9e73a022295452d890e19fc40eb5bb9f.ppt
- Количество слайдов: 40



Surgical infection and outbreaks Malcolm Richardson Ph. D, FSB, FRCPath Regional Mycology Reference Centre University Hospital of South Manchester, and The University of Manchester

Nosocomially vs. community-acquired IA Nosocomial • Due to break in, or contamination of hospital water system • Due to break in HEPA filtration system • Due to construction or demolition work in the hospital Community-acquired • Due to occupational activities • Due to leisure activities • Due to exposure to Aspergillus spores (minimum effective dose not known) Praz-Christinaz et al. Transplant Infect Dis 2007; 9: 175 -181

• 53 outbreaks: 1967 -2005 • 458 affected patients: – – – 299 (65. 3%) haematological malignancies Route of transmission: air Site of primary infection: lower respiratory tract (356 patients) Surgical site infections (24 patients) Skin infections (24 patients)

Nosocomial aspergillosis

Outbreaks update 2009 Weber et al. Medical Mycology 2009 • >60 English literature

Species distrubution

Infection sites • Pulmonary • Post-operative – Cardiac surgery – Ophthalmic surgery – Dental surgery • Cutaneous

Post-operative aspergillosis • Dd paper • >500 cases • Cardiac surgery (n = 188 • Ophthalmic surgery (n > 90) • Dental surgery (n = 100) • Wound infection (n = 22) • Bronchial infections (n = 30) • Orthopedic surgery (n = 42) • Vascular prosthetic surgery (n = 22) • Neurosurgery (n = 25) • Source presumed to be airborne infection

2010 • 20 healthy individuals • Conventional and molecular analysis • 74 culturable genera • 11 non-culturable • Aspergillus species: 35%

• Liver transplant recipient • 11 -days post-transplant: Aspergillus fumigatus deep-surgical site infection • 2 patients: transplantation unit: pulmonary aspergillosis • Debridement and changing of dressings: bioaerosols CID 2002


Events in the growth of Aspergillus

Aw < 0. 80, ERH <80% Aw < 0. 80 -0. 90, ERH <80 -90% Aw >0. 90, ERH >90% water Aw: Minimum water activity level at 25°C ERH: Equilibrium relative humidity

Air as a source of human infection Inhalation: most common portal of entry Temporal association between hospital-based outbreaks and construction Very little data on base-line concentrations Longitudinal studies show no correlation between sporadic cases of IA and changes in spore count

Concentrations of airborne Aspergillus compared to the incidence of invasive aspergillosis: lack of correlation 54 -week air sampling period A. fumigatus and A. flavus: mean 1. 83 cfu m-3 Individual samples: maximum: 11. 6 cfu m-3 No correlation with season or ward 6 cases of IPA during sampling period No association with fluctuations in air count Conclusion: “the available data do not provide a firm link between hospital exposure and an increased incidence of aspergillosis” Hospenthal et al. , Medical Mycology 1998.

Heavy excavation!

Ventilation as a source

Source of Aspergillus in the operating theatre

Surgical infection

A thermal ceiling as source of Aspergillus

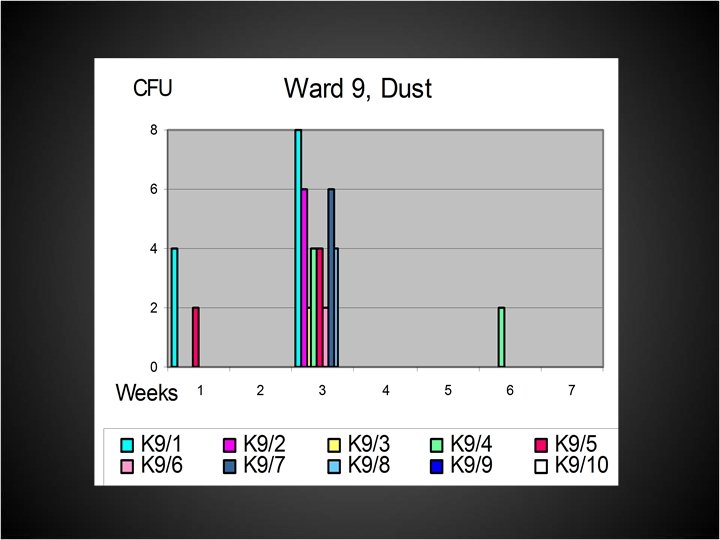
Dust: a perfect home for Aspergillus! GM

Dust collection

Air sampling: SAS Super 100 and Duo

Acceptable levels • • HEPA filtered air: 0 Open ward: ? General hospital areas: ? Outdoor air: highly variable/seasonal

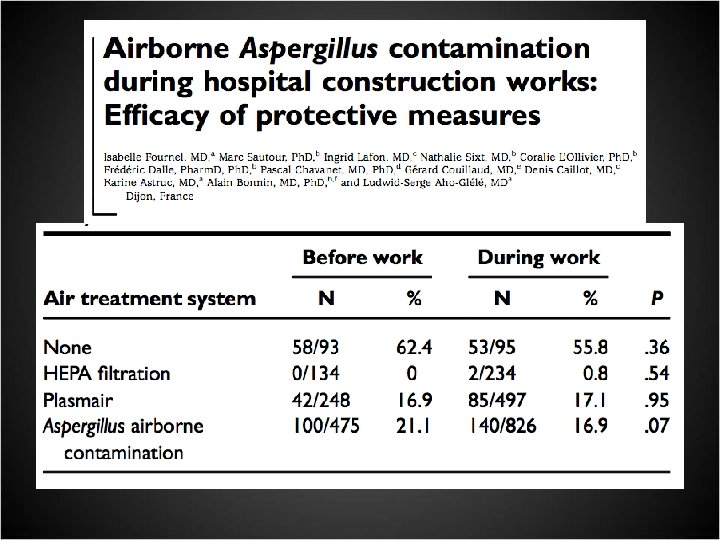
Efficacy of prevention by HEPA filtration or laminar airflow against Aspergillus airborne contamination during hospital renovation • Conclusions: – strong association between building renovation and an increase in environmental contamination – confirmation of the high efficacy of laminar airflow plus HEPA filtration and a high air-exchange rate – HEPA filtration alone did not prevent contamination during renovation – ”A standard protocol for aerobiological surveillance is needed” Cornet et al. Infect Control Hosp Epidemiol 1999; 20: 508 -513.

Invasive aspergillosis related to construction and the utility of air sampling 8 -bedded BMT unit 2 cases of IPA 5 cases of colonisation Coincided with major construction project on floor directly below unit • High air counts before cleaning • No isolation after construction stopped and deep cleaning • • Lai et al. , 39 th ICAAC, San Francisco 1999

Is air sampling necessary, if so, when? • Determination of source: outbreaks • occupants have symptoms, but no obvious building damage • contamination suspected through air from other parts of the building

Aspergillus fumigatus Malt extract agar • • • Heptane Undecane Isoprene 2, 4 Hexadiene 2 -Methyl-1, 3 -pentadiene 1, 3 -Octadiene 2 -Methyl-1 -butanol 3 -Methyl-1 -butanol 2 -Ethyl-1 -hexanol Head-space solid-phase microextraction Wood • • • Methylpyrazine Acetone 2 -Pentanon 2 -Hexanone 2 -Heptanone 4 -Heptanone 2 -Octanone 3 -Octanone Acetophenone -Farnesene Fiedler et al. 2001 Int J Hyg Environ Health

• 7 -year sampling period: weekly: 978 samples • Aspergillus spp. 16. 7%: 1. 8 cfu/m 3 - 28. 3 cfu/m 3 • 45 cases proven IA (2. 29% allo; 0. 36% auto HSCT) • cases of IA analysed 14 and 28 -days following high counts • Conclusion: high counts did not predict risk of developing IA Rupp et al. JHI 2008.

Particle counting Hansen et al. JHI 2008; 70: 259 -264.

Particle counting • IQAir Particle Scan Pro Airborne Laser Counter • 0. 3 m - 5 m

• during demolition building was sealed and water sprayed to minimise dust emission • particle and fungal concentrations monitored before and during demolition • particle concentrations significantly higher during demolition • no difference in moulds cultured at 370 C before and during demolition

Air quality monitoring of HEPA-filtered hospital rooms by particulate counting Anttila V-J, Nihtinen A, Kuutamo T, Richardson M. 2008.

Air quality monitoring of HEPA-filtered hospital rooms by particulate counting Anttila V-J, Nihtinen A, Kuutamo T, Richardson M. 2008.

• Construction of an outbreak curve • Line listing of all infected patients • Evaluation of air ventilation system • Regular particle counting • Water damage/ingress assessment • Possible common source exposure • Air sampling • Water analysis • Settled dust analysis

Air. In. Space: Immunair 540 -640 m 3/hr rapid air decontamination not sensitive to exterior movement • <1 cfu/m 3 • • Am J Infect Control 2007; 35: 460 -466.

Conclusions • Overall mortality among patients involved in outbreaks: 50 -60% • Recent outbreaks due to internal construction or renovation with failure to control spread of contaminated dust • Key interventions: surveillance and engineering controls • Minimum effective dose of Aspergillus conidia is not known
9e73a022295452d890e19fc40eb5bb9f.ppt