16b23a28d92eb99c7a1c5d044ee5393d.ppt
- Количество слайдов: 60



SPINE SBRT: The MSKCC Spine Service IAEA Singapore SBRT Symposium Josh Yamada MD FRCPC Mark Bilsky MD Departments of Radiation Oncology and Neurosurgery Memorial Sloan Kettering Cancer Center NY NY USA

Disclosures Varian Medical Systems Consultant Continuing Medical Education Institute Speakers Bureau

MSKCC Spine Service Radiation Oncology Josh Yamada, M. D. Radiology Eric Lis, M. D. George Krol, M. D. Sasan Karimi, M. D. Pierre Gobin, M. D. Athos Patsilides, M. D. Orthopedic Surgery Patrick Boland, M. D. Neurosurgery Mark Bilsky, M. D. Ilya Laufer, M. D. Neurology Edward Avila, D. O. Xi Chen, M. D. Sonia Sandhu, D. O Physiatry Michael Stubblefield, M. D. Jonas Sokolof, D. O. Christian Custodio, M. D. PT/OT Nursing Joan Zatcky, NP Cynthia Correa, RN Ruth Gargan-Klinger, NP Pain Jane Yoffe, NP Solange Inglis, NP Roma Tickoo, M. D. Marie Marte, NP Kenneth Cubert, M. D. Vinay Puttaniah, M. D. Amitabh Gulati, M. D.

Goals of Treatment Multi-disciplinary Approach • Metastasis • Palliation ØPain Control ØNeurology ØOncology ØMechanical Stability

The Spine Service at MSKCC: Multidisciplinary Care • Spine oncology requires multidisciplinary care • Spine conference • All physicians in the hospital bring their spine patient questions for multidisciplinary assessment—meets weekly • Spine clinic • Joint clinic with neurosurgery, interventional radiology and radiation oncology • NOMS assessment

Treatment Considerations NOMS 1, 2 • Neurologic • Systemic Therapy • Oncologic • Radiation Therapy • Mechanical Stability • Surgery • Systemic disease vs. 1 Bilsky MH, Smith M. Surgical approach to epidural spinal cord compression. Hematology/Oncology Clinics of North America. ; 20(6): 1307 -1317, 2006 2 Bilsky MH, Azeem S. The NOMS framework for decision making in metastatic cervical spine tumors. Current Opinions in Orthopedics 2007; 18(3): 263 -269.

Options for Therapy Multi-disciplinary Approach • Systemic Therapy • Chemo/Immuno-/Hormonal therapy • Targeted Therapy • Radiation Therapy • Conventional EBRT (30 Gy in 10 fractions) • Image-guided intensity modulated RT o Hypofractionated RT (10 Gy x 3) o Single Fraction RT (24 Gy) • Brachytherapy: p 32 plaque • Surgery – Percutaneous Cement Augmentation • Open: Anterior, Posterolateral, Combined • En bloc resection for margins

Presentation • Three Predominant Pain Syndromes: ØBiologic ØMechanical ØRadiculopathy • Myelopathy • Significant treatment implications
")
Presentation • Biologic pain • Indicative of bone pathology • Predominant pain syndrome (95%) • Night or morning pain that resolves over the course of the day • Mechanism: Diurnal variation in endogenous steroid secretion • Treatment: Steroids/RT

Presentation • Mechanical Pain • Indicative of bone pathology • Movement-related pain • Level dependent ØAA: Flexion/extension/rotation ØSAC: Flexion/extension ØThoracic: Extension ØLumbar: Mechanical Radiculopathy • Radiographic correlates • Treatment: Surgery or Kyphoplasty followed by RT

Presentation • Radiculopathy • Indicative of neuroforaminal disease • Differentiate from the following: ØBone lesion (eg. L 3 vs. femur fracture) ØNeuropathy ØBrachial/Lumbosacral Plexus Tumor ØLeptomeningeal Tumor • Treatment: Dependent on tumor histology and degree of ESCC, often RT in absence of instability
 ØCorticospinal tracts (Motor)")
Presentation • Myelopathy: • Indicative of high-grade ESCC ØSpinothalamic tracts (Pinprick) ØCorticospinal tracts (Motor) ØPosterior Columns (Proprioception) ØAutonomic (Bowel and Bladder) ü Neurogenic vs. other (eg. narcotics) ü Perineal numbness ü Conus medullaris or sacrum ü Other spinal levels: Significant degree of paralysis ØTreatment: Dependent on the radiosensitivity of the tumor

NOMS Assessment • Neurologic • Myelopathy • Functional Radiculopathy • Degree of epidural spinal cord compression • Oncologic • Tumor Histology • Radiation or Chemosensitivity • Mechanical Instability • Systemic Disease and Medical Co-morbidity

NOMS N: ESCC 0 2 1 3 O: Radiation Sensitivity Radiation Tumor Sensitivity Histology Sensitive Moderately Sensitive Moderately Resistant Highly Resistant Myeloma Lymphoma Breast Colon NSCLC Thyroid Renal Sarcoma Melanoma

NOMS N: ESCC 0 2 O: Radiation Sensitivity 1 3 c. EBRT 30 Gy in 3 Gy/fraction Radiation Tumor Sensitivity Histology Sensitive Moderately Sensitive Moderately Resistant Highly Resistant Myeloma Lymphoma Breast Colon NSCLC Thyroid Renal Sarcoma Melanoma

NOMS N: ESCC 0 2 1 3 SRS O: Radiation Sensitivity Radiation Tumor Sensitivity Histology Sensitive Moderately Sensitive Moderately Resistant Highly Resistant Myeloma Lymphoma Breast Colon NSCLC Thyroid Renal Sarcoma Melanoma

NOMS N: ESCC 0 2 O: Radiation Sensitivity 1 3 Surgery + SRS Radiation Tumor Sensitivity Histology Sensitive Moderately Sensitive Moderately Resistant Highly Resistant Myeloma Lymphoma Breast Colon NSCLC Thyroid Renal Sarcoma Melanoma
 Lymphoma Seminoma Breast Prostate")
Histologic Classification Radiosensitivity to c. EBRT (30 Gy in 10) Lymphoma Seminoma Breast Prostate Myeloma Sarcoma Melanoma GI NSCLC Renal Gilbert F F U U U Maranzano F F F U U U Rades F I I I U I Rades F F F U U U Katagiri F F F U U U Maranzano F F F U U U Rades F I I I U I Responses: F-Favorable, I-Intermediate, U-Unfavorable Gerszten PC, Mendel E, Yamada Y. Radiotherapy and radiosurgery for metastatic spine disease: What are the options, indications, and outcomes. Spine 34(22 S): S 78 -92, 2009

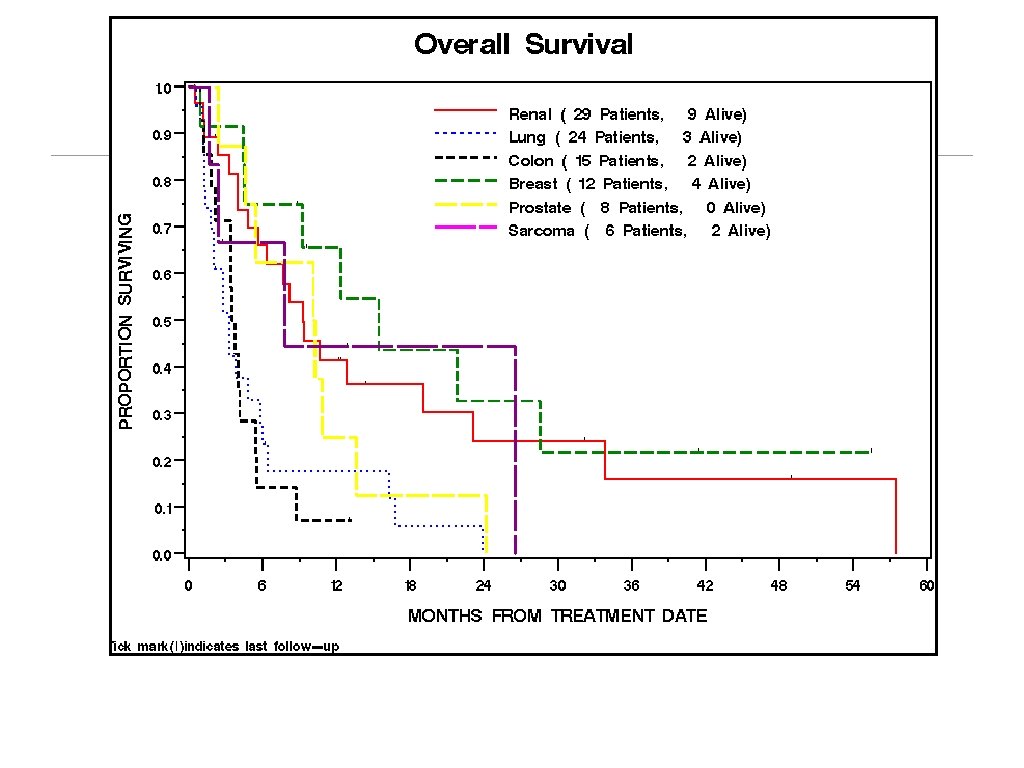
Local Control Histology 413 patients Histology 3 Yr Local Control Breast 98% GI 98% H&N 93% Lung 98% Melanoma 90% Unknown 91% Prostate 98% Renal 89% Sarcoma 96% Thyroid 92%

Radiosurgery Recommendations A strong recommendation can be made with low-quality evidence that radiosurgery should be considered over conventional fractionated radiotherapy for the treatment of solid tumor spine metastases in the setting of oligometastatic disease and/or radioresistant histology in which no relative contraindications exist. Gerszten PC, Mendel E, Yamada Y. Radiotherapy and radiosurgery for metastatic spine disease: What are the options, indications, and outcomes. Spine 34(22 S): S 78 -92, 2009

Case Solitary T 10 RCC

RCC/Melanoma Stereotactic Radiosurgery • 80 patients • 2004 -2008 • SSRS 18 to 24 Gy x 1 • Imaging and PE q 4 months • Radiographic/Symptom Control: 92% • Trend towards better control at 24 Gy: 97% vs. 83% Thiagaragan A, et. al. Stereotactic radiosurgery: A new paradigm For melanoma and renal cell carcinoma spine metastases. Presented ASCO, 2010

NOMS Assessment • Neurologic • Myelopathy • Functional Radiculopathy • Degree of epidural spinal cord compression • Oncologic • Tumor Histology: RCC • Radiation or Chemosensitivity • Mechanical Instability

NOMS Assessment • Neurologic • Myelopathy • Functional Radiculopathy • Degree of epidural spinal cord compression: ESCC 1 b • Oncologic • Tumor Histology: RCC • Radiation: Sensitive to SRS • Mechanical Stability: Stable • Systemic Disease and Medical Co-morbidity SR S

RCC SRS: 24 Gy, Cord d. Max: 14 Gy f/u in 26 Treatment of Metastatic months Bilsky M, , et. al. Shifting Paradigms the Spine Disease. Spine. 34(22 S) Supplement: S 101 -S 107, 2009.

RCC A strong recommendation is made that patients with solid renal cell carcinoma in the absence of epidural disease may benefit from stereotactic radiosurgery as first line therapy rather than en bloc excision. SRS: 24 Gy, Cord d. Max: 14 Gy f/u 26 months Bilsky M, , et. al. Shifting Paradigms in the Treatment of Metastatic Spine Disease. Spine. 34(22 S) Supplement: S 101 -S 107, 2009.

NOMS N: ESCC 0 2 O: Radiation Sensitivity 1 3 Surgery + SRS Radiation Tumor Sensitivity Histology Sensitive Moderately Sensitive Moderately Resistant Highly Resistant Myeloma Lymphoma Breast Colon NSCLC Thyroid Renal Sarcoma Melanoma

SRS and High-Grade ESCC • 7 local failures received <15 Gy to small percentage of PTV • Currently, d. Max Cord <14 Gy with 10% per mm falloff: ØCytotoxic tumoral dose risks overdosing the spinal cord ØSubtherapeutic dose that spares spinal cord tolerance risks epidural tumor progression • Resolution of soft tissue disease can take months: Under-dosed sub-volume No effective decompression of epidural disease • Caveat: SRS for RT-sensitive disease (Median 16 Gy)1 Cord Tumor (gross target volume) 1 Ryu S. , et. al Radiosurgical decompression of metastatic epidural compression. Cancer 116(9): 2250, 2010 Prescription isodose

Neurologic Oncologic Assessment • Prospective randomized trial • Solid tumors • HG-ESCC with myelopathy • Surgery + c. EBRT vs. c. EBRT alone • Exclusion criteria • RT-sensitive tumors ie. Hematologic malignancies and GCT • Multi-level disease • Systemic contraindications to surgery RA Patchell, et al. , Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomized trial. Lancet 366: 643, 2005
 57% (29/51) p=. 001 Duration 122")
Results Surgery Radiation Significance Overall Ambulation 84% (42/50) 57% (29/51) p=. 001 Duration 122 days 13 days p=. 003 Recover Ambulation 62% (10/16) 19% (3/16) p=. 012 Continence 155 days 17 days p=. 016 Narcotics (MSO 4) . 4 mgs 4 -8 mgs p=. 002 126 days 100 days p=. 033 Survival Time RA Patchell, et al. , Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomized trial. Lancet 366: 643, 2005
 57% (29/51) p=. 001 Duration 122")
Results Surgery Radiation Significance Overall Ambulation 84% (42/50) 57% (29/51) p=. 001 Duration 122 days 13 days p=. 003 Recover Ambulation 62% (10/16) 19% (3/16) p=. 012 Continence 155 days 17 days p=. 016 Narcotics (MSO 4) . 4 mgs 4 -8 mgs p=. 002 126 days 100 days p=. 033 Survival Time Evidence-based Recommendations (GRADE methodology) : A strong recommendation is made for patients with high-grade spinal cord compression due to solid tumor malignancy undergo surgical decompression and stabilization followed by RT. 1 Bilsky M, , et. al. Shifting Paradigms in the Treatment of Metastatic Spine Disease. Spine 34(22 S): S 101 -S 107, 2009

Radiosurgery Recommendations A strong recommendation can be made with low-quality evidence that radiosurgery should be considered over conventional fractionated radiotherapy for the treatment of solid tumor spine metastases in the setting of oligometastatic disease and/or radioresistant histology in which no relative contraindications exist. Gerszten PC, Mendel E, Yamada Y. Radiotherapy and radiosurgery for metastatic spine disease: What are the options, indications, and outcomes. Spine 34(22 S): S 78 -92, 2009

Postoperative Adjuvant Radiation • 101 patients/106 metastases operated between 1977 to 1996 • Surgery: ØPosterolateral: 79% ØAnterior: 12% ØCombined Anterior/Posterior: 9% ØPartial (48%) or Complete Resection (43%): 91% • Adjuvant Treatment: 100% • Local Control: 40% @ 6 months 30% @ 1 year 4% @ 4 years • Significant Predictors of Recurrence: Ø Ambulation, Tumor Histology, Completeness of Klekamp J, Samii. Surgical results for spinal metastases. Resection Acta Neurochir (Wien) 140 (9): 957 -967, 1998

Postoperative Adjuvant Radiation • MSKCC Data: 21 patients • RT-resistant tumors: 100% ØMelanoma ØRenal Cell Carcinoma ØSarcoma ØColorectal Carcinoma • Surgical Indication: ØHigh Grade ESCC (Grade 2 or 3): 96% ØMechanical Radiculopathy: 4% • SRS Single Fraction: 18 to 24 Gy Ø GTV contoured to the preoperative tumor volume Ø Myelogram/CT Moulding, et. al. Local disease control after decompressive surgery and high-dose single fraction radiation for spine metastases. J Neurosurg Spine 13(1): 87 -93, 2010

Local Control Surgery + SRS LD: 40% HD: 94% Moulding, et. al. Local disease control after decompressive surgery and adjuvant high-dose single fraction radiation for spine metastases. J Neurosurg Spine 13(1): 87 -93, 2010

Local Control Separation Surgery + SRS 192 pts. SRS: 90% Hypo LD: 78% Hypo HD: 95. 8%

“Separation Surgery” + SRS 86 year old Papillary thyroid ASIA C Absent proprioception N: HG ESCC O: RT-resistant M: Stable S: Tolerable

“Separation Surgery” + SRS

RCC En bloc excision • Published literature: • 6 case series: 15 patients • Operative times: 8 to 12 hours • Transfusion data: Melcher - PRBC-15. 7 units/FFP 20 units • No complications reported • Bilsky M, et. al. Shifting Paradigms in the Treatment of Metastatic Recurrences: 13% Spine Disease. Spine. 34(22 S) Supplement: S 101 -S 107, 2009. • Median follow-up 16 2

“Separation Surgery” + SRS • SST post RT/Chemo • Tumor progression with instability • T 3 vertebral body • Massive brachial plexus • N: ESCC 2 Radiculopathy/plexopathy • O: Resistant • M: Unstable • S: Tolerate an operation

NOMS Assessment • Neurologic • Myelopathy • Functional Radiculopathy • Degree of epidural spinal cord compression • Oncologic • Tumor Histology: RCC • Radiation or Chemosensitivity • Mechanical Stability

NOMS Assessment • Neurologic • Myelopathy • Functional Radiculopathy • Degree of epidural spinal cord compression • Oncologic • Tumor Histology: RCC • Radiation or Chemosensitivity • Mechanical Stability

NOMS Assessment • Neurologic • Myelopathy • Functional Radiculopathy • Degree of epidural spinal cord compression • Oncologic • Tumor Histology: RCC • Radiation or Chemosensitivity • Mechanical Stability • Systemic Disease and Medical Co-morbidity High-dose steroids Embolization

NOMS Assessment • Neurologic • Myelopathy • Functional Radiculopathy • Degree of epidural spinal cord compression • Oncologic • Tumor Histology: RCC • Radiation or Chemosensitivity • Mechanical Stability • Systemic Disease and Medical Co-morbidity Posterolateral decompression Instrumentation /SRS + /p 32 plaque

NOMS Assessment • Neurologic • Myelopathy • Functional Radiculopathy • Degree of epidural spinal cord compression • Oncologic • Tumor Histology: Lymphoma • Radiation or Chemosensitivity • Mechanical Stability • Systemic Disease and Medical Co-morbidity

NOMS Assessment • Neurologic • Myelopathy • Functional Radiculopathy • Degree of epidural spinal cord compression • Oncologic • Tumor Histology: Lymphoma • Radiation or Chemosensitivity • Mechanical Stability • Systemic Disease and Medical Co-morbidity High-dose steroids c. EBRT (30 Gy in 10 fractions)

NOMS Assessment • Neurologic • Myelopathy • Functional Radiculopathy • Degree of epidural spinal cord compression • Oncologic • Tumor Histology: Unknown • Radiation or Chemosensitivity • Mechanical Stability • Systemic Disease and Medical Co-morbidity

NOMS Assessment • Neurologic • Myelopathy • Functional Radiculopathy • Degree of epidural spinal cord compression • Oncologic • Tumor Histology: Unknown • Radiation or Chemosensitivity • Mechanical Stability • Systemic Disease and Medical Co-morbidity High-dose steroids Establish RT-sensitive: RT No Dx: Surgery

NOMechanical Instability. S • Recognition of instability as an indication for surgery or percutaneous cement augmentation prior to RT • Spine Oncology Study Group (SOSG) created a scoring system Spine Instability Neoplastic Score or SINS 1 -Integrates systematic literature review with expert opinion -Reliable: High inter and intra-relater reliability 2 -Valid: Substantial agreement between SINS score and expert opinion 2 1 Fisher CG, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. . Spine. 2010; 35(22): E 1221 -9. 2 Fourney DR, et al. Spinal instability neoplastic score: an analysis of reliability and validity from the spine oncology study group. J Clin Oncol 2011; 29(22): 3072 -71
 SINS Component Description Score Location Junctional (Occ-C 2, C")
Spine Instability Neoplastic Score (SINS) SINS Component Description Score Location Junctional (Occ-C 2, C 7 -T 2, T 11 -L 1, L 5 -S) Mobile (C 3 -6, L 2 -4) Semirigid (T 3 -10) Rigid (S 2 -5) 3 2 1 0 Yes* Occasional non-mechanical pain No 3 1 0 Bone Lesion Lytic Mixed Blastic 2 1 0 Alignment Subluxation / translation De novo deformity Normal 4 2 0 Vertebral Body >50% collapse <50% collapse No collapse with >50% VB involved None of above 3 2 1 0 Posterolateral Involvement Bilateral Unilateral 3 1 Pain Tallied Score from 6 components Stable 0 -6 Potentially Unstable 7 -12 13 -18 Fisher CG, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine 35(22): E 1221 -9, 2010
 SINS Component Description Score Location Junctional (Occ-C 2, C")
Spine Instability Neoplastic Score (SINS) SINS Component Description Score Location Junctional (Occ-C 2, C 7 -T 2, T 11 -L 1, L 5 -S) Mobile (C 3 -6, L 2 -4) Semirigid (T 3 -10) Rigid (S 2 -5) 3 2 1 0 Yes* Occasional non-mechanical pain No 3 1 0 Bone Lesion Lytic Mixed Blastic 2 1 0 Alignment Subluxation / translation De novo deformity Normal 4 2 0 Vertebral Body >50% collapse <50% collapse No collapse with >50% VB involved None of above 3 2 1 0 Posterolateral Involvement Bilateral Unilateral None 3 1 0 Pain Tallied Score from 6 components Stable 0 -6 Potentially Unstable 7 -12 13 -18 Fisher CG, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine 35(22): E 1221 -9, 2010
 SINS Component Description Score Location Junctional (Occ-C 2, C")
Spine Instability Neoplastic Score (SINS) SINS Component Description Score Location Junctional (Occ-C 2, C 7 -T 2, T 11 -L 1, L 5 -S) Mobile (C 3 -6, L 2 -4) Semirigid (T 3 -10) Rigid (S 2 -5) 3 2 1 0 Yes* Occasional non-mechanical pain No 3 1 0 Bone Lesion Lytic Mixed Blastic 2 1 0 Alignment Subluxation / translation De novo deformity Normal 4 2 0 Vertebral Body >50% collapse <50% collapse No collapse with >50% VB involved None of above 3 2 1 0 Posterolateral Involvement Bilateral Unilateral None 3 1 0 Pain Tallied Score from 6 components Stable 0 -6 Potentially Unstable 7 -12 13 -18 Fisher CG, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine 35(22): E 1221 -9, 2010
 SINS Component Description Score Location Junctional (Occ-C 2, C")
Spine Instability Neoplastic Score (SINS) SINS Component Description Score Location Junctional (Occ-C 2, C 7 -T 2, T 11 -L 1, L 5 -S) Mobile (C 3 -6, L 2 -4) Semirigid (T 3 -10) Rigid (S 2 -5) 3 2 1 0 Yes* Occasional non-mechanical pain No 3 1 0 Bone Lesion Lytic Mixed Blastic 2 1 0 Alignment Subluxation / translation De novo deformity Normal 4 2 0 Vertebral Body >50% collapse <50% collapse No collapse with >50% VB involved None of above 3 2 1 0 Posterolateral Involvement Bilateral Unilateral None 3 1 0 Pain Tallied Score from 6 components Stable 0 -6 Potentially Unstable 7 -12 13 -18 Fisher CG, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine 35(22): E 1221 -9, 2010
 SINS Component Description Score Location Junctional (Occ-C 2, C")
Spine Instability Neoplastic Score (SINS) SINS Component Description Score Location Junctional (Occ-C 2, C 7 -T 2, T 11 -L 1, L 5 -S) Mobile (C 3 -6, L 2 -4) Semirigid (T 3 -10) Rigid (S 2 -5) 3 2 1 0 Yes* Occasional non-mechanical pain No 3 1 0 Bone Lesion Lytic Mixed Blastic 2 1 0 Alignment Subluxation / translation De novo deformity Normal 4 2 0 Vertebral Body >50% collapse <50% collapse No collapse with >50% VB involved None of above 3 2 1 0 Posterolateral Involvement Bilateral Unilateral None 3 1 0 Pain Tallied Score from 6 components Stable 0 -6 Potentially Unstable 7 -12 13 -18 Fisher CG, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine 35(22): E 1221 -9, 2010
 SINS Component Description Score Location Junctional (Occ-C 2, C")
Spine Instability Neoplastic Score (SINS) SINS Component Description Score Location Junctional (Occ-C 2, C 7 -T 2, T 11 -L 1, L 5 -S) Mobile (C 3 -6, L 2 -4) Semirigid (T 3 -10) Rigid (S 2 -5) 3 2 1 0 Yes* Occasional non-mechanical pain No 3 1 0 Bone Lesion Lytic Mixed Blastic 2 1 0 Alignment Subluxation / translation De novo deformity Normal 4 2 0 Vertebral Body >50% collapse <50% collapse No collapse with >50% VB involved None of above 3 2 1 0 Posterolateral Involvement Bilateral Unilateral None 3 1 0 Pain Tallied Score from 6 components Stable 0 -6 Potentially Unstable 7 -12 13 -18 Fisher CG, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine 35(22): E 1221 -9, 2010
 SINS Component Description Score Location Junctional (Occ-C 2, C")
Spine Instability Neoplastic Score (SINS) SINS Component Description Score Location Junctional (Occ-C 2, C 7 -T 2, T 11 -L 1, L 5 -S) Mobile (C 3 -6, L 2 -4) Semirigid (T 3 -10) Rigid (S 2 -5) 3 2 1 0 Yes* Occasional non-mechanical pain No 3 1 0 Bone Lesion Lytic Mixed Blastic 2 1 0 Alignment Subluxation / translation De novo deformity Normal 4 2 0 Vertebral Body >50% collapse <50% collapse No collapse with >50% VB involved None of above 3 2 1 0 Posterolateral Involvement Bilateral Unilateral None 3 1 0 Pain Tallied Score from 6 components Stable 0 -6 Potentially Unstable 7 -12 13 -18 Fisher CG, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine 35(22): E 1221 -9, 2010
 SINS Component Description Score Location Junctional (Occ-C 2, C")
Spine Instability Neoplastic Score (SINS) SINS Component Description Score Location Junctional (Occ-C 2, C 7 -T 2, T 11 -L 1, L 5 S 1) Mobile (C 3 -6, L 2 -4) Semirigid (T 3 -10) Rigid (S 2 -5) 3 2 1 0 Yes* Occasional non-mechanical pain No 3 1 0 Bone Lesion Lytic Mixed Blastic 2 1 0 Alignment Subluxation / translation De novo deformity Normal 4 2 0 Vertebral Body >50% collapse <50% collapse No collapse with >50% VB involved None of above 3 2 1 0 Posterolateral Involvement Bilateral Unilateral 3 1 Pain Tallied Score from 6 components Stable 0 -6 Potentially Unstable 7 -12 13 -18 Fisher CG, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine 35(22): E 1221 -9, 2010

SRS NOMS Algorithm

Summary • NOMS provides a comprehensive approach to the multidisciplinary management of spine metastases • Metastatic cancer patients are a unique cohort • Integration of new technologies and therapeutic options • Most effective and low impact = best palliatiion • NOMS provides a vehicle for surgeons, medical and radiation oncologists to speak a common language
16b23a28d92eb99c7a1c5d044ee5393d.ppt