8a59d1add7ebb61828b5461bdf693592.ppt
- Количество слайдов: 60



Surviving sepsis Balraj APPADU M. D. , FRCA, FFICM Consultant in Anaesthesia & Intensive Care Medicine

Agenda 1 Understand the scope of the sepsis epidemic 2 Become familiar with the Surviving Sepsis Campaign and the IHI defined sepsis bundles 3 Recognize how time-critical therapies can save lives in the emergency departments and ICUs

What's the problem? n n n Severe sepsis affects over 120, 000 patients each year in the U. K. (increasing at a rate of 1. 5% per annum) Last year 78, 000 of these patients admitted to ITU Mortality for these 30 – 80 %

Comparable Global Epidemiology n 95 cases per 100, 000 n n n 2 week surveillance 206 French ICUs 3 month survey 23 Australian/New Zealand ICUs 51 cases per 100, 000 n England, Wales and Northern Ireland.

Severe Sepsis: Comparison With Other Major Diseases AIDS* Colon Breast Cancer§ †National Mortality of Severe Sepsis Deaths/Year Cases/100, 000 Incidence of Severe Sepsis CHF† Severe Sepsis‡ AIDS* Breast Cancer§ AMI† Severe Sepsis‡ Center for Health Statistics, 2001. §American Cancer Society, 2001. *American Heart Association. 2000. ‡Angus DC et al. Crit Care Med. 2001

Sepsis Epidemiology: Effect of the Aging Population

Economics of Sepsis v Severe Sepsis Ø Ø v $22, 000 per case US annual cost $16. 7 Billion Nosocomial Sepsis Ø Ø increased LOS - ICU 8 days, Hosp 24 days $40, 890 per case Angus CCM, 2001 Pittet JAMA, 1994

Time Sensitive Interventions AMI “Door to PCI” Focus on the timely return of blood flow to the affected areas of the heart. “Time is Brain” Stroke Trauma The sooner that treatment begins, the better are one’s chances of survival without disability. “The Golden Hour” Requires immediate response and medical care “on the scene. ” Patients typically transferred to a qualified trauma center for care.

Severe Sepsis vs. Current Care Priorities U. S. Incidence # of Deaths Mortality Rate AMI (1) 900, 000 225, 000 25% Stroke (2) 700, 000 163, 500 23% Trauma (3) 2. 9 million (Motor Vehicle) (injuries) 42, 643 1. 5% Severe Sepsis (4) 751, 000 215, 000 29% Source: (1) Ryan TJ, et al. ACC/AHA Guidelines for management of patients with AMI. JACC. 1996; 28: 1328 -1428. (2) American Heart Association. Heart Disease and Stroke Statistics – 2005 Update. Available at: www. americanheart. org. (3) National Highway Traffic Safety Administration. Traffic Safety Facts 2003: A Compilation of Motor Vehicle Crash Data from the Fatality Analysis Reporting System and the General Estimates System. Available at http: //www. nhtsa. dot. gov/. (4) Angus DC et al. Crit Care Med 2001; 29(7): 13031310.

Surviving Sepsis Campaign n Launched in Autumn 2002 as a collaborative effort of European Society of Intensive Care Medicine, the International Sepsis Forum, and the Society of Critical Care Medicine Goal: reduce sepsis mortality by 25% in the next 5 years Guidelines revealed at SCCM in Feb 2004, REVISED 2008 n Critical Care Medicine March 2004 32(3): 858 -87. n Website: survivingsepsis. org
, SSI (signs and")
What is sepsis? Sepsis, Septic Shock, SIRS (systemic inflammatory response syndrome), SSI (signs and symptoms of infection), Septicaemia, Bacteraemia, Toxic Shock Syndrome, Bloodstream infection etc, etc….

ACCP/SCCM Consensus Definitions n Infection – Inflammatory response to microorganisms, or – Invasion of normally sterile tissues n Systemic Inflammatory Response Syndrome (SIRS) – Systemic response to a variety of processes n n Severe Sepsis – Organ dysfunction n Septic shock – Sepsis – Hypotension despite fluid resuscitation Sepsis – Infection plus – 2 SIRS criteria Bone RC et al. Chest. 1992; 101: 1644 -55.

What is SIRS? A systemic response to a nonspecific insult Infection, trauma, surgery, massive transfusion, etc Defined as 2 of the following: SIRS Temperature >38. 3 or <36 0 C Heart rate >90 min-1 Respiratory rate >20 min-1 White cells <4 or >12 Acutely altered mental state Hyperglycaemia (BM>7. 7) in absence of DM SEVERE SEPSIS

What counts as an infection? Pneumonia 50% Abdominal 25% Urinary Tract infection Meningitis Endocarditis Device related Central line Cannula Pain Diarrhoea Distension Urgent laparotomy Soft tissue/ musculoskeletal Cellulitis Septic arthritis Fasciitis Wound infection

what is Sepsis? SIRS due to an infection

What is Severe Sepsis? Sepsis with organ dysfunction, hypoperfusion or hypotension CNS: CVS: Resp: Renal: Hepatic: Bone marrow: Hypoperfusion: Coagulopathy: Acutely altered mental status Syst < 90 or mean < 65 mm. Hg Sp. O 2 >90% only with new/ more O 2 Creatinine >177 μmol/l or UO <0. 5 ml/kg/hr for 2 hrs Bilirubin >34 μmol/l Platelets <100 Lactate >2 mmol/l INR>1. 5 or a. PTT>60 secs

What is shock? Tissue perfusion is not adequate for the tissues’ metabolic requirements Types of Shock Cardiogenic Neurogenic Hypovolaemic Anaphylactic and… Septic Shock secondary to systemic inflammatory response to a new infection

What is shock? Tissue perfusion is not adequate for the tissues’ metabolic requirements For sepsis, shock is one of: fluids SBP < 90 mm. Hg MBP < 65 mm. Hg Drop of < 40 mm. Hg Lactate > 4 mmol/l after IV

The Sepsis Continuum SIRS § Sepsis A clinical response arising from a nonspecific insult, with 2 of the following: o o § T >38 C or <36 C § HR >90 beats/min § RR >20/min 3 § WBC >12, 000/mm or <4, 000/mm 3 or >10% bands SIRS with a presumed or confirmed infectious process Severe Sepsis Septic Shock Sepsis with organ failure Refractory hypotension SIRS = systemic inflammatory response syndrome Chest 1992; 101: 1644.

Severe Sepsis Screening Tool Are any 2 of the following SIRS criteria present and new to your patient? Obs: Temperature >38. 3 or <36 0 C Respiratory rate >20 min-1 Heart rate >90 bpm Acutely altered mental state Bloods: White cells <4 x 109/l or >12 x 109/l Glucose>7. 7 mmol/l (if patient is not diabetic) If yes, patient has SIRS

Is this likely to be due to an infection? For example Cough/ sputum/ chest pain Dysuria Abdo pain/ diarrhoea/ distension Headache with neck stiffness Line infection Cellulitis/wound infection/septic arthritis Endocarditis If yes, patient has SEPSIS Start SEPSIS BUNDLE

Check for SEVERE SEPSIS BP Syst < 90 / Mean < 65 mm. Hg (after initial fluid challenge) Lactate > 4 mmol/l Urine output < 0. 5 ml/kg/hr for 2 hrs INR > 1. 5 a. PTT > 60 s Bilirubin > 34 μmol/l O 2 Needed to keep Sp. O 2 > 90% Platelets < 100 x 109/l Creatinine > 177 μmol/l or UO < 0. 5 ml/kg/hr Severe Sepsis: Ensure Senior Doctor/ITU to attend NOW!

What is a Bundle? n Specifically selected care elements n n From evidence based guidelines Implemented together provide improved outcomes compared to individual elements alone

6 Hour Resuscitation Bundle n n n Early Identification Early Antibiotics and Cultures Early Goal Directed Therapy

6 - hour Severe Sepsis/ Septic Shock Bundle n n Early Detection: n Obtain serum lactate level. Early Blood Cx/Antibiotics: n within 3 hours of presentation. Early EGDT: Hypotension (SBP < 90, MAP < 65) or lactate > 4 mmol/L: n initial fluid bolus 20 -40 ml of crystalloid (or colloid equivalent) per kg of body weight. • Vasopressors: – Hypotension not responding to fluid – Titrate to MAP > 65 mm. Hg. • Septic shock or lactate > 4 mmol/L: – CVP and Scv. O 2 measured. – CVP maintained >8 mm. Hg. – MAP maintain > 65 mm. Hg. • Scv. O 2<70%with CVP > 8 mm. Hg, MAP > 65 mm. Hg: – PRBCs if hematocrit < 30%. – Inotropes.

Why does it matter?

Perspective Severe Sepsis No. cases per 100, 000 per annum Acute coronary syndrome 127 200 Sepsis Six (our data) First hour antibiotics NNT invasive care EGDT (Rivers) Resusc Bundle (SSC) 6 Clopidogrel 48 5 β-blockade 42 Aspirin NNT ‘basic’ care 26 6 18 Thrombolysis 15 PCI over thrombolysis 33

The Sepsis Six 1. Give high-flow oxygen via non-rebreath bag 2. Take blood cultures and consider source control 3. Give IV antibiotics according to local protocol 4. Start IV fluid resuscitation Hartmann’s or equivalent 5. Check lactate 6. Monitor hourly urine output consider catheterisation within one hour. . plus Critical Care support to complete EGDT

Give Antibiotics Start therapy as soon as possible and certainly in the first hour. . . preferably after taking blood cultures!! Choice should include one or more with activity against likely pathogen Penetration of presumed source Guided by local pathogens Give broad spectrum till defined

SSC- antibiotics n n n Begin IV antibiotics as early as possible, and always within the first hour of recognising severe sepsis (1 D) and septic shock. (1 B) Broad-spectrum: one or more agents active against likely bacterial/ fungal pathogens and with good penetration into presumed source. (1 B) Reassess antimicrobial regimen daily to optimise efficacy, prevent resistance, avoid toxicity & minimise costs. (1 C)

Begin IV antibiotics as early as possible, and always within the first hour of recognising severe sepsis (1 D) and septic shock. (1 B) Citation: Kumar A et al. Crit Care Med 2006: 34(6) Retrospective, 15 years, 14 sites n = 2, 154 median 6 h, 50% administered in 6 h Only 5% first 30 minutes- survival 87% 12% first hour- survival 84%

Cumulative Initiation of Effective Antimicrobial Therapy and Survival in Septic Shock 1. 0 survival fraction 0. 8 0. 6 0. 4 0. 2 0. 5 51 - 1 2 23 34 45 56 69 912 12 -2 24 4 -3 36 6 + 0. 0 0 - fraction of total patients cumulative antibiotic initiation time from hypotension onset (hrs) Kumar et al. CCM. 2006: 34: 1589 -96.
 Funk and Kumar")
Running average survival in septic shock based on antibiotic delay (n=4195) Funk and Kumar Critical Care Clinics 2012(in press)
 For each hour’s")
Running average survival in septic shock based on antibiotic delay (n=2154) For each hour’s delay in administering antibiotics in septic shock, mortality increases by 7. 6% Funk and Kumar Critical Care Clinics 2011 (in press)
 Odds Ratio")
Early antibiotics are good. . . Author n Setting Median time (mins) Odds Ratio for death Gaieski 261 ED, USA (Shock) 119 0. 30 Daniels 567 Whole hospital, 121 UK 0. 62 Kumar 2154 ED, Canada (Shock) 360 0. 59 Appelboam 375 Whole hospital, 240 UK 0. 74 Levy 15022 Multi-centre 0. 86 Crit Care Med 2010; 38: 1045 -53 Emerg Med J 2010; doi: 10. 1136 Crit Care Med 2006; 34(6): 1589 -1596 Critical Care 2010; 14(Suppl 1): 50 Crit Care Med 2010; 38 (2): 1 -8 (first hour vs all times) (first hour vs second hour) (first 3 hours vs delayed)

Retrospective, 22 hospitals, n= 4532 • 64. 4% septic shock patients developed early AKI • Median time shock to antibiotic = 5. 5 h • OR for AKI 1. 14 (1. 10 -1. 20) P < 0. 001 per hour’s delay Bagshaw SM et al Intensive Care Med. 2009; 35(5): 871 -81
: 1 -8")
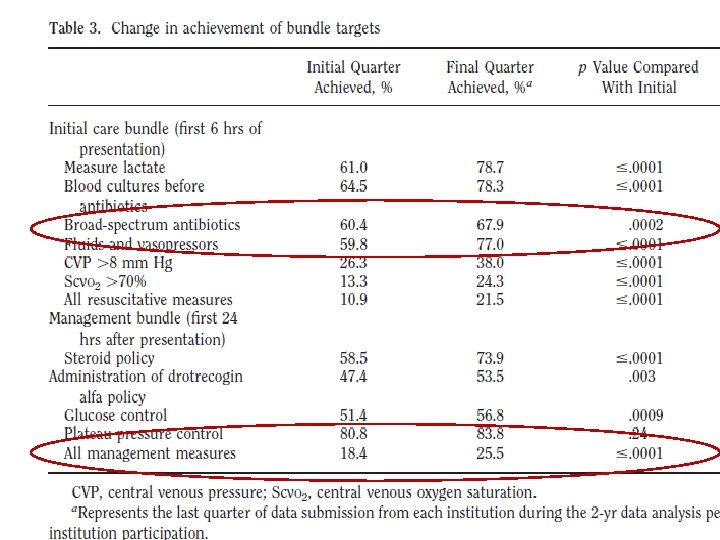
SSC Results: Critical Care Medicine 2010; 38(2): 1 -8
: 1 -8")
SSC Results: Critical Care Medicine 2010; 38(2): 1 -8

Appropriate antibiotics Citation: Ibrahim et al. Chest 2000; 118: 146– 155 BSI, n = 492 70 60 50 Mortality (%) 59. 1% HAI p<0. 001 40 29. 9% inadequate 8. 3% fungal VREs Pseudomonas Coag-neg Staph 30 20 10 0 Appropriate initial antibiotic Inappropriate initial antibiotic MONARCS trial OR 0. 65 for death with adequate cover (n=2634) Mac. Arthur RD et al. Clin Infect Dis 2004; 38: 284 -288

Fluids Why? To reduce organ dysfunction and multi-organ failure By optimising tissue oxygen delivery By increasing organ perfusion

Optimising oxygen delivery DO 2 = Oxygen delivery to the tissue DO 2 = Ca. O 2 x CO Ca. O 2 = Amount of O 2 in arterial blood Ca. O 2 = ([Hb] x Sa. O 2 x 1. 34) + (Pa. O 2 x 0. 0225) Fluid therapy improves cardiac output by increasing venous return to the heart

How to fluid resuscitate Judicious fluid challenges Up to 60 ml/kg in divided boluses (min. 20 ml/kg in shock) Crystalloid Colloid (500 ml boluses) (250 -300 ml boluses) Reassess for effect after each challenge HR, BP, capillary refill, urine output, RR In patients with cardiac disease Use smaller volumes More frequent assessment Early CVC

Lactate High lactate identifies tissue hypoperfusion in patients at risk who are not hypotensive ‘Cryptic shock’ Gives an overview of current tissue oxygen delivery The Goal Lactate to improve as resuscitation progresses

Risk stratification by lactate Trzeciak, S et al , Acad Emerg Med; 13, 1150 -1151. n-=1613
 The")
Urine Output Accurate hourly urine output monitoring (for many, this will mean catheterisation) The Goal > 0. 5 ml/kg/hr > 40 ml/hour in the average adult

Urine Output Urine output is a direct measure of GFR= Glomerular Filtration Rate GFR is directly proportional to CO Kidneys receive 1/5 cardiac output (1 L/min) CO falls UO falls Therefore urine output in the early stages is a useful assessment of cardiac output

Renal Blood Flow & Urine Output In health, kidneys autoregulate, so UO is independent of BP over a wide range In sepsis, this is lost and UO will fall as BP falls

Early Goal Directed Therapy

EGDT Call for specialist support CVP line < 8 mm. Hg Crystalloid Colloid >8 mm. Hg MAP < 65 or <90 mm. Hg Vasoactive Drugs >65 & >90 mm. Hg Scv. O 2 < 70% Transfuse red cells until Hb > 10 g/dl YES >70% Scv. O 2 >70% NO Goals Achieved Inotropic agents Rivers et al 2001, NEJM; 345, 1368 -1377
 60 50")
The Importance of Early Goal-Directed Therapy for Sepsis Induced Hypoperfusion Mortality (%) 60 50 40 Standard therapy 30 EGDT 20 10 0 NNT to prevent 1 event (death) = 6 -8 In-hospital mortality (all patients) 28 -day mortality 60 -day mortality ARR 16% Adapted from Table 3, page 1374, with permission from Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345: 1368 -1377
 567 (100) Total Mortality % 34. 7")
Mortality by Sepsis Six Cohort size (%) 567 (100) Total Mortality % 34. 7 Sepsis Six 347 (61. 2) 44. 0 Sepsis Six 220 (38. 8) 20. 0 RRR % (NNT) - 46. 6 (4. 16)
 Total 567 (100%) 34.")
Mortality by antibiotics Cohort size Mortality % RRR % (NNT) Total 567 (100%) 34. 7 - Delayed Antibiotics 217 (38. 4%) 45. 4 Antibiotics within 1 h 350 (61. 6%) 28. 1 38. 1 (5. 77)
 Total 567 (100%)")
Mortality by fluid challenges Cohort size Mortality % RRR % (NNT) Total 567 (100%) 34. 7 - No fluids in 1 h 183 (32. 3%) 44. 8 Fluids in 1 h 384 (67. 7%) 30. 0 33. 0 (6. 73)

For patients receiving the Sepsis Six 2. 0 fewer Critical Care bed days 3. 4 fewer hospital bed days Compared with other survivors Equates to c. £ 5, 000 cost ‘saving’

The clincher

Achieving 80% reliability For each year, for every 500 beds. . 62 lives saved 883 fewer bed days 520 fewer CC bed days Direct costs for survivors reduced by £ 0. 78 M

Summary n n n Improve recognition/diagnosis Alter attitude – treat sepsis like MI Early aggressive treatment Use EGDT Collaborate with ITU early

n n Sepsis is a life-threatening condition that arises when the body's response to an infection injures its own tissues and organs. Sepsis leads to shock, multiple organ failure and death especially if not recognized early and treated promptly. Sepsis remains the primary cause of death from infection despite advances in modern medicine, including vaccines, antibiotics and acute care. Millions of people die of sepsis every year worldwide

Comments and Questions
8a59d1add7ebb61828b5461bdf693592.ppt