097b61b5ea17729dcef7af24e41099ac.ppt
- Количество слайдов: 30



Thames Valley review of rehabilitation services for patients diagnosed with head and neck cancer following treatment Siân Lewis Macmillan Clinical Lead Dietitian 24 th February 2016

Rehabilitation • To restore a patient’s roles and functions as far as possible, and help them to adjust to limitations where required (Cancer Taskforce 2015) • Focus is primarily rehabilitation services - dietetics, nursing, psychology, occupational therapy, restorative dentistry, SLTs and physiotherapy - To ensure prudent healthcare and co-production a multi -disciplinary team approach led by the surgeons and oncologists is paramount

Project background 2012: • Concerns were formally raised regarding the overall current provider capacity to deliver a service to meet HNC patient’s demands and be compliant with national guidelines • Patients felt there was a lack of specialist workforce in restorative dentistry and AHPs such as dietetics and SLTs • SCN approached Macmillan for funding towards a major scoping project

Achieving world-class cancer outcomes Cancer Taskforce 2015 How should we improve the QOL of patients after treatment & at end of life? • Recommendation 63: The NHS and partners should drive forward a programme of work to ensure that people living with and beyond cancer are fully supported and their needs are met. • Recommendation 65: NHS England should accelerate the commissioning of services for patients living with and beyond cancer, with a view to ensuring that every person with cancer has access to the elements of the Recovery Package by 2020 • Recommendation 67: NHS England should pilot stratified follow-up pathways of care for other tumour types

Cancer of the UAT NICE 2016 Follow up • Ensure people with cancer of the upper aerodigestive tract and their carers have tailored information about the symptoms of recurrence and late effects of treatment at the end of curative therapy • Consider structured, risk‑adapted follow‑up using locally‑agreed protocols for people who have had curative treatment for cancer of the upper aerodigestive tract. Use the follow‑up protocols to: - Help improve QOL, including discussing psychological issues - Detect disease recurrence or second primary cancer

Aims & Objectives Aim: The main aim of the scoping project is to identify and understand key areas within the rehabilitation services for HNC patients where the support and care is not met and needs enhancement

Aims & Objectives: • Identify the number of HNC patients • Map current services for HNC patients within the network • Identify gaps in current service provision • Identify models for service development to support HNC patients • Identify staff involved with HNC patients and their needs

Incidence of new cases of HNC in Thames Valley SCN National Cancer Registration Service 2015 Tumour site Number of new cases of HNC diagnosed per annum 2011 2012 2013 Lip, tongue & oral cavity 156 152 148 Salivary glands 24 28 41 Pharynx & tonsil 75 83 89 Nose, ear, sinus & larynx 86 104 88 Total 341 367 366

CCG Number of new cases of HNC diagnosed per annum 2011 2012 2013 NHS Aylesbury Vale 34 22 27 NHS Bracknell & Ascot 16 18 14 NHS Chiltern 38 51 37 NHS Milton Keynes 37 36 33 NHS Newbury & District 13 19 22 NHS North & West Reading 15 16 20 NHS Oxfordshire 97 93 98 NHS Slough 11 15 19 NHS South Reading 13 9 14 NHS Swindon 35 34 36 NHS Windsor, Ascot & Maidenhead 11 28 21 NHS Wokingham 21 26 25 Total 341 367 366

Methodology Main activities conducted: • Mapping of current services within the network and identification of gaps • Patient experience using focus and support groups • Education and training needs of the workforce • Recommendations

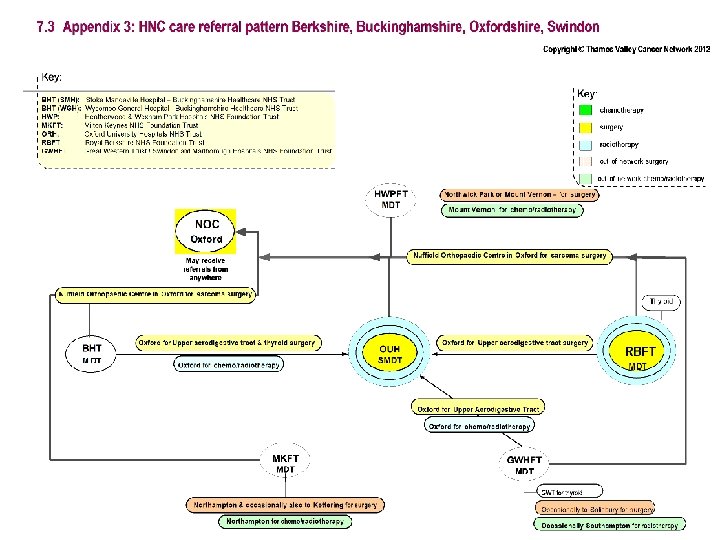
Mapping current services

1. Great Western Hospital 2. Milton Keynes Hospital 3. Churchill Hospital 4. Royal Berkshire Hospital 5. Stoke Mandeville Hospital 6. Wexham Hospital 7. Wycombe Hospital NHS Milton Keynes CCG 2 NHS Aylesbury Vale CCG 5 NHS Oxfordshire CCG 3 7 NHS Chiltern CCG NHS Swindon CCG 1 NHS Winsdor , Ascot & Maidenhead CCG NHS Newbury & District CCG NHS South Reading CCG NHS North & West Reading CCG 4 NHS Bracknell Wokingham CCG& Ascot CCG 6 NHS Slough CCG

NCAT workforce mapping tool

Main findings • Limited access to MDT post treatment • HNA not being completed due to time constraints • Variation in services across the network • Data activity supports development of pay band 4 role

General Practitioners: • Rehabilitation services should be provided by cancer centres/ units - Skills & expertise - Access to members of MDT • End of Treatment summary could be used as education tool • Use of modern technology - Internet - Mobile phones - Videoconferencing

Patient experiences

Findings • High praise from patients and their carers for the care they had received during their treatment • Lack of access or delays with referrals to some rehabilitation services such as SLT, physiotherapy, dentistry and psychology - some patients accessed services privately • Lack of restorative dental services - lack of dental staff, waiting times for treatment and location of services • Local support groups seem invaluable - provided additional psychological and emotional support • Laryngectomy patients report some difficulty in accessing SLT services - standard approach in prosthesis replacement across the network

• Need to be provided with more information regarding side effects of treatment and specific HNC services • Some patients felt that an EOT meeting which included a holistic assessment and provision of information specific to them would be beneficial • H & WB events were valued - carers felt that they were included • Patients valued texting service - ease of communication with CNS during periods of speech difficulties • Milton Keynes: - Highly valued the support and care provided by SLT and community dietitians - Significant lack of co-ordinated services, access to rehabilitative services and communication

Education & training needs of workforce

Findings • Overall response rate for the questionnaire was 78% • Highest response rate was by dietitian and SLTs, lowest was OT • Majority of education was in the form of self-directed learning • 69% felt that their education and training needs not met • Top three priorities: - Opportunities to work across network - HNC specific training - Improved psychology, counselling and communication training

Recommendations

Hub and Spoke Model

Version A • One team providing after care services: - Attached to hub and hosted by OUH - Regular rehabilitation OPCs to spokes • Team would consist of: - Care coordinator - CNS - Dietitian - SLT - Musculoskeletal physiotherapist

Version B • Increase in workforce at each spoke: - CNS - Dietitians - SLT - Access to musculoskeletal physiotherapist • AHP rehabilitation clinic in conjunction with local medical review

Version C • Hybrid of version A and B • Three community teams each covering two localities - Locality Team 1: OUH and GWHT - Locality Team 2: RBH and FHFT - Locality Team 3: BHT and MKH - Access to musculoskeletal physiotherapist • Each team would consist of a CNS, Dietitian, SLT and access to musculoskeletal physiotherapist • AHP rehabilitation clinic in conjunction with local medical review and local H&WB events

Summary • Patients should be offered stratified follow-up pathways • Development of local specialist HNC teams • Increase rehabilitation staff at cancer units • Development of the pay band 4 role within cancer centres • Increase restorative dentistry services • Better access to physiotherapy, lymphoedema and OT services • Develop and implement a programme of new learning opportunities and ensure protected time

Acknowledgements • Steering group • Kim Bowles • Nick Crowson-Towers • Dr. Richard Fisher • Sam Penney • Helen Petley • Mr. Priy Silva • Allan Warnock • All staff and patients who helped and contributed to the project

097b61b5ea17729dcef7af24e41099ac.ppt