

85ffaa667373bbd297b953f6d27e0ac2.ppt
- Количество слайдов: 80
 STROKE TYPES AND MANAGEMENT Filissa M Caserta MSN, ACNP-BC, CNRN The Johns Hopkins Hospital Neurosciences Critical Care Unit Baltimore Maryland
STROKE TYPES AND MANAGEMENT Filissa M Caserta MSN, ACNP-BC, CNRN The Johns Hopkins Hospital Neurosciences Critical Care Unit Baltimore Maryland
 STROKE: Defined Destruction of a portion of brain tissue as a result of circulatory failure in the distribution of a specific arterial vessel
STROKE: Defined Destruction of a portion of brain tissue as a result of circulatory failure in the distribution of a specific arterial vessel
 Epidemiology of Stroke • 5, 500, 000 stroke survivors are alive today • 700, 000 each year – 500, 000 of these are first attacks – 200, 000 are recurrent attacks. • • • Every 45 seconds, someone in the US has a stroke Every 3 minutes, someone in the US dies from a stroke 30% to 50% of stroke survivors do not regain functional independence • 15% to 30% of all stroke survivors are permanently disabled • Public awareness about the signs of stroke should be improved, so that patients and their loved ones realize when a stroke is occurring
Epidemiology of Stroke • 5, 500, 000 stroke survivors are alive today • 700, 000 each year – 500, 000 of these are first attacks – 200, 000 are recurrent attacks. • • • Every 45 seconds, someone in the US has a stroke Every 3 minutes, someone in the US dies from a stroke 30% to 50% of stroke survivors do not regain functional independence • 15% to 30% of all stroke survivors are permanently disabled • Public awareness about the signs of stroke should be improved, so that patients and their loved ones realize when a stroke is occurring
 Incidence of Stroke • • • Increases with age 28% are less than 65 yrs old 80% of strokes are preventable 19% greater in men than women Women > 65 have higher incidence than men African Americans twice as likely to have a stroke than Caucasians
Incidence of Stroke • • • Increases with age 28% are less than 65 yrs old 80% of strokes are preventable 19% greater in men than women Women > 65 have higher incidence than men African Americans twice as likely to have a stroke than Caucasians
 Stroke: Classification Two Broad Categories ISCHEMIC HEMORRHAGIC • Too little blood • Too much blood • Intracerebral Hemorrhage • Thrombotic (ICH) • Embolic • Subarachnoid Hemorrhage (SAH) • Intraventricular Hemorrhage (IVH)
Stroke: Classification Two Broad Categories ISCHEMIC HEMORRHAGIC • Too little blood • Too much blood • Intracerebral Hemorrhage • Thrombotic (ICH) • Embolic • Subarachnoid Hemorrhage (SAH) • Intraventricular Hemorrhage (IVH)
 STROKE TYPES • ISCHEMIC 84% • Thrombotic 53% • Embolic 31% • HEMORRHAGIC 16% • Intracerebral 10% • Subarachnoid 6%
STROKE TYPES • ISCHEMIC 84% • Thrombotic 53% • Embolic 31% • HEMORRHAGIC 16% • Intracerebral 10% • Subarachnoid 6%
 Circle of Willis Arteries that supply brain
Circle of Willis Arteries that supply brain
 STROKE TREATMENT • Guidelines for Prevention of Stroke in Patients With Ischemic Stroke or Transient Ischemic Attack • Guidelines for the Early Management of Adults With Ischemic Stroke • Guidelines for the Management of Spontaneous Intracerebral Hemorrhage in Adults
STROKE TREATMENT • Guidelines for Prevention of Stroke in Patients With Ischemic Stroke or Transient Ischemic Attack • Guidelines for the Early Management of Adults With Ischemic Stroke • Guidelines for the Management of Spontaneous Intracerebral Hemorrhage in Adults
 ISCHEMIC STROKE
ISCHEMIC STROKE
 Risk Factors for Ischemic Stroke AHA/ASA Guidelines Primary Prevention of Ischemic Stroke A Guideline From the American Heart Association/American Stroke Association Stroke Council. . . Stroke. 2006; 37: 1583
Risk Factors for Ischemic Stroke AHA/ASA Guidelines Primary Prevention of Ischemic Stroke A Guideline From the American Heart Association/American Stroke Association Stroke Council. . . Stroke. 2006; 37: 1583
 Risk Factors for Stroke Not Modifiable • Sex • Age • Race/ethnicity • Low birth weight • Genetics
Risk Factors for Stroke Not Modifiable • Sex • Age • Race/ethnicity • Low birth weight • Genetics
 Risk Factors for Stroke • Modifiable- well documented – – – Hypertension Heart Disease [Afib] Carotid artery stenosis Sickle cell disease Postmenopausal hormone therapy Cholesterol level Diabetes Exposure to Cigarette Smoke Poor diet Physical Activity Obesity Body fat distribution • Modifiable- Less well documented – – – ETOH abuse Drug abuse BCP Sleep disordered breathing Migraines Hyperhomocysteinemia Elevated lipoprotein-associated lipase Hypercoagulability Inflammation Infection
Risk Factors for Stroke • Modifiable- well documented – – – Hypertension Heart Disease [Afib] Carotid artery stenosis Sickle cell disease Postmenopausal hormone therapy Cholesterol level Diabetes Exposure to Cigarette Smoke Poor diet Physical Activity Obesity Body fat distribution • Modifiable- Less well documented – – – ETOH abuse Drug abuse BCP Sleep disordered breathing Migraines Hyperhomocysteinemia Elevated lipoprotein-associated lipase Hypercoagulability Inflammation Infection
 Ischemic Stroke: Types Thrombotic • Cause: Platelet Aggregation/Vessel Occlusion • Onset: During Sleep when BP is lowest • Risk Factors: – Large Vessel Disease • • • Atherosclerosis Dissection Arteritis – Small Vessel Disease • Chronic Hypertension • Lacunar : small subcortical infarcts Embolic • Cause: Fragments formed outside the brain break off and travel to a vessel in the brain • Onset: Abrupt, may occur during exercise • Risk Factors – – Afib Endocarditis Valve Disease Patent Foramen Ovale (PFO)
Ischemic Stroke: Types Thrombotic • Cause: Platelet Aggregation/Vessel Occlusion • Onset: During Sleep when BP is lowest • Risk Factors: – Large Vessel Disease • • • Atherosclerosis Dissection Arteritis – Small Vessel Disease • Chronic Hypertension • Lacunar : small subcortical infarcts Embolic • Cause: Fragments formed outside the brain break off and travel to a vessel in the brain • Onset: Abrupt, may occur during exercise • Risk Factors – – Afib Endocarditis Valve Disease Patent Foramen Ovale (PFO)
 Transient Ischemic Attack • A TIA is a rapidly reversible focal neurologic deficit that usually lasts for less than 30 minutes • Within 48 hours of the TIA there is an increased risk of stroke • A TIA workup should be given the same importance as a stroke workup • TIA is a warning sign; find the source, treat, and hopefully prevent a stroke
Transient Ischemic Attack • A TIA is a rapidly reversible focal neurologic deficit that usually lasts for less than 30 minutes • Within 48 hours of the TIA there is an increased risk of stroke • A TIA workup should be given the same importance as a stroke workup • TIA is a warning sign; find the source, treat, and hopefully prevent a stroke
 Prevention of Recurrent Ischemic Event • Guidelines for Prevention of Stroke in Patients With Ischemic Stroke or Transient Ischemic Attack – A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Council on Stroke… Stroke. 2006; 37: 577
Prevention of Recurrent Ischemic Event • Guidelines for Prevention of Stroke in Patients With Ischemic Stroke or Transient Ischemic Attack – A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Council on Stroke… Stroke. 2006; 37: 577
 Prevention of Recurrent Ischemic Event • Includes all strategies listed in primary prevention document for BP, Smoking, Lipids, DM, weight etc. . • ETOH; eliminate/reduce • Medical and/or surgical intervention for: – Arterial dissection – Patent Foramen Ovale
Prevention of Recurrent Ischemic Event • Includes all strategies listed in primary prevention document for BP, Smoking, Lipids, DM, weight etc. . • ETOH; eliminate/reduce • Medical and/or surgical intervention for: – Arterial dissection – Patent Foramen Ovale
 Prevention of Recurrent Ischemic Event • Medical management for the following: – – – Vertebrobasilar disease Intracranial atherosclerosis Atrial fibrillation Acute MI and LV thrombus Cardiomegaly Valvular disease “Cryptogenic” Infarcts Lacunar Infarcts Hypercoagulable states Hyperhomocysteinemia Cerebral venous thrombosis Pregnancy
Prevention of Recurrent Ischemic Event • Medical management for the following: – – – Vertebrobasilar disease Intracranial atherosclerosis Atrial fibrillation Acute MI and LV thrombus Cardiomegaly Valvular disease “Cryptogenic” Infarcts Lacunar Infarcts Hypercoagulable states Hyperhomocysteinemia Cerebral venous thrombosis Pregnancy
 Ischemic Penumbra • Definition: – the area surrounding the infarcted tissues that is potentially reversible – The main goal of stroke therapy is to preserve the ischemic penumbra!!!
Ischemic Penumbra • Definition: – the area surrounding the infarcted tissues that is potentially reversible – The main goal of stroke therapy is to preserve the ischemic penumbra!!!
 Management of Ischemic Stroke Guidelines for the Early Management of Adults With Ischemic Stroke A Guideline From the American Heart Association/ American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational to neurologists (Stroke. 2007; 38: 1655. )
Management of Ischemic Stroke Guidelines for the Early Management of Adults With Ischemic Stroke A Guideline From the American Heart Association/ American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational to neurologists (Stroke. 2007; 38: 1655. )
 Classification of Recommendations Class I: • Conditions for which there is evidence for and/or general agreement that the procedure or treatment is useful and effective Class II: – Conditions for which there is conflicting evidence and/or a DO’s divergence of opinion about the usefulness/efficacy of a procedure or treatment • Class IIa The weight of evidence or opinion is in favor of the procedure or treatment. • Class IIb Usefulness/efficacy is less well established by evidence or opinion. Class III D – Conditions for which there is evidence and/or general agreement O that the procedure or treatment is NOT useful/effective and in N some cases may be HARMFUL Ts
Classification of Recommendations Class I: • Conditions for which there is evidence for and/or general agreement that the procedure or treatment is useful and effective Class II: – Conditions for which there is conflicting evidence and/or a DO’s divergence of opinion about the usefulness/efficacy of a procedure or treatment • Class IIa The weight of evidence or opinion is in favor of the procedure or treatment. • Class IIb Usefulness/efficacy is less well established by evidence or opinion. Class III D – Conditions for which there is evidence and/or general agreement O that the procedure or treatment is NOT useful/effective and in N some cases may be HARMFUL Ts
 I. Pre-Hospital Management Class I • EMS • Assessment – Cincinnati Prehospital Stroke Scale – Los Angeles Prehospital Stroke Screen • Management
I. Pre-Hospital Management Class I • EMS • Assessment – Cincinnati Prehospital Stroke Scale – Los Angeles Prehospital Stroke Screen • Management
 EMS Management • • DO’s Manage ABCs Cardiac monitoring Intravenous access Oxygen (as required O 2 saturation <92%) Assess for hypoglycemia NPO Alert receiving ED Rapid transport to closest appropriate facility capable of treating acute stroke DON’T’S • Dextrose-containing fluids in nonhypoglycemic patients • Hypotension/excessive blood pressure reduction • Excessive intravenous fluids
EMS Management • • DO’s Manage ABCs Cardiac monitoring Intravenous access Oxygen (as required O 2 saturation <92%) Assess for hypoglycemia NPO Alert receiving ED Rapid transport to closest appropriate facility capable of treating acute stroke DON’T’S • Dextrose-containing fluids in nonhypoglycemic patients • Hypotension/excessive blood pressure reduction • Excessive intravenous fluids
 II. Designation of A Stroke Center Class I • Brain Attack Coalition recommended that stroke centers be established • Goal: to improve the organization and delivery of care to stroke patients • Certification through JCAHO began in 2004 – Standard measures for stroke (see end) – Primary Stroke Center (PSC) • Comprehensive Stroke Center (CPS)
II. Designation of A Stroke Center Class I • Brain Attack Coalition recommended that stroke centers be established • Goal: to improve the organization and delivery of care to stroke patients • Certification through JCAHO began in 2004 – Standard measures for stroke (see end) – Primary Stroke Center (PSC) • Comprehensive Stroke Center (CPS)
 II. Designation of A Stroke Center PSC CSC • Have personnel, • All for PSC PLUS programs, expertise and – Treat complicated strokes including ICH/IVH / SAH infrastructure to care for – Have endovascular uncomplicated strokes capabilities • Use many acute therapies – Have ICUs to manage the • Admit patient to a stroke complicated stroke patients unit • JCAHO & ASA are creating a formal process for certification
II. Designation of A Stroke Center PSC CSC • Have personnel, • All for PSC PLUS programs, expertise and – Treat complicated strokes including ICH/IVH / SAH infrastructure to care for – Have endovascular uncomplicated strokes capabilities • Use many acute therapies – Have ICUs to manage the • Admit patient to a stroke complicated stroke patients unit • JCAHO & ASA are creating a formal process for certification
 Class I • Organized") III. Emergency Evaluation and Diagnosis of Acute Ischemic Stroke (AIS) Class I • Organized protocol for emergency evaluation and treatment plan within 60 minutes • Acute stroke team to include MD/RN/ Lab/Radiology • Use of stroke rating scale (preferably NIHSS—see end) • Lab tests • Imaging
III. Emergency Evaluation and Diagnosis of Acute Ischemic Stroke (AIS) Class I • Organized protocol for emergency evaluation and treatment plan within 60 minutes • Acute stroke team to include MD/RN/ Lab/Radiology • Use of stroke rating scale (preferably NIHSS—see end) • Lab tests • Imaging
 All Patients Selected patients") III. Emergency Evaluation and Diagnosis of Acute Ischemic Stroke (AIS) All Patients Selected patients • Noncontrast brain CT or brain MRI (should not delay tx) • Blood glucose • Serum electrolytes/renal function tests • ECG • Markers of cardiac ischemia • CBC • Coags • Oxygen saturation • • • Hepatic function tests Toxicology screen Blood alcohol level Pregnancy test ABG (if hypoxia is suspected) Chest radiography (if lung disease is suspected) • Lumbar puncture (if subarachnoid hemorrhage is suspected and CT scan is negative for blood) • Electroencephalogram (if seizures are suspected)
III. Emergency Evaluation and Diagnosis of Acute Ischemic Stroke (AIS) All Patients Selected patients • Noncontrast brain CT or brain MRI (should not delay tx) • Blood glucose • Serum electrolytes/renal function tests • ECG • Markers of cardiac ischemia • CBC • Coags • Oxygen saturation • • • Hepatic function tests Toxicology screen Blood alcohol level Pregnancy test ABG (if hypoxia is suspected) Chest radiography (if lung disease is suspected) • Lumbar puncture (if subarachnoid hemorrhage is suspected and CT scan is negative for blood) • Electroencephalogram (if seizures are suspected)
 IV. Early Diagnosis: Brain and Vascular Imaging Class I • Imaging recommended prior to therapy: CT provides the info you need • Multi-modal CT and MRI can be helpful but should not delay treatment Class II • For intra-arterial rt. PA, surgery and endovascular procedures, need vascular imaging
IV. Early Diagnosis: Brain and Vascular Imaging Class I • Imaging recommended prior to therapy: CT provides the info you need • Multi-modal CT and MRI can be helpful but should not delay treatment Class II • For intra-arterial rt. PA, surgery and endovascular procedures, need vascular imaging
 Ischemic stroke on HCT
Ischemic stroke on HCT
 V. General Supportive Care and Treatment of Acute Complications Class I • ABCs • Normothermia • CV Monitoring and Treatment • BP control –HTN • BP control– Hypotension – Avoid it – Find and tx cause • Glycemic control
V. General Supportive Care and Treatment of Acute Complications Class I • ABCs • Normothermia • CV Monitoring and Treatment • BP control –HTN • BP control– Hypotension – Avoid it – Find and tx cause • Glycemic control
 V. General Supportive Care and Treatment of Acute Complications • HTN Management – Controversial because data is ambiguous, however, it is true that rapidly lowering BP does cause harm. – Not eligible for t. PA • SBP< 220 mm. Hg /or DBP < 120 mm. Hg non-t. PA – Eligible for t. PA • Pre Rx: SBP <185 or DBP <110 • Post Rx: SBP < 180 or DBP <105
V. General Supportive Care and Treatment of Acute Complications • HTN Management – Controversial because data is ambiguous, however, it is true that rapidly lowering BP does cause harm. – Not eligible for t. PA • SBP< 220 mm. Hg /or DBP < 120 mm. Hg non-t. PA – Eligible for t. PA • Pre Rx: SBP <185 or DBP <110 • Post Rx: SBP < 180 or DBP <105
 VI. Intravenous Thrombolytics Class I • IV t. PA is the only FDA approved medical therapy for patients with AIS • Other thrombolytics are NOT recommended outside of clinical trials
VI. Intravenous Thrombolytics Class I • IV t. PA is the only FDA approved medical therapy for patients with AIS • Other thrombolytics are NOT recommended outside of clinical trials
 is") VI. Intravenous Thrombolytics Intravenous rt. PA (0. 9 mg/kg, maximum dose 90 mg) is strongly recommended for carefully selected patients who can be treated within 3 hours of onset of ischemic stroke Agent • Tissue Plasminogen Activator [t-PA] Timeframe: • 3 hours for Intra. Venous Goals: • Open the occluded vessel • Re-establish blood flow • Limit injury/Improve Outcome
VI. Intravenous Thrombolytics Intravenous rt. PA (0. 9 mg/kg, maximum dose 90 mg) is strongly recommended for carefully selected patients who can be treated within 3 hours of onset of ischemic stroke Agent • Tissue Plasminogen Activator [t-PA] Timeframe: • 3 hours for Intra. Venous Goals: • Open the occluded vessel • Re-establish blood flow • Limit injury/Improve Outcome

 VII. Intra-arterial t. PA Class I • < 6 hours for selected patients who are NOT eligible for IV t. PA. • Must be at an experienced stroke center with immediate access to angio and interventionalists Class II • IA t. PA is reasonable for pts who have contraindications to IV t. PA (recent surgery, age, time frame) • Class III • Availability of IA t. PA should NOT preclude IV t. PA in eligible patients
VII. Intra-arterial t. PA Class I • < 6 hours for selected patients who are NOT eligible for IV t. PA. • Must be at an experienced stroke center with immediate access to angio and interventionalists Class II • IA t. PA is reasonable for pts who have contraindications to IV t. PA (recent surgery, age, time frame) • Class III • Availability of IA t. PA should NOT preclude IV t. PA in eligible patients
 VIII. Anticoagulants Class III • VIII. Anticoagulation – Urgent anticoagulation is NOT recommended for treatment of AIS – Should not be used in lieu of IV thrombolysis in eligible patients – Can cause hemorrhagic transformation
VIII. Anticoagulants Class III • VIII. Anticoagulation – Urgent anticoagulation is NOT recommended for treatment of AIS – Should not be used in lieu of IV thrombolysis in eligible patients – Can cause hemorrhagic transformation
 IX. Antiplatelets Class I • Aspirin : initial dose 325 mg • Given within 24 - 48 hours of stroke onset Class III • Aspirin should NOT be used as a substitute for other acute interventions, especially intravenous administration of rt. PA • ASA as an adjunctive therapy within 24 hours of rt. PA is NOT recommended • Clopidogrel alone or in conjunction with ASA is NOT recommended for AIS
IX. Antiplatelets Class I • Aspirin : initial dose 325 mg • Given within 24 - 48 hours of stroke onset Class III • Aspirin should NOT be used as a substitute for other acute interventions, especially intravenous administration of rt. PA • ASA as an adjunctive therapy within 24 hours of rt. PA is NOT recommended • Clopidogrel alone or in conjunction with ASA is NOT recommended for AIS
 X. Volume expansion/Vasodilators and Induced Hypertension Class I • Induced HTN: In “exceptional” cases, an MD may prescribe vasopressors to improve cerebral blood flow • Need close CV and neuro monitoring Class III • No hemodilution • No vasodilators (methylxanthine derivatives)
X. Volume expansion/Vasodilators and Induced Hypertension Class I • Induced HTN: In “exceptional” cases, an MD may prescribe vasopressors to improve cerebral blood flow • Need close CV and neuro monitoring Class III • No hemodilution • No vasodilators (methylxanthine derivatives)
 – Extracranial-intracranial arterial bypass") XI. Surgical Intervention • Immediate intervention – Carotid Endarterectomy (CEA) – Extracranial-intracranial arterial bypass (EC-IC bypass) • Insufficient data exists to make a recommendation
XI. Surgical Intervention • Immediate intervention – Carotid Endarterectomy (CEA) – Extracranial-intracranial arterial bypass (EC-IC bypass) • Insufficient data exists to make a recommendation
 XII. Endovascular Intervention Class II • MERCI retrieval device is reasonable in carefully selected patients although the utility of the device in improving outcomes is unclear • Other mechanical endovascular treatments should be used in the setting of clinical trials.
XII. Endovascular Intervention Class II • MERCI retrieval device is reasonable in carefully selected patients although the utility of the device in improving outcomes is unclear • Other mechanical endovascular treatments should be used in the setting of clinical trials.
 XII. Endovascular Intervention • Mechanical removal of clot – Clinical trials have shown that thrombectomy with mechanical thrombolysis devices is indeed feasible in the treatment of acute stroke. – Many devices have been discontinued – MERCI Retriever has received FDA clearance.
XII. Endovascular Intervention • Mechanical removal of clot – Clinical trials have shown that thrombectomy with mechanical thrombolysis devices is indeed feasible in the treatment of acute stroke. – Many devices have been discontinued – MERCI Retriever has received FDA clearance.
 XIII. Combination Reperfusion Therapies in AIS Class III • Combo interventions to restore perfusion are NOT recommended outside of clinical trials **Combo =Using thromolysis combined with antiplatlets/neuroprotection XIV. Neuroprotective Agents Class III • No neuroprotection agents can be recommended ** Neuroprotective agents= nimodipine, NMDA, magnesium and others
XIII. Combination Reperfusion Therapies in AIS Class III • Combo interventions to restore perfusion are NOT recommended outside of clinical trials **Combo =Using thromolysis combined with antiplatlets/neuroprotection XIV. Neuroprotective Agents Class III • No neuroprotection agents can be recommended ** Neuroprotective agents= nimodipine, NMDA, magnesium and others
 XV. Admission to Hospital & General Acute Treatment after Hospitalization Class I • • • Use of comprehensive, specialized stroke care Use of standardized stroke ordersets Early mobilization Swallow eval BEFORE eat/drink Treat UTI/pneumo with abx DVT prophylaxis with SQ anticoagulation ( as well as early mobilization and external compression devices) • Treatment of concomitant medical disease • Early intervention to prevent recurrent stroke
XV. Admission to Hospital & General Acute Treatment after Hospitalization Class I • • • Use of comprehensive, specialized stroke care Use of standardized stroke ordersets Early mobilization Swallow eval BEFORE eat/drink Treat UTI/pneumo with abx DVT prophylaxis with SQ anticoagulation ( as well as early mobilization and external compression devices) • Treatment of concomitant medical disease • Early intervention to prevent recurrent stroke
 XV. Admission to Hospital & General Acute Treatment after Hospitalization Class II • If cannot swallow, provide NG/OG/PEG nutrition • ASA is potential intervention for DVT prophylaxis, but less effective than anticoagulation. • If cannot receive anticoagulation for DVT, use external compression devices Class III • No nutritional supplements are needed for patients who can swallow • If possible, avoid using a foley due to high rosk of UTI
XV. Admission to Hospital & General Acute Treatment after Hospitalization Class II • If cannot swallow, provide NG/OG/PEG nutrition • ASA is potential intervention for DVT prophylaxis, but less effective than anticoagulation. • If cannot receive anticoagulation for DVT, use external compression devices Class III • No nutritional supplements are needed for patients who can swallow • If possible, avoid using a foley due to high rosk of UTI
 XVI. Treatment of Acute Neurological Complications Class I • Treat increased ICP as using standard interventions to decrease ICP • For risk of malignant cerebral edema, transfer to medical center with neurosurgical expertise • EVD if hydro • Decompressive surgical evacuation of spaceoccupying cerebellar infarctions • Treat recurrent seizures
XVI. Treatment of Acute Neurological Complications Class I • Treat increased ICP as using standard interventions to decrease ICP • For risk of malignant cerebral edema, transfer to medical center with neurosurgical expertise • EVD if hydro • Decompressive surgical evacuation of spaceoccupying cerebellar infarctions • Treat recurrent seizures
 XVI. Treatment of Acute Neurological Complications Class II • Although measure to decrease ICP are used, they are unproven with AIS • Decompressive Surgery for cerebral hemisphere infarct – Can be a life-saving measure – Age, side of infarct – Surgery may be recommended for seriously affected patients – If surgery is recommended, in-depth discussion with families re: potential outcomes/disability should occur.
XVI. Treatment of Acute Neurological Complications Class II • Although measure to decrease ICP are used, they are unproven with AIS • Decompressive Surgery for cerebral hemisphere infarct – Can be a life-saving measure – Age, side of infarct – Surgery may be recommended for seriously affected patients – If surgery is recommended, in-depth discussion with families re: potential outcomes/disability should occur.
 XVI. Treatment of Acute Neurological Complications Class III • NO steroids • NO prophylactic anticonvulsants Palliative Care • Ensure dialogue is occurring re: patient wishes • Advanced directives • Withdrawal of Life Support
XVI. Treatment of Acute Neurological Complications Class III • NO steroids • NO prophylactic anticonvulsants Palliative Care • Ensure dialogue is occurring re: patient wishes • Advanced directives • Withdrawal of Life Support
 Other Diagnostic Work-Up • Additional work up • LABS: TSH, RPR, Homocysteine, cholesterol, LDL, HDL, triglycerides – TESTS • Transthoracic Echo • Carotid Dopplers
Other Diagnostic Work-Up • Additional work up • LABS: TSH, RPR, Homocysteine, cholesterol, LDL, HDL, triglycerides – TESTS • Transthoracic Echo • Carotid Dopplers
 HEMORRHAGIC STROKE
HEMORRHAGIC STROKE
 – Ruptured Aneurysm • ICH (Intracerebral Hemorrhage)") Hemorrhagic Strokes: Types • SAH (Subarachnoid Hemorrhage) – Ruptured Aneurysm • ICH (Intracerebral Hemorrhage) – Hypertension – Cocaine – Many other • IVH (Intraventricular Hemorrhage) – Usually an extension of ICH – Rarely isolated
Hemorrhagic Strokes: Types • SAH (Subarachnoid Hemorrhage) – Ruptured Aneurysm • ICH (Intracerebral Hemorrhage) – Hypertension – Cocaine – Many other • IVH (Intraventricular Hemorrhage) – Usually an extension of ICH – Rarely isolated
 Risk Factors for Hemorrhagic Stroke Modifiable • HTN!!! • IVDA- cocaine/amphetamines
Risk Factors for Hemorrhagic Stroke Modifiable • HTN!!! • IVDA- cocaine/amphetamines
 ICH CAUSES • Chronic hypertension • Coagulopathy – Thrombocytopenia • Neoplasm – Malignant primary CNS – Metastatic CNS tumor – Hepatic failure • Postendarterectomy reperfusion – Factor deficiency • Sinus thrombosis/venous – Anticoagulant therapy • Trauma – Thrombolytic therapy • Vascular anomalies • Drugs – Cocaine – Sympathomimetics • Hemorrhagic transformation of cerebral infarct • Infection – Aneurysms/ Arteriovenous malformations – Vasculitis/Vasculopathy – Amyloid angiopathy – Moyamoya disease
ICH CAUSES • Chronic hypertension • Coagulopathy – Thrombocytopenia • Neoplasm – Malignant primary CNS – Metastatic CNS tumor – Hepatic failure • Postendarterectomy reperfusion – Factor deficiency • Sinus thrombosis/venous – Anticoagulant therapy • Trauma – Thrombolytic therapy • Vascular anomalies • Drugs – Cocaine – Sympathomimetics • Hemorrhagic transformation of cerebral infarct • Infection – Aneurysms/ Arteriovenous malformations – Vasculitis/Vasculopathy – Amyloid angiopathy – Moyamoya disease
 Intracerebral hemorrhages most commonly involve cerebral lobes, originating from penetrating") Intracerbral Hemorrhages Location A) Intracerebral hemorrhages most commonly involve cerebral lobes, originating from penetrating cortical branches of the anterior, middle, or posterior cerebral arteries B) Basal ganglia, originating from ascending lenticulostriate branches of the middle cerebral artery C) Thalamus, originating from ascending thalmogeniculate branches of the posterior cerebral artery D) Pons, originating from paramedian branches of the basilar artery E) Cerebellum, originating from penetrating branches of the posterior inferior, anterior inferior, or superior cerebellar arteries Spontaneous Intracerebral Hemorrhage Adnan I. Qureshi, M. D. , Stanley Tuhrim, M. D. , Joseph P. Broderick, M. D. , H. Hunt Batjer, M. D Hidek Hondo, M. D. , and Daniel F. Hanley, M. D. NEJM. Volume 344: 1450 -1460 May 10, 2001 Number 19
Intracerbral Hemorrhages Location A) Intracerebral hemorrhages most commonly involve cerebral lobes, originating from penetrating cortical branches of the anterior, middle, or posterior cerebral arteries B) Basal ganglia, originating from ascending lenticulostriate branches of the middle cerebral artery C) Thalamus, originating from ascending thalmogeniculate branches of the posterior cerebral artery D) Pons, originating from paramedian branches of the basilar artery E) Cerebellum, originating from penetrating branches of the posterior inferior, anterior inferior, or superior cerebellar arteries Spontaneous Intracerebral Hemorrhage Adnan I. Qureshi, M. D. , Stanley Tuhrim, M. D. , Joseph P. Broderick, M. D. , H. Hunt Batjer, M. D Hidek Hondo, M. D. , and Daniel F. Hanley, M. D. NEJM. Volume 344: 1450 -1460 May 10, 2001 Number 19
 ICH Management Guidelines for the Management of Spontaneous Intracerebral Hemorrhage in Adults 2007 Update: A Guideline From the American Heart Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists (Stroke. 2007; 38: 2001. )
ICH Management Guidelines for the Management of Spontaneous Intracerebral Hemorrhage in Adults 2007 Update: A Guideline From the American Heart Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists (Stroke. 2007; 38: 2001. )
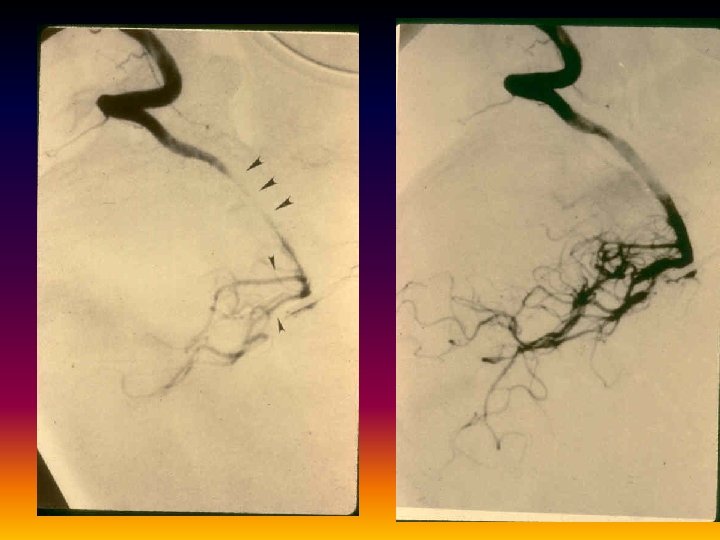
 Emergency Diagnosis and Assessment of ICH Class I • ICH is a medical emergency, with frequent early, ongoing bleeding and progressive deterioration, severe clinical deficits, and subsequent high mortality and morbidity rates, and it should be promptly recognized and diagnosed • CT and magnetic resonance are each first-choice initial imaging options; in patients with contraindications to magnetic resonance, CT should be obtained • ***Angiography- if high suspicion of vascular anomaly
Emergency Diagnosis and Assessment of ICH Class I • ICH is a medical emergency, with frequent early, ongoing bleeding and progressive deterioration, severe clinical deficits, and subsequent high mortality and morbidity rates, and it should be promptly recognized and diagnosed • CT and magnetic resonance are each first-choice initial imaging options; in patients with contraindications to magnetic resonance, CT should be obtained • ***Angiography- if high suspicion of vascular anomaly
 ICH
ICH
 IVH
IVH
 Treatment of Acute ICH/IVH Class I • Monitor in an ICU • Antiepileptic drugs (AEDs) to treat seizures • Treat and decrease fever • Early mobilization and rehab
Treatment of Acute ICH/IVH Class I • Monitor in an ICU • Antiepileptic drugs (AEDs) to treat seizures • Treat and decrease fever • Early mobilization and rehab
 Treatment of Acute ICH/IVH Class II • ICP-manage using a variety of medical therapies as well as EVD if hydro; CPP goal > 70 mm. Hg • Glycemic control (treat > 140 mg/d. L) • BP control: SBP < 180 and MAP < 130; CPP 6080 • Factor r. FVIIa • “Brief” period of prophylactic AEDs soon after ICH may decrease risk of seizures especially in lobar hemorrhage
Treatment of Acute ICH/IVH Class II • ICP-manage using a variety of medical therapies as well as EVD if hydro; CPP goal > 70 mm. Hg • Glycemic control (treat > 140 mg/d. L) • BP control: SBP < 180 and MAP < 130; CPP 6080 • Factor r. FVIIa • “Brief” period of prophylactic AEDs soon after ICH may decrease risk of seizures especially in lobar hemorrhage
 Treatment of Acute ICH/IVH • If SBP is >200 mm Hg or MAP is >150 mm Hg, then consider aggressive reduction of blood pressure with continuous IV meds monitor BP q 5 minutes. • If SBP is >180 mm Hg or MAP is >130 mm Hg and there is suspicion of increased ICP, reducing blood pressure using intermittent or continuous IV meds to keep CPP perfusion pressure >60 to 80 mm Hg • If SBP is >180 mm Hg or MAP is >130 mm Hg and no suspicion of elevated ICP, then consider a modest reduction of blood pressure (eg, MAP of 110 mm Hg or target blood pressure of 160/90 mm Hg) using intermittent or continuous intravenous medications to control blood pressure, and clinically reexamine the patient every 15 minutes.
Treatment of Acute ICH/IVH • If SBP is >200 mm Hg or MAP is >150 mm Hg, then consider aggressive reduction of blood pressure with continuous IV meds monitor BP q 5 minutes. • If SBP is >180 mm Hg or MAP is >130 mm Hg and there is suspicion of increased ICP, reducing blood pressure using intermittent or continuous IV meds to keep CPP perfusion pressure >60 to 80 mm Hg • If SBP is >180 mm Hg or MAP is >130 mm Hg and no suspicion of elevated ICP, then consider a modest reduction of blood pressure (eg, MAP of 110 mm Hg or target blood pressure of 160/90 mm Hg) using intermittent or continuous intravenous medications to control blood pressure, and clinically reexamine the patient every 15 minutes.
 Treatment of Acute ICH/IVH Class II • r. FVIIa • Treatment with r. FVIIa within the first 3 to 4 hours after onset to slow progression of bleeding has shown promise in one moderate-sized phase II trial • However, the efficacy and safety of this treatment must be confirmed in phase III trials before its use in patients with ICH can be recommended outside of a clinical trial
Treatment of Acute ICH/IVH Class II • r. FVIIa • Treatment with r. FVIIa within the first 3 to 4 hours after onset to slow progression of bleeding has shown promise in one moderate-sized phase II trial • However, the efficacy and safety of this treatment must be confirmed in phase III trials before its use in patients with ICH can be recommended outside of a clinical trial
 Prevention of DVT and PE Class I • Hemiparesis/hemiplegia ---should have intermittent pneumatic compression Class II • Prophylaxis: – after 3 -4 days – once documented bleeding has stopped – low-dose subcutaneous low-molecular-weight heparin or unfractionated heparin • Treatment – Placement of a vena cava filter – Long-term antithrombotic therapy after placement of a vena cava filter must look at risk of rebleed vs risk of thrombus
Prevention of DVT and PE Class I • Hemiparesis/hemiplegia ---should have intermittent pneumatic compression Class II • Prophylaxis: – after 3 -4 days – once documented bleeding has stopped – low-dose subcutaneous low-molecular-weight heparin or unfractionated heparin • Treatment – Placement of a vena cava filter – Long-term antithrombotic therapy after placement of a vena cava filter must look at risk of rebleed vs risk of thrombus
 ICH Related to Fibrinolysis Carries a poorer prognosis because bleeds tend to be huge Class I • Heparin---Protamine sulfate (dose depends on time heparin stopped) • Coumadin– Vitamin K IV (10 mg) with treatment to replace clotting factors Class II • Replace clotting factors – Prothrombin complex concentrate, factor IX complex concentrate, and r. FVIIa; quick and less volume – FFP; large volumes and longer infusion time
ICH Related to Fibrinolysis Carries a poorer prognosis because bleeds tend to be huge Class I • Heparin---Protamine sulfate (dose depends on time heparin stopped) • Coumadin– Vitamin K IV (10 mg) with treatment to replace clotting factors Class II • Replace clotting factors – Prothrombin complex concentrate, factor IX complex concentrate, and r. FVIIa; quick and less volume – FFP; large volumes and longer infusion time
 ICH Related to Fibrinolysis When to restart anticoagulation after ICH? ? Class II • Consider: – Risk of subsequent arterial or venous thromboembolism – Risk of recurrent ICH – Overall state of the patient • If low risk of thromboembolic event, may restart antiplatelet instead of warfarin • If warfarin must be restarted, wait 7 -10 days after ICH
ICH Related to Fibrinolysis When to restart anticoagulation after ICH? ? Class II • Consider: – Risk of subsequent arterial or venous thromboembolism – Risk of recurrent ICH – Overall state of the patient • If low risk of thromboembolic event, may restart antiplatelet instead of warfarin • If warfarin must be restarted, wait 7 -10 days after ICH
 Surgery • Surgical Approaches • Timing of Surgery • Decompressive Craniectomy • International Surgical Trial in Intracerebral Hemorrhage (STICH) • New NIH study: Minimally Invasive Stereotactic Surgery + rt. Pa for ICH Evacuation (MISTIE)
Surgery • Surgical Approaches • Timing of Surgery • Decompressive Craniectomy • International Surgical Trial in Intracerebral Hemorrhage (STICH) • New NIH study: Minimally Invasive Stereotactic Surgery + rt. Pa for ICH Evacuation (MISTIE)
 Surgical Approaches Class I • Cerebellar ICH > 3 cm with neuro deterioration /herniation or hydro should have removal of hemorrhage Class II • Lobar clots within 1 cm of the surface may be considered for standard craniotomy • Stereotactic infusion of urokinase into clot – decreases size of clot and risk of death BUT it’s usefulness is UNKNOWN • Minimally invasive clot evacuation via mechanical devices – needs further testing therefore it’s usefulness is UNKNOWN Class III • Evacuation of supratentorial ICH by standard craniotomy within 96 hours is NOT RECOMMENDED except as noted above
Surgical Approaches Class I • Cerebellar ICH > 3 cm with neuro deterioration /herniation or hydro should have removal of hemorrhage Class II • Lobar clots within 1 cm of the surface may be considered for standard craniotomy • Stereotactic infusion of urokinase into clot – decreases size of clot and risk of death BUT it’s usefulness is UNKNOWN • Minimally invasive clot evacuation via mechanical devices – needs further testing therefore it’s usefulness is UNKNOWN Class III • Evacuation of supratentorial ICH by standard craniotomy within 96 hours is NOT RECOMMENDED except as noted above
 Decompressive Craniectomy Class II • Too few data currently exist to comment on the potential of decompressive craniectomy to improve outcome in ICH
Decompressive Craniectomy Class II • Too few data currently exist to comment on the potential of decompressive craniectomy to improve outcome in ICH
 Withdrawal of Life Support • We recommend careful consideration of aggressive full care during the first 24 hours after ICH onset and postponement of NEW DNR orders during that time. • In all cases, physicians and nurses caring for ICH patients who are given DNR status should be reminded that the designation relates only to the circumstance of cardiopulmonary arrest and that patients should receive all other appropriate medical and surgical interventions.
Withdrawal of Life Support • We recommend careful consideration of aggressive full care during the first 24 hours after ICH onset and postponement of NEW DNR orders during that time. • In all cases, physicians and nurses caring for ICH patients who are given DNR status should be reminded that the designation relates only to the circumstance of cardiopulmonary arrest and that patients should receive all other appropriate medical and surgical interventions.
 Prevention of Recurrent ICH Class I • Treating hypertension in the nonacute setting is the most important step to reduce the risk of ICH and probably recurrent ICH as well • Smoking, heavy alcohol use, and cocaine use are risk factors for ICH, and discontinuation should be recommended for prevention of ICH recurrence
Prevention of Recurrent ICH Class I • Treating hypertension in the nonacute setting is the most important step to reduce the risk of ICH and probably recurrent ICH as well • Smoking, heavy alcohol use, and cocaine use are risk factors for ICH, and discontinuation should be recommended for prevention of ICH recurrence
 • 72 yo white male • PMHx: Case Study – Mild HTN • Meds – Lisinopril 10 mg qday • Family Hx – – Mom- s/p cva Dad- s/p cva x 2 • Social – MS in Civil Engineering – Working as tunnel expert FHWA
• 72 yo white male • PMHx: Case Study – Mild HTN • Meds – Lisinopril 10 mg qday • Family Hx – – Mom- s/p cva Dad- s/p cva x 2 • Social – MS in Civil Engineering – Working as tunnel expert FHWA
 Case Study • • • Home alone “Didn’t feel well” Sudden onset right sided weakness Called 911—could he talk? ? EMS Arrives---house locked—tic-toc t. PA minutes!! • Establish TOSO? ?
Case Study • • • Home alone “Didn’t feel well” Sudden onset right sided weakness Called 911—could he talk? ? EMS Arrives---house locked—tic-toc t. PA minutes!! • Establish TOSO? ?
 Case Study • Since could not establish TOSO, no thrombolytics • Cause? – Undiagnosed afib with SLOW ventricular response • Rx – Pacemaker – Heparin--- Coumadin – Acute rehab after 72 hours! • Rehab – Acute 30 days – Day Hospital 2 months - Subacute 3 months - Outpatient
Case Study • Since could not establish TOSO, no thrombolytics • Cause? – Undiagnosed afib with SLOW ventricular response • Rx – Pacemaker – Heparin--- Coumadin – Acute rehab after 72 hours! • Rehab – Acute 30 days – Day Hospital 2 months - Subacute 3 months - Outpatient
 PRE STROKE HAWAII 1996
PRE STROKE HAWAII 1996
 POST STROKE HAWAII 2005
POST STROKE HAWAII 2005
 THERE IS LIFE AFTER STROKE!!
THERE IS LIFE AFTER STROKE!!
 Cincinnati Prehospital Stroke Scale Last time seen normal ________ Evaluate for Facial Droop Present? Absent? Hold up arms and look for Drift Present? Absent? Repeat “The sky is blue in Cincinnati. Abnormal? Normal? BP_____ Blood sugar______ History of anticoagulant medications ? Warfarin_____ Heparin ____ Patients with 1 of these 3 findings -as a new event - have a 66% probability of an ischemic stroke. If all 3 findings are present the probability of an acute stroke is more than 88%
Cincinnati Prehospital Stroke Scale Last time seen normal ________ Evaluate for Facial Droop Present? Absent? Hold up arms and look for Drift Present? Absent? Repeat “The sky is blue in Cincinnati. Abnormal? Normal? BP_____ Blood sugar______ History of anticoagulant medications ? Warfarin_____ Heparin ____ Patients with 1 of these 3 findings -as a new event - have a 66% probability of an ischemic stroke. If all 3 findings are present the probability of an acute stroke is more than 88%
 Los Angeles Prehospital Stroke Screen • Last time patient known to be symptom free • Screening – – – Age >45 y No history of seizures or epilepsy Symptoms present <24 h Not previously bedridden or wheelchair bound If unknown or yes • Blood glucose 60 to 400 mg/d. L Yes No Examination • Exam – Facial smile grimace – Grip – Arm strength (drift) • Based on examination, patient has unilateral weakness Yes No • If items are yes or unknown, meets criteria for stroke
Los Angeles Prehospital Stroke Screen • Last time patient known to be symptom free • Screening – – – Age >45 y No history of seizures or epilepsy Symptoms present <24 h Not previously bedridden or wheelchair bound If unknown or yes • Blood glucose 60 to 400 mg/d. L Yes No Examination • Exam – Facial smile grimace – Grip – Arm strength (drift) • Based on examination, patient has unilateral weakness Yes No • If items are yes or unknown, meets criteria for stroke
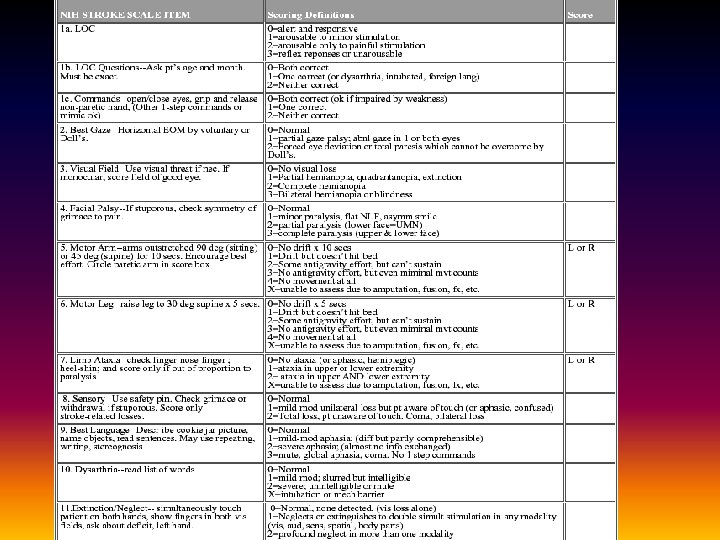
 – The initial NIHSS score") NIHSS • National Institutes of Health Stroke Scale (NIHSS) – The initial NIHSS score provides important prognostic information. – Approximately 60% to 70% of patients with an acute ischemic stroke and a baseline NIHSS score <10 will have a favorable outcome after 1 year as compared with only 4% to 16% of those with a score >20. – The NIHSS score can also help identify those patients at greatest risk for ICH associated with thrombolytic treatment.
NIHSS • National Institutes of Health Stroke Scale (NIHSS) – The initial NIHSS score provides important prognostic information. – Approximately 60% to 70% of patients with an acute ischemic stroke and a baseline NIHSS score <10 will have a favorable outcome after 1 year as compared with only 4% to 16% of those with a score >20. – The NIHSS score can also help identify those patients at greatest risk for ICH associated with thrombolytic treatment.
 Designation of A Stroke Center JCAHO Standard Measures • t. PA considered • Screen for dysphagia • Deep vein thrombosis prophylaxis • Lipid profile during hospitalization • Smoking cessation • Education about stroke • Plan for rehabilitation considered • Antithrombotic medications started within 48 hours • Antithrombotic medications prescribed at discharge • Anticoagulants prescribed to patients with a-fib
Designation of A Stroke Center JCAHO Standard Measures • t. PA considered • Screen for dysphagia • Deep vein thrombosis prophylaxis • Lipid profile during hospitalization • Smoking cessation • Education about stroke • Plan for rehabilitation considered • Antithrombotic medications started within 48 hours • Antithrombotic medications prescribed at discharge • Anticoagulants prescribed to patients with a-fib