73c3f8efa810f982bc6fe891df654b0a.ppt
- Количество слайдов: 77
 TESTOSTERONE REPLACEMENT THERAPY -A RECIPE FOR SUCCESS- --John Crisler, DO Lansing, MI USA MSU-COM www. All. Things. Male. com
TESTOSTERONE REPLACEMENT THERAPY -A RECIPE FOR SUCCESS- --John Crisler, DO Lansing, MI USA MSU-COM www. All. Things. Male. com
 “Everything You Always Wanted to Know About TRT But Didn’t Have Time to Ask”
“Everything You Always Wanted to Know About TRT But Didn’t Have Time to Ask”
 WHAT IS TESTOSTERONE REPLACEMENT THERAPY?
WHAT IS TESTOSTERONE REPLACEMENT THERAPY?
 TRT: Restoration of Testosterone to HEALTHY physiological levels.
TRT: Restoration of Testosterone to HEALTHY physiological levels.
 TRT is NOT: § Total T>normal range § Steroids § Viagra
TRT is NOT: § Total T>normal range § Steroids § Viagra
 SCREENING FOR HYPOGONADISM
SCREENING FOR HYPOGONADISM
 WHAT ARE THE SYMPTOMS OF LOW TESTOSTERONE? § § § TAT Syndrome Fatigue USTA Syndrome Loss of muscle mass Fat gain Poor recovery § § § Pain/Inflammation Irritability Depression Decreased memory Loss of Libido Erectile Dysfunction
WHAT ARE THE SYMPTOMS OF LOW TESTOSTERONE? § § § TAT Syndrome Fatigue USTA Syndrome Loss of muscle mass Fat gain Poor recovery § § § Pain/Inflammation Irritability Depression Decreased memory Loss of Libido Erectile Dysfunction
 ADAM Questionnaire 1. Do you have a decrease in sex drive? 2. Do you have a lack of energy? 3. Do you have a decrease in strength and/or endurance? 4. Have you lost height? 5. Have you noticed a decreased enjoyment of life?
ADAM Questionnaire 1. Do you have a decrease in sex drive? 2. Do you have a lack of energy? 3. Do you have a decrease in strength and/or endurance? 4. Have you lost height? 5. Have you noticed a decreased enjoyment of life?
 6. Are you sad and/or grumpy? 7. Are your erections less") ADAM Questionnaire (con’t) 6. Are you sad and/or grumpy? 7. Are your erections less strong? 8. Has it been more difficult to maintain your erection throughout sexual intercourse? 9. Are you falling asleep after dinner? 10. Has your work performance deteriorated recently?
ADAM Questionnaire (con’t) 6. Are you sad and/or grumpy? 7. Are your erections less strong? 8. Has it been more difficult to maintain your erection throughout sexual intercourse? 9. Are you falling asleep after dinner? 10. Has your work performance deteriorated recently?
 INITIAL LAB WORK
INITIAL LAB WORK
 INITIAL HYPOGONADISM PANEL § § § § § Total Testosterone § Bioavailable/Free T SHBG § DHT (? ) LH/FSH § DHEA-S Estradiol § Total Estrogens (urine) § Prolactin § Cortisol Thyroid Panel (TSH, FT 4, FT 3) Comp Metabolic Panel CBC Lipid Panel PSA (if over 40) Progesterone
INITIAL HYPOGONADISM PANEL § § § § § Total Testosterone § Bioavailable/Free T SHBG § DHT (? ) LH/FSH § DHEA-S Estradiol § Total Estrogens (urine) § Prolactin § Cortisol Thyroid Panel (TSH, FT 4, FT 3) Comp Metabolic Panel CBC Lipid Panel PSA (if over 40) Progesterone
 §") MEASURES OF TESTOSTERONE § Total Testosterone—all that is produced (300 -1000 ng/d. L) § Free Testosterone—all that is unbound (2 -4%) (80 -300 pg/d. L) --Equilibrium Dialysis, NOT RIA! § Bioavailable Testosterone—Gold Standard “Free and Loosely/Weakly Bound” 40 -60% (120 -600 ng/d. L)
MEASURES OF TESTOSTERONE § Total Testosterone—all that is produced (300 -1000 ng/d. L) § Free Testosterone—all that is unbound (2 -4%) (80 -300 pg/d. L) --Equilibrium Dialysis, NOT RIA! § Bioavailable Testosterone—Gold Standard “Free and Loosely/Weakly Bound” 40 -60% (120 -600 ng/d. L)
 “Laboratory reference values for testosterone vary widely, and are established without clinical considerations. ” Lazarou S, et al. Harvard Medical School, Division of Urology, Beth Israel Deaconess Medical Center
“Laboratory reference values for testosterone vary widely, and are established without clinical considerations. ” Lazarou S, et al. Harvard Medical School, Division of Urology, Beth Israel Deaconess Medical Center
 § Refrigerated, no additive serum preferred (Plain, Red Top) §") T SAMPLE PREPARATION (SERUM) § Refrigerated, no additive serum preferred (Plain, Red Top) § Heparanized serum less acceptable (green-top) § NO Serum Separator Tubes (SST)
T SAMPLE PREPARATION (SERUM) § Refrigerated, no additive serum preferred (Plain, Red Top) § Heparanized serum less acceptable (green-top) § NO Serum Separator Tubes (SST)
 IMPORTANT ABOUT ESTROGEN TESTING § Total Estrogens is NOT a valid assay for adult males --cross reactivity w/ progesterone § Estradiol MUST be by “ultrasensitive” method, LC/MS assay--ALL OTHERS NOT VALID § Gold standard is 24 hour urine, esp w/ TD’s (Trans. Dermals) § Be extra mindful of SHBG level
IMPORTANT ABOUT ESTROGEN TESTING § Total Estrogens is NOT a valid assay for adult males --cross reactivity w/ progesterone § Estradiol MUST be by “ultrasensitive” method, LC/MS assay--ALL OTHERS NOT VALID § Gold standard is 24 hour urine, esp w/ TD’s (Trans. Dermals) § Be extra mindful of SHBG level
 Sample Matrixes § BLOOD --most common --Total, Free, Bioavailable --”snap shot” only --limited value given TD’s, hormone conversions, etc. § URINE --best of all, esp. w/ TD’s --”free” levels provided --limited assays --expanded hormone assay types, incl. metabolites --use only 24 hour collections—no spots --be careful of contamination --better to assess intracellular 5 -AR activity
Sample Matrixes § BLOOD --most common --Total, Free, Bioavailable --”snap shot” only --limited value given TD’s, hormone conversions, etc. § URINE --best of all, esp. w/ TD’s --”free” levels provided --limited assays --expanded hormone assay types, incl. metabolites --use only 24 hour collections—no spots --be careful of contamination --better to assess intracellular 5 -AR activity
 will be well within normal") Many times T on bloods (especially for morning draw) will be well within normal range. But when you collect a 24 hour urine, T will be deficient. Thus a spurt of T in the morning, then very little the rest of the day.
Many times T on bloods (especially for morning draw) will be well within normal range. But when you collect a 24 hour urine, T will be deficient. Thus a spurt of T in the morning, then very little the rest of the day.
 COMMON SENSE IN ORDER TO TEST THE LEVEL OF A DRUG, YOU MUST TAKE THE DRUG, ON SCHEDULE!!!
COMMON SENSE IN ORDER TO TEST THE LEVEL OF A DRUG, YOU MUST TAKE THE DRUG, ON SCHEDULE!!!
 COMMON SENSE HAVE PATIENT DRAW AT SAME TIME OF DAY EACH TIME, ESPECIALLY WITH TRANSDERMALS (b/c PK’s)
COMMON SENSE HAVE PATIENT DRAW AT SAME TIME OF DAY EACH TIME, ESPECIALLY WITH TRANSDERMALS (b/c PK’s)
 COMMON SENSE 1. NEVER SMOKE IN BED 2. ALWAYS WEAR PAJAMAS
COMMON SENSE 1. NEVER SMOKE IN BED 2. ALWAYS WEAR PAJAMAS

 DHT § Most responsible for All Things Male § 5 -AR’d from T § Unfairly deemed “evil hormone” § NOT responsible for prostate morbidity § 25 -75 ng/d. L § Serum assay valid? § Metabolite ratios on 24 hour urines best § Avoid finasteride
DHT § Most responsible for All Things Male § 5 -AR’d from T § Unfairly deemed “evil hormone” § NOT responsible for prostate morbidity § 25 -75 ng/d. L § Serum assay valid? § Metabolite ratios on 24 hour urines best § Avoid finasteride
 Estradiol § § § § Major player amongst estrogens Total Estrogens is NOT valid assay for males MUST be monitored during TRT Masks benefits of TRT Adjunctive cause of serious illness Numerous benefits for health, so… Must not be driven too low (10 -50 pg/m. L) maintain mid-range ( w/ mid-range SHBG) § May rise over time § TD’s elevate E more than IM
Estradiol § § § § Major player amongst estrogens Total Estrogens is NOT valid assay for males MUST be monitored during TRT Masks benefits of TRT Adjunctive cause of serious illness Numerous benefits for health, so… Must not be driven too low (10 -50 pg/m. L) maintain mid-range ( w/ mid-range SHBG) § May rise over time § TD’s elevate E more than IM
 § Produced by pituitary § Stimulates T production § Pulsatile production") Luteinizing Hormone (LH) § Produced by pituitary § Stimulates T production § Pulsatile production § Short half-life § Acute phase reactant § Must be careful in its interpretation § Possible Gn-secreting tumor
Luteinizing Hormone (LH) § Produced by pituitary § Stimulates T production § Pulsatile production § Short half-life § Acute phase reactant § Must be careful in its interpretation § Possible Gn-secreting tumor
 § Produced by pituitary § Spermatogenesis § 180 -240 minute") Follicle Stimulating Hormone (FSH) § Produced by pituitary § Spermatogenesis § 180 -240 minute half-life § Inhibited largely by estrogen § Better measure of gonadotrophin output? § Possible FSH-secreting tumor
Follicle Stimulating Hormone (FSH) § Produced by pituitary § Spermatogenesis § 180 -240 minute half-life § Inhibited largely by estrogen § Better measure of gonadotrophin output? § Possible FSH-secreting tumor
 Prolactin § Significant cause of hypogonadism § May signal tumor presence § Health benefits § Must be maintained within normal range § Ref Range (3. 0 -18. 0 ng/m. L) § >300= tumor § Elevated by eating, sex (<30)
Prolactin § Significant cause of hypogonadism § May signal tumor presence § Health benefits § Must be maintained within normal range § Ref Range (3. 0 -18. 0 ng/m. L) § >300= tumor § Elevated by eating, sex (<30)
 HYPERPROLACTINEMIA CAUSES § Pituitary tumor § Stalk compression § Primary hypothyroidism § Chronic renal failure § Cirrhosis § § § Opiates Tri-cyclics D 2 antagonists Metoclopramide Verapamil Chest wall trauma
HYPERPROLACTINEMIA CAUSES § Pituitary tumor § Stalk compression § Primary hypothyroidism § Chronic renal failure § Cirrhosis § § § Opiates Tri-cyclics D 2 antagonists Metoclopramide Verapamil Chest wall trauma
 Cortisol § “Stress hormone” § Cause of secondary hypogonadism § Healthful benefits § Must be maintained within normal range § If elevated: Tx’d with Phosphatidylserine (PS) (300 mg po QD) § If depressed: Tx’d with Hydrocortisone PO
Cortisol § “Stress hormone” § Cause of secondary hypogonadism § Healthful benefits § Must be maintained within normal range § If elevated: Tx’d with Phosphatidylserine (PS) (300 mg po QD) § If depressed: Tx’d with Hydrocortisone PO
 “Progesterone puts plaque in the arteries, and wrinkles in the penis” --Dr. John Crisler
“Progesterone puts plaque in the arteries, and wrinkles in the penis” --Dr. John Crisler

 T/E ratio § Measure of system performance --ratio does have importance, but… --absolute values of hormones are important --cannot elevate E without consequence as long as T is proportionately high § Used to explain pathophysiology --low T higher proportionate E morbidity § NOT to be used as treatment goal
T/E ratio § Measure of system performance --ratio does have importance, but… --absolute values of hormones are important --cannot elevate E without consequence as long as T is proportionately high § Used to explain pathophysiology --low T higher proportionate E morbidity § NOT to be used as treatment goal
 § Thyroid Panel (TSH, FT 4, FT 3) § CBC ( anemia") LABS (con’t) § Thyroid Panel (TSH, FT 4, FT 3) § CBC ( anemia mimics ↓T ) § Comprehensive Metabolic Panel § Lipid Profile § PSA (if over 40)
LABS (con’t) § Thyroid Panel (TSH, FT 4, FT 3) § CBC ( anemia mimics ↓T ) § Comprehensive Metabolic Panel § Lipid Profile § PSA (if over 40)
 TESTOSTERONE DELIVERY SYSTEMS § Gels and Creams § Patches § Implantable Pellets § IM § Orals
TESTOSTERONE DELIVERY SYSTEMS § Gels and Creams § Patches § Implantable Pellets § IM § Orals
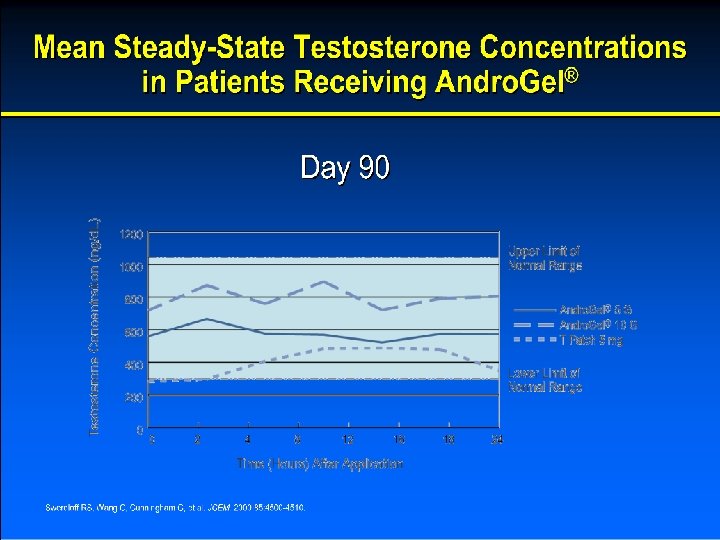
 Gels and Creams § § § Ease of application May be more convenient—OR NOT Stable across week, not day “Pulsing” [T] may be beneficial Quickly attains stable serum levels Boosts DHT May elevate estrogens Risk of accidental transferal Be mindful of application method Avoid antecubital fossa—looks like AAS use EXTREMELY variable absorption… Especially with hypothyroidism
Gels and Creams § § § Ease of application May be more convenient—OR NOT Stable across week, not day “Pulsing” [T] may be beneficial Quickly attains stable serum levels Boosts DHT May elevate estrogens Risk of accidental transferal Be mindful of application method Avoid antecubital fossa—looks like AAS use EXTREMELY variable absorption… Especially with hypothyroidism
 § “Big House” products Solvay Pharmaceuticals’ Androgel Auxilium Pharmaceuticals’ Testim") Gels and Creams (con’t) § “Big House” products Solvay Pharmaceuticals’ Androgel Auxilium Pharmaceuticals’ Testim --MUCH more expensive --support physician education (“The Cause”) --covered by insurance --vouchers/sample --1% --be mindful of application technique
Gels and Creams (con’t) § “Big House” products Solvay Pharmaceuticals’ Androgel Auxilium Pharmaceuticals’ Testim --MUCH more expensive --support physician education (“The Cause”) --covered by insurance --vouchers/sample --1% --be mindful of application technique
 § Compounded gels/creams --various bases --1%, 5%, 10, 20% --higher") Gels and Creams (con’t) § Compounded gels/creams --various bases --1%, 5%, 10, 20% --higher conc. < E, DHT conversion --soy, yam-based T’s --ALL T gels/creams are ”bio-identical” --creams slow absorption --can compound anti-E’s into product --MUCH less expensive --syringe applicators great --pumps coming onto market
Gels and Creams (con’t) § Compounded gels/creams --various bases --1%, 5%, 10, 20% --higher conc. < E, DHT conversion --soy, yam-based T’s --ALL T gels/creams are ”bio-identical” --creams slow absorption --can compound anti-E’s into product --MUCH less expensive --syringe applicators great --pumps coming onto market
 T GEL APPLICATION § Jars with measuring spoons § Plastic capped syringes § Metered Dose Pumps § 1% apply to outer arms, shoulders, flanks § 5%, 10% applied to forearms § NO scrotal application!
T GEL APPLICATION § Jars with measuring spoons § Plastic capped syringes § Metered Dose Pumps § 1% apply to outer arms, shoulders, flanks § 5%, 10% applied to forearms § NO scrotal application!
 Testosterone Patches § Convenient—MAYBE! § No risk of accidental transfer § Stable serum androgen levels § Little DHT, E boost § Scrotal patches available (WHEW!) § 2/3’s--Contact Dermatitis
Testosterone Patches § Convenient—MAYBE! § No risk of accidental transfer § Stable serum androgen levels § Little DHT, E boost § Scrotal patches available (WHEW!) § 2/3’s--Contact Dermatitis
 Testosterone Injection § Convenient—MAYBE! § MUST be injected weekly § Stable across day, not week § Ease of dose titration § Injection risks § The “Gold Standard” NO MORE!
Testosterone Injection § Convenient—MAYBE! § MUST be injected weekly § Stable across day, not week § Ease of dose titration § Injection risks § The “Gold Standard” NO MORE!
 NEEDLE SIZES § Glutes: 22 ga 1 ½” § Thighs: 25 ga 1”
NEEDLE SIZES § Glutes: 22 ga 1 ½” § Thighs: 25 ga 1”
 OTHER MEDICATIONS: § HCG --LH analog --traditional treatment-of-choice for 2 nd low T --not just “fertility drug” --best use is adjunctive to TRT --does not produce subjective benefits of T delivery § SERM’s --elevates T, but… --does not bring subjective benefits of TRT --for testing, purposes of HPTA intactness --HPTA recovery “PCT” (AAS Post Cycle Therapy) --”rescue” Tx for gynocomastia (Tamoxifen) --possible issues with respect to brain function
OTHER MEDICATIONS: § HCG --LH analog --traditional treatment-of-choice for 2 nd low T --not just “fertility drug” --best use is adjunctive to TRT --does not produce subjective benefits of T delivery § SERM’s --elevates T, but… --does not bring subjective benefits of TRT --for testing, purposes of HPTA intactness --HPTA recovery “PCT” (AAS Post Cycle Therapy) --”rescue” Tx for gynocomastia (Tamoxifen) --possible issues with respect to brain function
 § Clomiphene --racemic mixture (antagonist AND agonist) --enclomiphene+zuclomiphene --may bring untoward visual") SERM’s (con’t) § Clomiphene --racemic mixture (antagonist AND agonist) --enclomiphene+zuclomiphene --may bring untoward visual effects --may bring untoward emotional effects § Tamoxifen --pure estrogen antagonism --great for “nipple issues” --↑ progesterone receptor [conc] § Raloxifen --great estrogen antagonism --MUCH more expensive § Others (more to come)
SERM’s (con’t) § Clomiphene --racemic mixture (antagonist AND agonist) --enclomiphene+zuclomiphene --may bring untoward visual effects --may bring untoward emotional effects § Tamoxifen --pure estrogen antagonism --great for “nipple issues” --↑ progesterone receptor [conc] § Raloxifen --great estrogen antagonism --MUCH more expensive § Others (more to come)
 CONTRAINDICATIONS TO TRT: § Prostate CA § Breast CA § Untreated prolactinoma
CONTRAINDICATIONS TO TRT: § Prostate CA § Breast CA § Untreated prolactinoma
 RELATIVE CONTRAINDICATIONS: § PSA >4. 0 or accel>0. 75 § H/H> 18/55 § Sleep Apnea § Cardiac, Hepatic, Renal Dz
RELATIVE CONTRAINDICATIONS: § PSA >4. 0 or accel>0. 75 § H/H> 18/55 § Sleep Apnea § Cardiac, Hepatic, Renal Dz
 § Increased risk of bladder outlet symptoms due § § §") POTENTIAL RISKS (listed) § Increased risk of bladder outlet symptoms due § § § § to increase in prostate volume Edema in patients with preexisting cardiac, renal, or hepatic disease Gynecomastia Erythrocytosis (monitor H/H) Precipitation or worsening of sleep apnea Acne Decreased sperm production Stimulation of growth in previously undiagnosed prostate cancer
POTENTIAL RISKS (listed) § Increased risk of bladder outlet symptoms due § § § § to increase in prostate volume Edema in patients with preexisting cardiac, renal, or hepatic disease Gynecomastia Erythrocytosis (monitor H/H) Precipitation or worsening of sleep apnea Acne Decreased sperm production Stimulation of growth in previously undiagnosed prostate cancer
 DRUG INTERACTIONS: § Diabetic Medications § Propranolol § Oxyphenbutazone
DRUG INTERACTIONS: § Diabetic Medications § Propranolol § Oxyphenbutazone
 The Meat and Potatoes of TRT
The Meat and Potatoes of TRT
 § Testosterone") INITIAL DOSAGES § Transdermal gels/creams 50 mgs total QD 5 mgs (delivered) § Testosterone Cypionate IM: 100 mg QW --double dose “front load” --split weekly dose for those with anxiety issues (not initially)?
INITIAL DOSAGES § Transdermal gels/creams 50 mgs total QD 5 mgs (delivered) § Testosterone Cypionate IM: 100 mg QW --double dose “front load” --split weekly dose for those with anxiety issues (not initially)?
 FOLLOW-UP LABS § § § § § Total T Bio T LH/FSH (especially with transdermal) FSH—to back up LH interpretation of HPTA status SHBG Estradiol CBC Comp. Metabolic Panel PSA (if over 40)
FOLLOW-UP LABS § § § § § Total T Bio T LH/FSH (especially with transdermal) FSH—to back up LH interpretation of HPTA status SHBG Estradiol CBC Comp. Metabolic Panel PSA (if over 40)
 § Initial F/U at 2 weeks with TD (transdermal) --stable") FOLLOW UP LABS (con’t) § Initial F/U at 2 weeks with TD (transdermal) --stable serum T levels quickly attained --logistical consideration of 30 -day dose § Initial F/U at 6 weeks with IM --takes that long to equilibrate --interpret by PK’s of T ester (48 -72 hour peak) --cypionate/enanthate t 1/2 5 -8 days § F/U at 4 -6 weeks S/P dosage change or estrogen control s/p HPTA-suppression
FOLLOW UP LABS (con’t) § Initial F/U at 2 weeks with TD (transdermal) --stable serum T levels quickly attained --logistical consideration of 30 -day dose § Initial F/U at 6 weeks with IM --takes that long to equilibrate --interpret by PK’s of T ester (48 -72 hour peak) --cypionate/enanthate t 1/2 5 -8 days § F/U at 4 -6 weeks S/P dosage change or estrogen control s/p HPTA-suppression
 § Once dose is titrated: --q 6 months or yearly --Include") FOLLOW-UP LABS (con’t) § Once dose is titrated: --q 6 months or yearly --Include PSA --Perform Digital Rectal Exam (DRE)
FOLLOW-UP LABS (con’t) § Once dose is titrated: --q 6 months or yearly --Include PSA --Perform Digital Rectal Exam (DRE)
 TIMING OF LABS FOR IM § Cypionate, Enanthate esters peak at 48 -72 hours s/p IM injection § Decline thereafter § T 1/2=5 -8 days § No lab draw on injection day --no urines first three days § Use these facts to interpret labs
TIMING OF LABS FOR IM § Cypionate, Enanthate esters peak at 48 -72 hours s/p IM injection § Decline thereafter § T 1/2=5 -8 days § No lab draw on injection day --no urines first three days § Use these facts to interpret labs
 TIMING OF LABS FOR TD’s § Apply at same time each day § Always ask pt. when they apply (lifestyle) § Split dose? § Consider TD carrier! § Allow at least 2 hours prior to draw § 2 -4 hours is best with T gels § Above no consequence with 24 hour urines § Absorption is slowed, lost with T creams
TIMING OF LABS FOR TD’s § Apply at same time each day § Always ask pt. when they apply (lifestyle) § Split dose? § Consider TD carrier! § Allow at least 2 hours prior to draw § 2 -4 hours is best with T gels § Above no consequence with 24 hour urines § Absorption is slowed, lost with T creams
 ESTROGEN ISSUES § Do not Tx until post F/U labs --E 2 may actually DROP with TRT --insight into body’s response § Maintain E 2 at mid-range --with mid-range SHBG
ESTROGEN ISSUES § Do not Tx until post F/U labs --E 2 may actually DROP with TRT --insight into body’s response § Maintain E 2 at mid-range --with mid-range SHBG
 Detriments of Elevated Estrogen § § § Suppresses HPTA Elevates SHBG Impotence Infertility Psychological morbidities § Vasospasm § Increases clotting § § § factors Water retention Prostate morbidity Cancers Female fat distribution Fx on thyroid function ↑ “Wimpy Factor”
Detriments of Elevated Estrogen § § § Suppresses HPTA Elevates SHBG Impotence Infertility Psychological morbidities § Vasospasm § Increases clotting § § § factors Water retention Prostate morbidity Cancers Female fat distribution Fx on thyroid function ↑ “Wimpy Factor”
") ESTROGEN ELEVATORS § § § § Age Obesity ETOH overconsumption (incl HOPS in beer!) Liver Dz Zinc deficiency (50 mg Zn/2 mg Cu QD) Vitamin C deficiency Excessive DHEA supplementation (100 mg QD) § Androstenedione supplementation § Xenoestrogens (incl Vinyl IV bags!) --Lavender, Tea Tree Oil § Liver Detoxification issues § Soy § Flax seed § Foods
ESTROGEN ELEVATORS § § § § Age Obesity ETOH overconsumption (incl HOPS in beer!) Liver Dz Zinc deficiency (50 mg Zn/2 mg Cu QD) Vitamin C deficiency Excessive DHEA supplementation (100 mg QD) § Androstenedione supplementation § Xenoestrogens (incl Vinyl IV bags!) --Lavender, Tea Tree Oil § Liver Detoxification issues § Soy § Flax seed § Foods

 Inhibitor § Competitive Inhibitor § #1 use of this") ANASTROZOLE § Aromatase (“Estrogen synthase”) Inhibitor § Competitive Inhibitor § #1 use of this med in world: Male TRT § other AI’s available § concerns with Endocrine pathway disruption (as with finasteride) § Some c/o H/A’s § AI’s as sole TRT is RARE
ANASTROZOLE § Aromatase (“Estrogen synthase”) Inhibitor § Competitive Inhibitor § #1 use of this med in world: Male TRT § other AI’s available § concerns with Endocrine pathway disruption (as with finasteride) § Some c/o H/A’s § AI’s as sole TRT is RARE
 ANASTROZOLE DOSING § 0. 25 mg QOD, 0. 5 mg Q 2 -3 D § 2 day t 1/2, never >Q 3 D § “Frontload” (double initial dose) § Titrate from there § Allow 4 -5 weeks prior to f/u labs
ANASTROZOLE DOSING § 0. 25 mg QOD, 0. 5 mg Q 2 -3 D § 2 day t 1/2, never >Q 3 D § “Frontload” (double initial dose) § Titrate from there § Allow 4 -5 weeks prior to f/u labs
 § NEVER") CRISLER HCG PROTOCOL § 250 IU twice per week SC (starting dose) § NEVER more than 500 IU QD (or elevates estrogens, progesterone) § Transdermal T patients: --every third day § Test cyp IM patients: --T-2/T-1 prior to IM injection --Fri/Sat c/ Sun IM is nice!
CRISLER HCG PROTOCOL § 250 IU twice per week SC (starting dose) § NEVER more than 500 IU QD (or elevates estrogens, progesterone) § Transdermal T patients: --every third day § Test cyp IM patients: --T-2/T-1 prior to IM injection --Fri/Sat c/ Sun IM is nice!
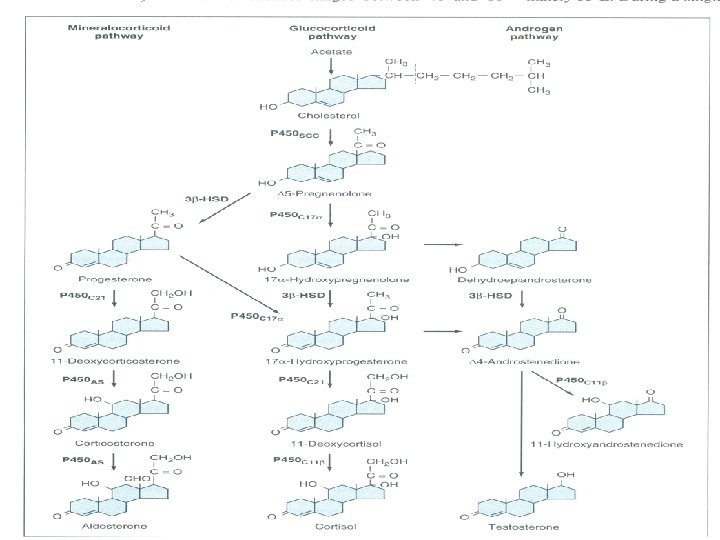
 § Evens out serum androgen levels by t 1/2 of") CRISLER HCG PROTOCOL (con’t) § Evens out serum androgen levels by t 1/2 of cypionate ester § Prevents testicular atrophy § Stimulates all three CHOL pathways § Abundant boost in libido/sense of well being
CRISLER HCG PROTOCOL (con’t) § Evens out serum androgen levels by t 1/2 of cypionate ester § Prevents testicular atrophy § Stimulates all three CHOL pathways § Abundant boost in libido/sense of well being
 RESTORING PATHWAYS § HCG --IM: start at 250 IU SC Days 5/6 --TD: start at 200 IU SC QOD --never more than 500 IU § DHEA --25 mg BID --100 mg QD can elevate E 1 --oral SR>TD>standard oral preparation § Pregnenolone --50 mg TD QD in a cream
RESTORING PATHWAYS § HCG --IM: start at 250 IU SC Days 5/6 --TD: start at 200 IU SC QOD --never more than 500 IU § DHEA --25 mg BID --100 mg QD can elevate E 1 --oral SR>TD>standard oral preparation § Pregnenolone --50 mg TD QD in a cream
 Rescue from “Nipple Issues” § Burning, itching, swelling, FREAKING § Occurs with mere changes in hormone levels, even within physiological range, so… § DO NOT treat in first month (get F/U labs) § 40 mg QD tamoxifen until gone, then taper --cut dose ½ Q 5 D § Prefer tamoxifen over clomiphene § Cannot assay estrogens on SERM-class drugs! § Hold Gh. RT (magnifies E fx) § Gyno may be caused by progesterones
Rescue from “Nipple Issues” § Burning, itching, swelling, FREAKING § Occurs with mere changes in hormone levels, even within physiological range, so… § DO NOT treat in first month (get F/U labs) § 40 mg QD tamoxifen until gone, then taper --cut dose ½ Q 5 D § Prefer tamoxifen over clomiphene § Cannot assay estrogens on SERM-class drugs! § Hold Gh. RT (magnifies E fx) § Gyno may be caused by progesterones
 NO TRT “CYCLING” § Historically “borrowed” from AAS use. § No evidence of benefit § Does not do what is claimed § Leaves substantial periods of letdown § The body thrives on regularity
NO TRT “CYCLING” § Historically “borrowed” from AAS use. § No evidence of benefit § Does not do what is claimed § Leaves substantial periods of letdown § The body thrives on regularity
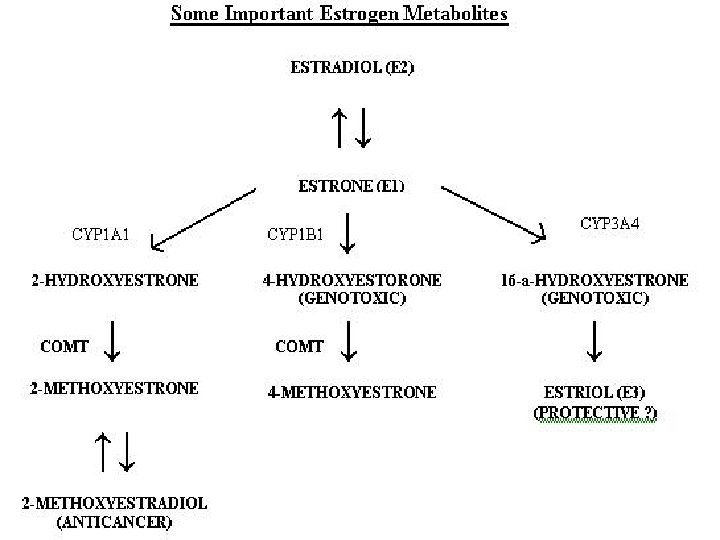
 WHAT IS THE FUTURE OF TRT? § Elevating T to healthy, happy levels § Estrogen metabolism § Actions at the androgen, estrogen receptors § Restoring endocrine pathways
WHAT IS THE FUTURE OF TRT? § Elevating T to healthy, happy levels § Estrogen metabolism § Actions at the androgen, estrogen receptors § Restoring endocrine pathways
 THE GOAL? “The ultimate goal of TRT medicine is to optimize health and happiness in our patients, which means producing an environment where we have elevated testosterone to sufficient levels, with the body responding as if it is unaware of the exogenous manipulations. ” --John Crisler, DO
THE GOAL? “The ultimate goal of TRT medicine is to optimize health and happiness in our patients, which means producing an environment where we have elevated testosterone to sufficient levels, with the body responding as if it is unaware of the exogenous manipulations. ” --John Crisler, DO