LOCAL EXCISION + AXILLARY CLEARANCE+ LOCAL BREAST RADIOTHERAPY PROVIDED MASS BREAST RELATION IS ACCEPTABLE

INDICATIONS OF MODIFIED RADICAL MASTECTOMY 1. BIG SIZE TUMOUR IN REALATION TO THE BREAST 2. CENTRAL TUMOUR; UNDER THE NIPPLE 3. MULTIFOCAL TUMOUR 4. RECURRENCE AFTER LUMPECTOMY 5 IN PREGNANCY 6. PATIENT`S PREFERENCE

WHAT IS MODIFIED RADICAL MASTECTOMY ? : simple mastectomy + axillary clearance LONG THORACIC N. SHOULD BE PRESERVED INTERCOSTOBRACHIAL N. CAN BE SACRIFIED Apical CENTRAL Lateral Ax. VEIN POSTERIOR INTERPECTORAL

Axillary clearance of l. nodes Modified radical mastectomy Breast conserving surgery

WHAT IS THE DIFFERENCE BETWEEN THE 2 § NO DIFFERENCE IN 5 -YEAR SURVIVAL § THERE IS A DIFFERENCE IN LOCAL RECURRENCE § RECURRENCE AFTER LUMPECTOMY IS MORE. TREATED BY MASTECTOMY AND THEY DO BETTER

THE OTHER MODALITIES § CHEMOTHERAPY; == CMF == 1 -ADJUVANT & 2 -NEOADJUVANT § HORMONAL THERAPY; TAMOXIFEN: OESTROGEN BLOCKER LHRH : OVARIAN ABLATION IN the young ANASTROZOLE: AROMATASE INHIBITOR INHIBIT CONVERSION OF ANROGENS TO OESTROGEN In the postmenopausal women § IMMUNE THERAPY; HERCEPTIN [monoclonal antibody ; Anti HER 2, Human Epidermal Growth Factor Receptor ] § RADIOTHERAPY; LOCAL ACTION
![Port-a-cath for systemic chemotherapy Chemotherapy kills all dividing cells [malignant or not malignant]. so](https://present5.com/presentation/196847023_164720123/image-66.jpg "Port-a-cath for systemic chemotherapy Chemotherapy kills all dividing cells [malignant or not malignant]. so")
Port-a-cath for systemic chemotherapy Chemotherapy kills all dividing cells [malignant or not malignant]. so bone marrow GIT and skin are affected.

HOW TO EXAMINE YOUR OWN BREASTS TEACH PATIENT OK AT MIRROR NOTE ANY ABNORMALITY IN YOUR BREASTS OR AXILLAE AT EVERY SHOWER

USE PALMER ASPECTS OF YOUR FINGERS USE PALMER ASPECTS OF

gynecomastia

MALE BREAST CANCER

MALE BREAST CANCER
the breast.ppt