1ef2c088559259a59f53bbdcd46ee139.ppt
- Количество слайдов: 78



Surgical and Non-Surgical Treatment of Endometriosis Maciej Barczentewicz, Radosław Maksym, Magdalena Machlarz IIRRM 11 th Annual General Meeting 2014 & Restorative Reproductive Medicine Conference Stratford-upon-Avon, UK | July 9 th, 2014

Faculty Disclosure Doctor Maciej E. Barczentewicz, MD Male Fertility Support Dr. Maciej E. Barczentewicz has listed no financial 33 rd Annual Meeting of the American Academy of interest/arrangement that would be considered Fertility. Care™ Professionals Stratford-upon-Avon, UK | July 9 -12, 2014 a conflict of interest. Maciej Barczentewicz, Wojciech Dzierżak

Surgical and Non-Surgical Treatment of Endometriosis Presentation Outline • Update • Critical appraisal • Our Management • Our results • Case presentation

Endometriosis Endometrial tissue is found outside the uterus • Pelvic pain: dysmenorrhoea, dyspareunia, dyschezia • Subfertility • High Prevalence ( 4 -20% ) • Incidence rate 1 per mille / year • Limited treatment possibilities • Ovarian cancer risk is 27 -80% higher

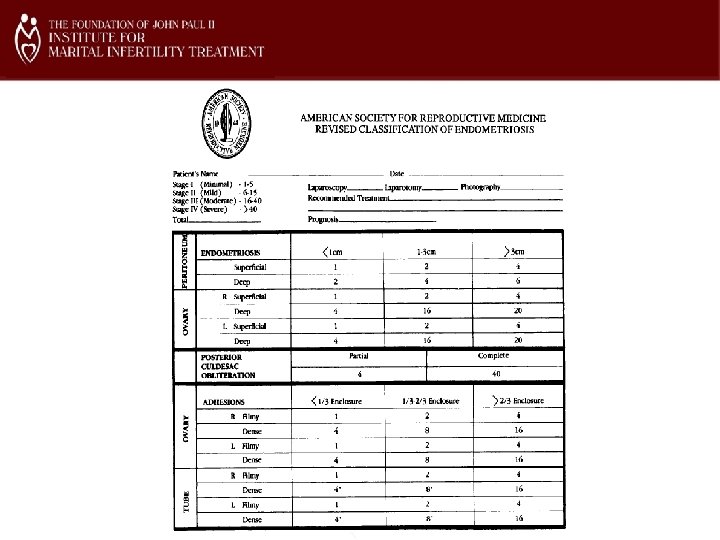
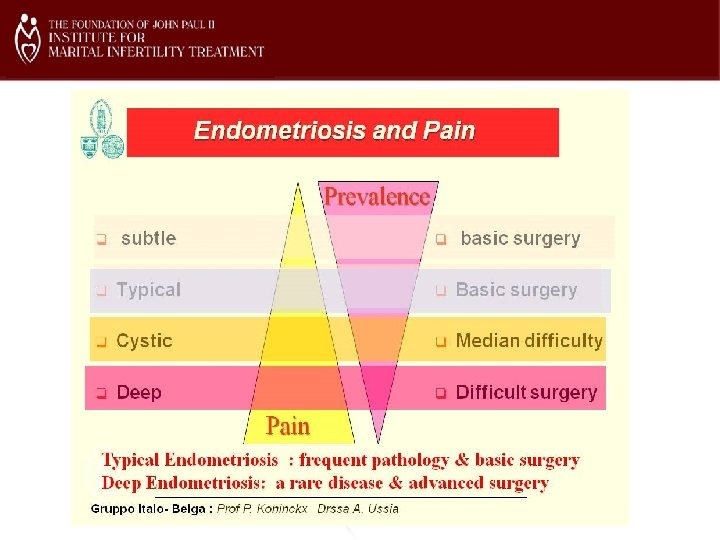
Clinical types of endometriosis • Subtle endometriosis : 1 -3 mm superficial • Typical endometriosis : 5 -40 mm superficial lesions • Cystic ovarian endometriosis • Deep involved endometriosis • Peritoneal Pockets or Allen en Master syndrome Adenomyosis Endosalphingiosis

Retrograde menstruation Sampson JA. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am J Obstet Gynecol 1927; 14: 422 -469.

Retrograde menstruation - physiologic „Endometriosis does not exist. All women have endometriosis” J. Evers 1994, ESHRE

Endometriosis Theories • Coelomic metaplasia • Hormones • Apoptosis Suppression and Alteration of Endometrial Cell Fate • Stem Cells • Genetics • Oxidative Stress and Inflammation • Immune Dysfunction

Immune Dysfunction women with endometriosis • • Presence of Immune complex antigen-antibody Ig. G & C 3 complement in endometrium Weed JC, Arquembourg PC 1980 Peripheral blood T cells low and B cells high activity , high antibodies syntesis Stratseva 1980 High level of Ig. A & Ig. G anti-endometrial and anti-ovarian antibodies in peripheral blood Mathur 1982 Presence of Anti- phospholipid antibodies Ig. G and Ig. M in peripheral blood Gleicher 1986 Women with endometriosis are at increased risk for a host of other diseases including chronic fatigue syndrome, multiple sclerosis, lupus, underactive thyroid, and rheumatoid arthritis National Institute of Child Health and Human Development 2002 CD 4⁺ CD 25⁺ FOXP 3⁺ regulatory T cells in peripheral blood and peritoneal fluid of patients with endometriosis. Olkowska-Truchanowicz J, Maksym RB et al. 2013 High rate of allergies among women with endometriosis Matalliotakis 2012
: • positive correlation between endometriosis and")
Role of allergy and autoimmune infamantory diseases (endometriosis): • positive correlation between endometriosis and allergic manifestations, including hay fever, sinus allergic rhinitis, and food allergy type 1 (immediate type hypersensitivity) • women with endometriosis frequently suffer from autoimmune inflammatory diseases, allergies and asthma • study indicated a link between endometriosis and increased risk of allergic autoimmune disorders (that should further be explored) Matalliotakis et al. , 2012; Bungum et al. , 2014

Food hypersensitivity and Ig. G-dependent immune reactions: • No significant correlation between food hypersensitivity and fertility problems • Ig. G-dependent allergy affects about 45% of USA and Europe population, and is twice as common in women than in men • Immunotoxins : immune complexes formed with Ig. G antibodies and fragments of dietary proteins cause systemic or local chronic inflammation at low intensity • No specific symptoms, possible changes in the clinical picture in the course of the disease and localization of the lesions • Delayed reactions : might occur 8 -72 hours after the food consumption Audit of York Nutritional Laboratory survey, conducted by the Department of Health Studies, University of York, on behalf of the British Allergy Foundation. 2001, January

Ig. G-dependent food hypersensitivity and chronic/autoimmune diseases: Food-specific Ig. G & immune reactions • Complement & anafilatoxin generation (C 3 a, C 5 a) • Immune cells & release of proinflammatory cytokines (IL-1, IL-6, TNF-a), proteases, ROS-mediated reactions • Basophils and platelets & release of amines vasomotor Chronic /autoimmune diseases • Functional bowel disorders (e. g. Irritable bowel syndrome) • Inflammatory bowel disease (e. g. Crohn’s Disease, Ulcerative colitis) • Joint diseases (e. g. Rheumatoid arthritis) • Respiratory disorders (e. g. Asthma, Chronic sinusitis) • Dermatological disorders (e. g. Atopic dermatitis) • Chronic medical conditions (e. g. Obesity, Atherosclerosis, Migraine headaches, Diabetes) Sampson & Mc. Caskill, 1985; Pelikan, 1988; Crowe & Perdue, 1992; Hazebons & et al. , 1996; Aktinson & et al. , 2004; Ress & et al. , 2005; Harman & Hart, 2007; Zuo & et al. , 2007; Wilders & et al. , 2008; Bentz & et al. , 2010; Aply & et al. , 2010;

Vitamin D deficiency – discussion: • • • vitamin D role in the pathogenesis and treatment of endometriosis (an immunomodulator and anti-inflammatory agent) VDR and vitamin D metabolizing enzymes are found in endometrium (normal cycling, eutopic and ectopic endometrium of women with endometriosis) the endometrium is a target of 1, 25 dihydroxyvitamin D actions through regulation of specific genes and via immunomodulation. the endometrium in endometriosis expresses dysregulation of some vitamin D enzymes and receptors. VDR-agonist was shown to reduce the development of endometriotic lesions and recurrence (mouse model) Sayegh et al, 2014; Bertone-Johnson et al. , 2010; Du et al. , 2005, Sayegha et al. , 2013

Diagnosis and Treatment of Endometriosis CAROLINE WELLBERY, M. D. , Georgetown University School of Medicine, Washington, D. C Am Fam Physician. 1999 Oct 15; 60(6): 1753 -1762.



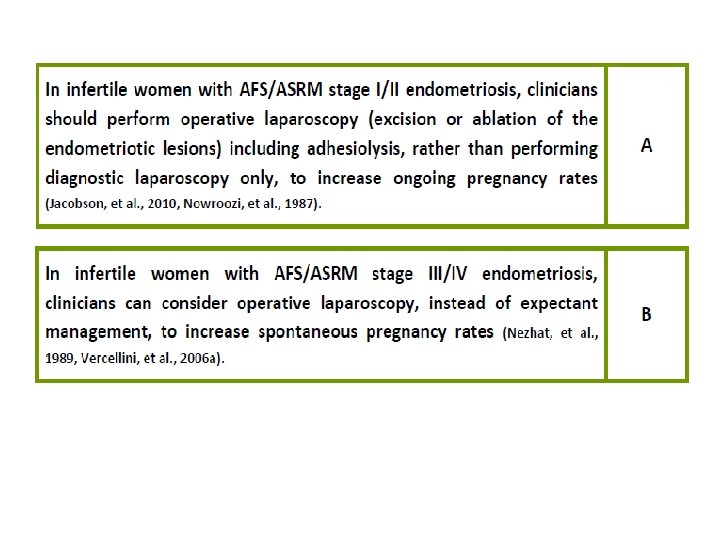
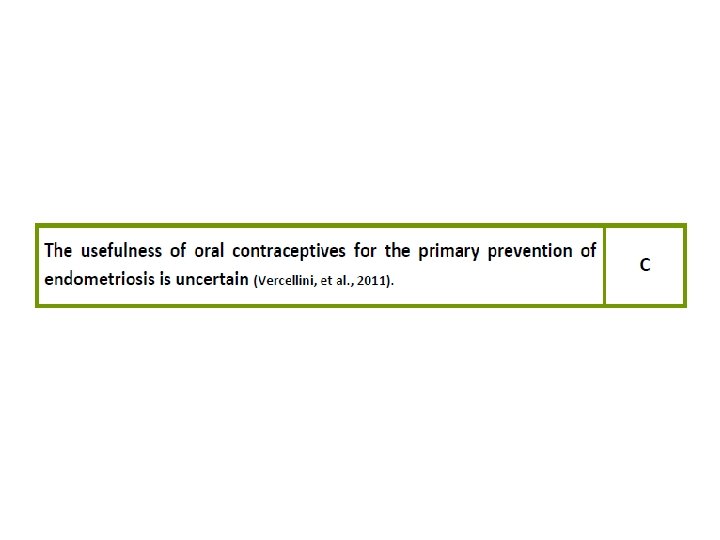
Aktualne wytyczne


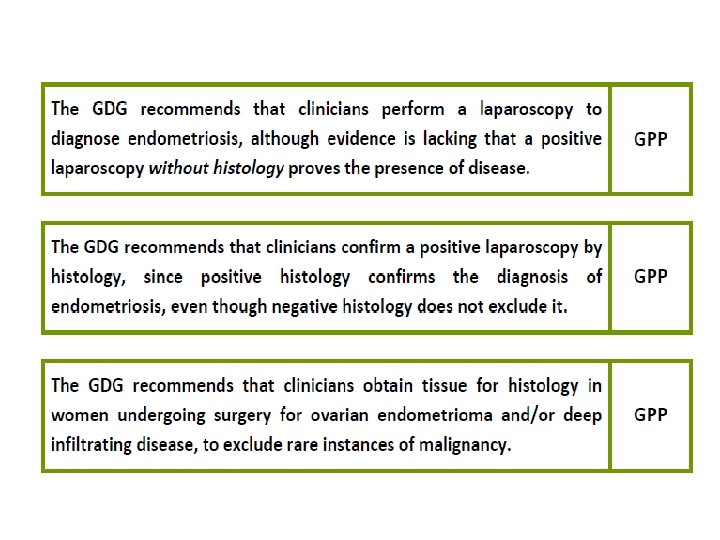
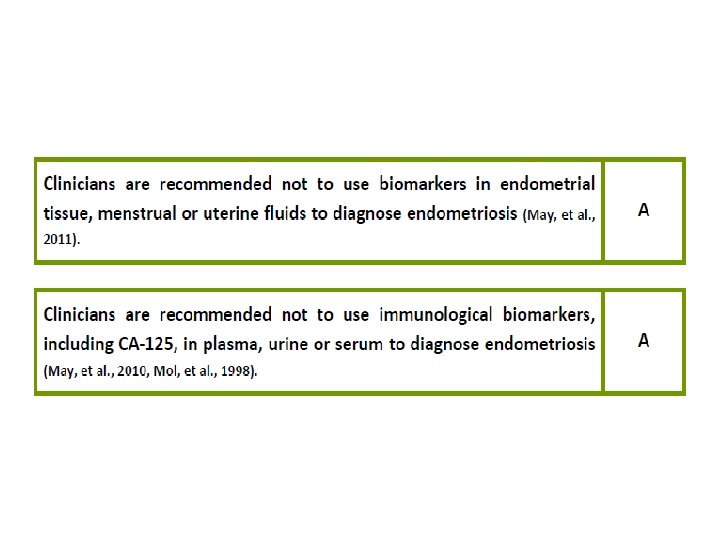
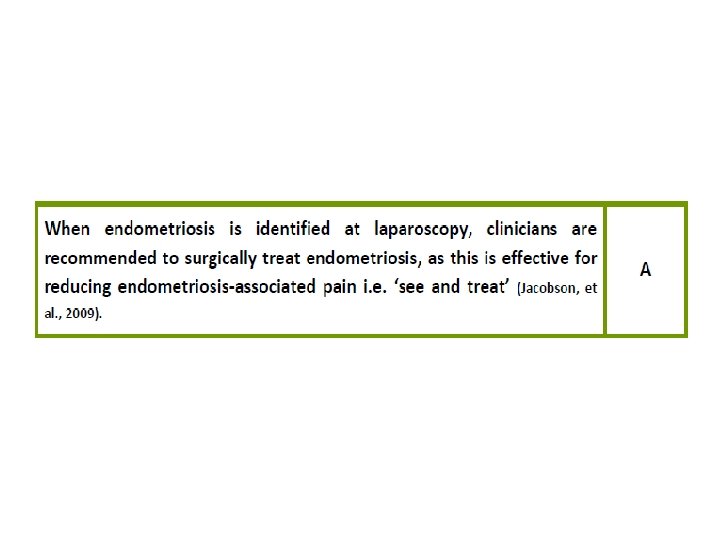
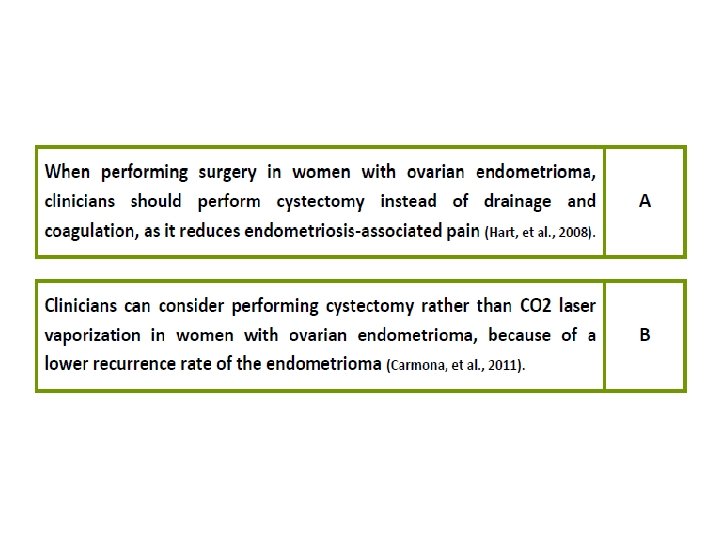
Grades of Recommendations A Supporting evidence Evidence from meta-analysis of randomized controlled trials B Evidence from at least one controlled study without randomization C Evidence from non-experimental descriptive studies, such as comparative studies, correlation studies, and case-control studies D Case reports GPP Evidence from expert committee reports or opinions or clinical experience of respected authorities, or both


Surgical and Non-Surgical Treatment of Endometriosis Our Management : • Medical treatment : “good” Cr. MS chart, letrozol , LDN • Diet • Surgery – near contact LPS, LPT – cooperating surgeons in Poland: Dr Dr: Baryła, Binkiewicz, Gałczyński, Gratkowski, Klimas, Maksym, Ulman, • Interventional Radiology: prof Małgorzata Szczerbo. Trojanowska, prof Jan Oleszczuk, Dr Waciński • Psychotherapy ( some cases)
 – our results, n= 61 (1): Most frequently")
Role of diet and nutrients (endometriosis) – our results, n= 61 (1): Most frequently consumed foods: • gluten grains: wheat bread, wheat pasta, wheat roll • dairy products: cheese, sour cream, cottage cheese, cow's milk • vegetables: potato, tomato • fruits: apple, banana
 – our results, n=61 (2): Conclusions: • too")
Role of diet and nutrients (endometriosis) – our results, n=61 (2): Conclusions: • too high intake of processing dairy products • too high intake of processing cereal products • excessive intake of cereal gluten • too low intake of gluten-free cereals (including rice, millet, buckwheat, amaranth) • too low a variety of fruits and vegetables consumed • too high intake of processed meat • small intake: fish, legumes, nuts and seeds, unrefined oils

Distribution of food-specific Ig. G in women with infertility & edometriosis – our results, n= 124 • In patients with a diagnosis of female subfertility and coexisting endomteriosis are elevated levels of food-specific Ig. G(1 -4) • The most common “female subfertility” food allergens identified by the diagnostic tests for serum specific Ig. G(1 -4) antibodies are: hen’s eggs (90%), wheat (92%), gluten & other gluten cereals (58%) milk (72%), corn (55%), yeast (51%) Food. Detective test 46; ELISA Ig. G(1 -4), (Cambridge Nutritional Sciences Ltd/ Genesis Diagnostics Ltd, UK)
")
Vitamin D deficeincy – our results, n=61 • Vitamin D deficiency: 91, 8% (56) 11. 5 % (7) 0 -10 ng/ml 45. 9 % (28) 10 -20 ng/ml 34. 4 % (21) 20 - 30 ng/ml 8, 2 % (5) 30 - 80 ng/ml • Vitamin D in the standard: 8, 2 % (5) • The average concentration of vitamin D: 18. 7 ng / ml (4. 6 ng / ml - 37. 3 ng / ml)

Our Individual Dietetic Program consists of: • • • Quantitative and qualitative analysis of individual nutrition habits Optimization of nutritional program Recommendations for the preconception nutrition Recommendations for the anti-inflammatory diet Recommendations for the elimination and/or rotation diet Recommendations for the nutrition in the coexisting diseases (on the basis of current scientific data) • Consideration of the possible interactions between nutrition and medicines taken by the patients • Supplementation (in regard to accompanying diseases, and /or elimination diet) • Recommendations for the healthy life style (sport activity, appropriate sleeping time, sun exposition, avoiding the stress, prayer time)

The expected benefits of dietary intervention with our Individual Dietetic Program: • Mute the allergic response and inflammation in the digestive system • Reduction and prevention of mucosal barrier dysfunction to food allergens • Improved gastrointestinal function and nutrient absorption • Minimize the likelihood of pseudoallergic reactions • Recovery of immune tolerance to the actually harmful food

CASE PRESENTATION

Couple 1 G-0 P-0 Age of wife: 37 Age of husband: 40 • Efforts to conceive: 6 month • Diagnosis on entry into NPT : • ENDOMETRIOSIS Grade IV LPS 2011; • Adhesions - frozen pelvis • Large Bowel obstruction • Endometriosis of urinary tract • Hydronephrosis with left ureteral stricture • Left fallopian tube occluded
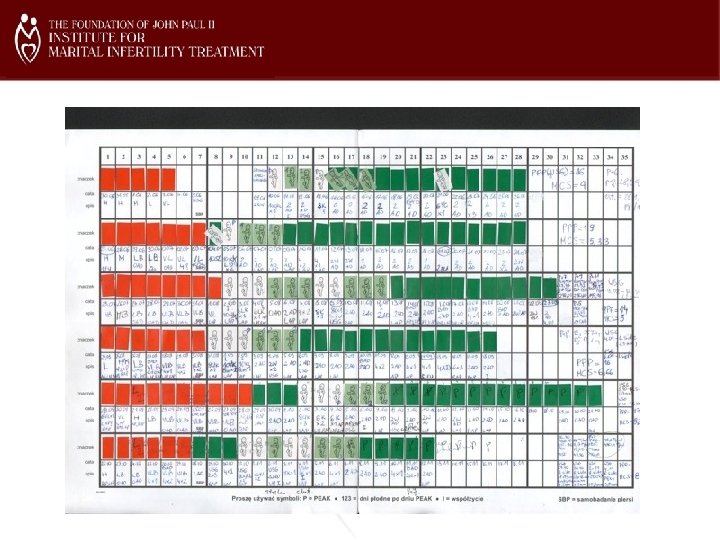

Couple 1 G-0 P-0 Cr. MS from : 30. 05. 2012 NPT diagnosis: WIFE • CA 125 178 • Hydrosalpinx • Latent hyperprolactinemia after MTC PRL 490 IU/ml 4265 IU/ml • Limited mucus MCS 6. 9 • Low progesterone at Peak+7 • FOOD Intolerance • treatment with bromocryptine, progesterone, vitamin. D 3 , LDN, Letrozole, ACC, Diet

Couple 1 G-0 P-0 Referal to surgery Pope Paul VI Institute Dr Hilgers Omaha , Nebraska USA

Couple 1 G-0 P-0 Cr. MS from : 30. 05. 2012 NPT diagnosis: HUSBAND • SPERM ANALISYS 18. 09. 2012 sperms 32 mln/ml motility 34% morph 21% elevated viscosity • Treatment : suplements; acetylcysteine 600 – fertile period • SPERM ANALISYS 13. 11. 2012 sperms 53 mln/ml motility 44% morph 29% norm viscosity

Couple 1 G-0 P-0 Cr. MS from : 30. 05. 2012 After 12 month of Cr. MS natural conception Baby Girl 3680 g cesarian section 6. 02. 2014

CASE PRESENTATION

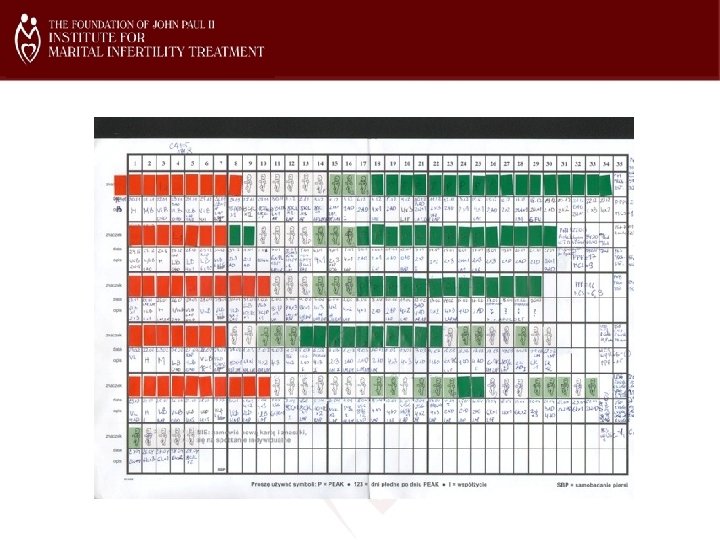
Couple nr 2 G-0 P-0 Woman age 30 Man age 32 Infertility 6 years Diagnosis on start: 21. 10. 2009 Male Infertility: sperm sample 2009: sperm count 0, 0 Past medical history: Hodgkin's lymphoma CTX 2007 Female infertility: Endometriosis LPS 2008 endometrioma AFS IV

Couple nr 2 G-0 P-0 Cr. MS from: 5. 06. 2010 Diagnosis in NPT: HUSBAND Hypogonadism, Varicocele 4, 5 mm, Valsalva maneuver (-) sperm sample 14. 04. 2010 : 0. 06 mln sperm, 15% mobility, 0%morphology, elevated viscosity sperm sample 6. 09. 2010: 12 mln sperm, 33% mobility, 18%morphology, elevated viscosity treatment: acetylcysteine sperm sample 4. 04. 2011 9 mln sperm, 35% mobility, 3%morphology, normal viscosity Treatment: tamoxifen, Testosterone undecanoate, zinc, alfa lipoic acid, l-carnitine, selenium

Couple nr 2 G-0 P-0 Cr. MS from: 5. 06. 2010 sperm sample 10. 12. 2011 after 4 month tamoxifen, Testosterone undecanoate 21 mln sperm, 26% mobility, 18%morphology, elevated viscosity Libido decrease, Hair loss treatment: acetylcysteine, zinc, alfa lipoic acid, l-carnitine, selenium


Couple nr 2 G-0 P-0 Cr. MS from: 5. 06. 2010 NPT Diagnosis: WIFE • Abnormal bleeding • Cervical Ectropion • Latent hyperprolactinemia mg treatment bromocriptine 1. 25 • Low progesterone • Limited mucus • Food Intolerance • Treatment: clomiphene HCG 2500 Peak +3, 5, 7, Vitamin B 6 , guaifenesin • Electrocoagulation/Hypherfaction

Couple nr 2 G-0 P-0 Cr. MS from: 5. 06. 2010 NPT Diagnosis: WIFE • Abnormal bleeding • Cervical Ectropion • Treatment: Policresulenum, Hyaluronan • Near contact LPS 15. 04. 2011 Frozen pelvis, endometrioma • Letrozole, Pre Seed • Psychotherapy

Couple nr 2 Cr. MS from: G-0 P-0 5. 06. 2010 • Natural conception 2 -5. 12. 2011 (follicle tracking) • Pregnancy test HCG (+) positive • Ultrasound confirms presence of fetus

Couple 2 Cr. MS from: G-0 P-0 5. 06. 2010 Baby girl 3600 g born August 12 th 2012 Caesarian Section Postpartum depression Lactation 9 month 13. 06. 2014 charting start

CASE PRESENTATION

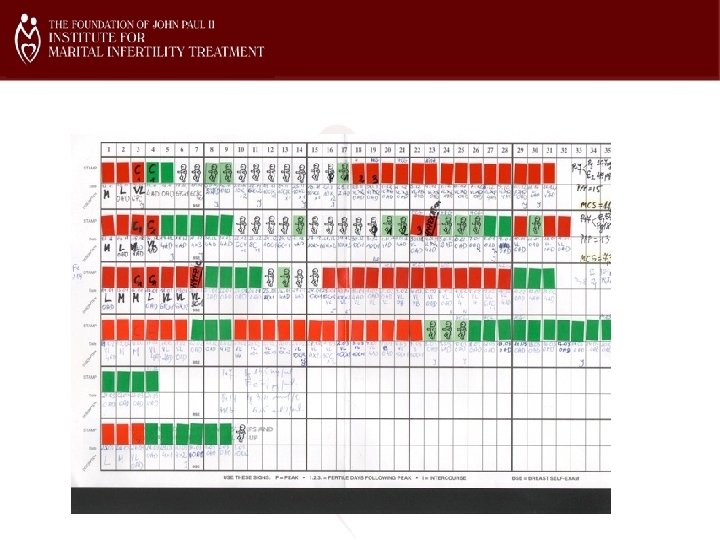
Couple nr 3 G-0 P-0 Woman age 34 Man age 35 Infertility 12 years Diagnosis on commencement of treatment: LPS 2003 ENDOMETRIOSIS, LPS 2005 TUBAL OCCLUSION, LPS 2010 ENDOMETRIOMA, adhesions, myoma, tubes patent medical treatment: Danazol, Gn. RH Analoques, Femara 1 x 1 MALE: sperm count 43 mln motility 50%, 16 % morphology IUI 2 x In vitro 1 x 2005: 5 embryos, transfer 3, kryo 1

Couple nr 3 G-0 P-0

Couple nr 3 G-0 P-0 Creighton Model : 9. 05. 2011 Na. Pro Dgn: Wife Multiple food intolerance including dairy milk, poultry egg, wheat, gluten - low carbohydrates & elimination diet latent hyperprolactinemia fasting PRL 9, 7 ng/ 219 ng after MTC vitamin D 3 12, 6 ng treatment bromocriptin, metformin, vit D 3, LDN

Couple nr 3 G-0 P-0 endometriosis IV grade

Couple nr 3 G-0 P-0 3 rd cycle - natural conception pregnancy test HCG (+) positive Ultrasound confirms presence of fetus GS 6 w 6 d CRL 6 w 3 d FHR (+) Progesterone at 6 weeks: 36, 1 ng/l estradiol 658 pmol/l EDD 16. 04. 2012 27. 03. 2012 cc Baby girl 2400 g

Couple nr 3 G-0 P-0 Baby girl 2400 g born March 27 th 2012 Caesarian Section

Research in course of realisation : 1. Quantitative and qualitative analysis of the nutrition of the patients’ group with the fertility problems and coexisting diseases: • autoimmune thyroidis (Hashimoto’s disease) • polycystic ovary syndrome (PCOS) • endometriosis 2. Clinical evaluation of elimination diet based of the results of Ig. G- dependent food hypersensitivity test (in the group of patients with the fertility problems and diagnosed coexisting autoimune disease(s): autoimmune thyroiditis and/or endometriosis)

Research in course of realisation : 3. Analysis of the serum D 3 vitamin level (25 -OH-D 3) (in the group of the women with infertility problems) 4. Establishment of the dietary standards in the diagnostics and therapy of female infertility and coexisting diseases 5. Development of educational standards regarding the dietary habits and life style in the preconception period of women with infertility problems 6. Infertility & Psychology : Stress level and quality of marital bonding 7. Retrospective treatment outcome analisys 8. i. Nest – center Number 22

Take home messages: • Immune Dysfunction • “Good” Cr. MS chart • LDN • Diet • Surgery

Correspondence address: Maciej Barczentewicz Leśna 37 20 -423 Lublin, POLAND phone: 0048 667 660 289 e-mail: maciej. barczentewicz@infertility. pl
1ef2c088559259a59f53bbdcd46ee139.ppt