

dc91239604d64efc477963951c555bab.ppt
- Количество слайдов: 27
 Sexual Health Matters…. Sex, Sexuality, Pleasure, STIs and Public Health Dr David M Lee Honorary Fellow in Sexual Health The University of Melbourne & Ms. Sheranne Dobinson Sexual Health Nurse Melbourne Sexual Health Centre
Sexual Health Matters…. Sex, Sexuality, Pleasure, STIs and Public Health Dr David M Lee Honorary Fellow in Sexual Health The University of Melbourne & Ms. Sheranne Dobinson Sexual Health Nurse Melbourne Sexual Health Centre
 Cock: Device marking ‘North’ on the human male compass. The smokestack of the male imagination. A microphone with which one’s friend (s) can broadcast directly to the Interior…Also, unfortunately, a one-lane viral superhighway. [R. Summerbell]
Cock: Device marking ‘North’ on the human male compass. The smokestack of the male imagination. A microphone with which one’s friend (s) can broadcast directly to the Interior…Also, unfortunately, a one-lane viral superhighway. [R. Summerbell]
![Aim of the Session • Public health perspective [Broaden our awareness of diversity ]](https://present5.com/presentation/dc91239604d64efc477963951c555bab/image-3.jpg "Aim of the Session • Public health perspective [Broaden our awareness of diversity ]") Aim of the Session • Public health perspective [Broaden our awareness of diversity ] – Historical past – Psycho-social dimension – Culturally (Baby boomers; Gen X, Y and W) • Provide an insight into the public health control of sexually transmitted infections (STIs) • Update the epidemiological picture of various STIs in Australia and particularly in Victoria
Aim of the Session • Public health perspective [Broaden our awareness of diversity ] – Historical past – Psycho-social dimension – Culturally (Baby boomers; Gen X, Y and W) • Provide an insight into the public health control of sexually transmitted infections (STIs) • Update the epidemiological picture of various STIs in Australia and particularly in Victoria
 WHO Definition of Sexual Health Sexual health is a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination and violence. For sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected and fulfilled. Sexual rights embrace human rights that are already recognized in national laws, international human rights documents and other consensus statements. They include the right of all persons, free of coercion, discrimination and violence, to: • the highest attainable standard of sexual health, including access to sexual and reproductive health care services; seek, receive and impart information related to sexuality; v sexuality education; v respect for bodily integrity; v choose their partner; v decide to be sexually active or not; v consensual sexual relations; v consensual marriage; v decide whether or not, and when, to have children; and v pursue a satisfying, safe and pleasurable sexual life. The responsible exercise of human rights requires that all persons respect the rights of others.
WHO Definition of Sexual Health Sexual health is a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination and violence. For sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected and fulfilled. Sexual rights embrace human rights that are already recognized in national laws, international human rights documents and other consensus statements. They include the right of all persons, free of coercion, discrimination and violence, to: • the highest attainable standard of sexual health, including access to sexual and reproductive health care services; seek, receive and impart information related to sexuality; v sexuality education; v respect for bodily integrity; v choose their partner; v decide to be sexually active or not; v consensual sexual relations; v consensual marriage; v decide whether or not, and when, to have children; and v pursue a satisfying, safe and pleasurable sexual life. The responsible exercise of human rights requires that all persons respect the rights of others.
.") Courtesy: Dr. David Bradford, retired Chief Venereologist (Victoria).
Courtesy: Dr. David Bradford, retired Chief Venereologist (Victoria).
 Courtesy: Prof. Basil Donovan, UNSW / Sydney SHC
Courtesy: Prof. Basil Donovan, UNSW / Sydney SHC
![Common STIs / GTI and BBV in Australia Bacterial Chlamydia trachomatis [O] [N] >>>>>](https://present5.com/presentation/dc91239604d64efc477963951c555bab/image-7.jpg "Common STIs / GTI and BBV in Australia Bacterial Chlamydia trachomatis [O] [N] >>>>>") Common STIs / GTI and BBV in Australia Bacterial Chlamydia trachomatis [O] [N] >>>>> LGV [N] Neisseria gonorrhoea [O] [N] Mycoplasma genitalium Treponema pallidum [O] [N] Non specific urethritis [O] Viral Hepatitis A, [O] [N] B[N] HIV [N]* HPV [O] [S] HSV [O] [S] Protozoa Trichomonasis Non-STI [Genital tract Infections] - Physiological Candida spp (albicans) Bacterial vaginosis Blood Borne Infections [BBV] Hepatitis C [N] [O] Oral transmission possible [S] Skin-to-skin contact [N] Notifiable infection
Common STIs / GTI and BBV in Australia Bacterial Chlamydia trachomatis [O] [N] >>>>> LGV [N] Neisseria gonorrhoea [O] [N] Mycoplasma genitalium Treponema pallidum [O] [N] Non specific urethritis [O] Viral Hepatitis A, [O] [N] B[N] HIV [N]* HPV [O] [S] HSV [O] [S] Protozoa Trichomonasis Non-STI [Genital tract Infections] - Physiological Candida spp (albicans) Bacterial vaginosis Blood Borne Infections [BBV] Hepatitis C [N] [O] Oral transmission possible [S] Skin-to-skin contact [N] Notifiable infection
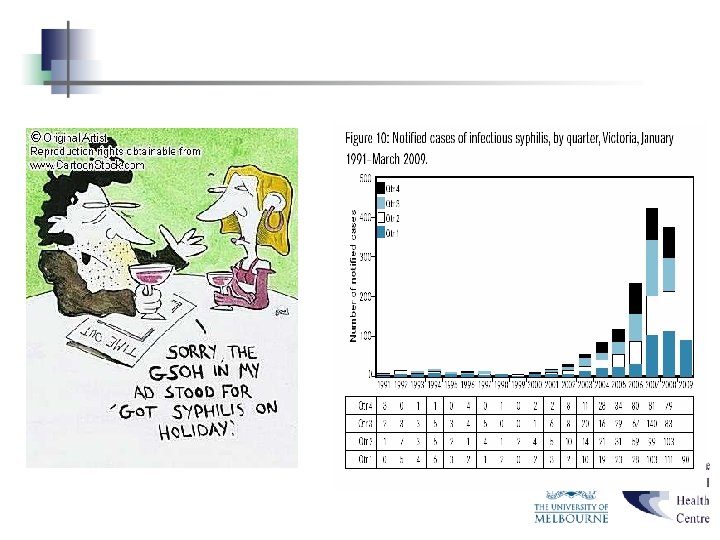
 Important local points *Source: DHS Victoria vidb Jul 2007 • HIV 91% HIV cases diagnosed in men, * 81% of these men-who-have-sex-with-men (MSM)* Decrease in number of diagnoses of AIDS since 94 -95 (HAART) 12 cases heterosexual (1 born high prevalence country; 6 reported sex in high prevalence country; 3 IDU; 2 – locally acquired? )* • Gonorrhoea 80% in MSM, * nearly all amongst MSM; heterosexual – sex overseas* increasing amongst MSM; Issue – antibiotic resistance • Syphilis 300% increase in infectious syphilis* 90% amongst MSM* • Chlamydia 4 fold increase in last decade in Australia mostly impacting young women – :
Important local points *Source: DHS Victoria vidb Jul 2007 • HIV 91% HIV cases diagnosed in men, * 81% of these men-who-have-sex-with-men (MSM)* Decrease in number of diagnoses of AIDS since 94 -95 (HAART) 12 cases heterosexual (1 born high prevalence country; 6 reported sex in high prevalence country; 3 IDU; 2 – locally acquired? )* • Gonorrhoea 80% in MSM, * nearly all amongst MSM; heterosexual – sex overseas* increasing amongst MSM; Issue – antibiotic resistance • Syphilis 300% increase in infectious syphilis* 90% amongst MSM* • Chlamydia 4 fold increase in last decade in Australia mostly impacting young women – :
 Snapshot of Sex and Relationships Figure 1. 9 Population and diagrammatic representation of the core group concept Non core Group – Fewer partners; more sex acts per partner [Serial Monogamy] Bridge Group Core Group – More partners; less sex acts per partner. [Concurrent partnerships]
Snapshot of Sex and Relationships Figure 1. 9 Population and diagrammatic representation of the core group concept Non core Group – Fewer partners; more sex acts per partner [Serial Monogamy] Bridge Group Core Group – More partners; less sex acts per partner. [Concurrent partnerships]
![How do you control STIs? R 0[t] = βc. D(χ) R 0 Reproductive Rate](https://present5.com/presentation/dc91239604d64efc477963951c555bab/image-10.jpg "How do you control STIs? R 0[t] = βc. D(χ) R 0 Reproductive Rate") How do you control STIs? R 0[t] = βc. D(χ) R 0 Reproductive Rate [t]=time β Transmission probability per partnership C Rate of partner change D Duration of Infection
How do you control STIs? R 0[t] = βc. D(χ) R 0 Reproductive Rate [t]=time β Transmission probability per partnership C Rate of partner change D Duration of Infection
 Commonwealth Department of Health and Aged Care National Sexually Transmissible Infections Strategy 2005 – 2008 Priority Areas • Chlamydia Control and Prevention • STIs in gay and other homosexually active men • STIs in Aboriginal and Torres Straits Islanders http: //www. health. gov. au/internet/wcms/publishing. nsf/Content/phd-sti-strategy-cnt. htm/$FILE/sti_strategy. pdf
Commonwealth Department of Health and Aged Care National Sexually Transmissible Infections Strategy 2005 – 2008 Priority Areas • Chlamydia Control and Prevention • STIs in gay and other homosexually active men • STIs in Aboriginal and Torres Straits Islanders http: //www. health. gov. au/internet/wcms/publishing. nsf/Content/phd-sti-strategy-cnt. htm/$FILE/sti_strategy. pdf
 Epidemiology: Chlamydia trachomatis Source: DHS Victoria www. dhs. vic. gov. au/ideas
Epidemiology: Chlamydia trachomatis Source: DHS Victoria www. dhs. vic. gov. au/ideas
 Priority Group: Gay or other homosexually active men R 0 = βc. D β– Good degree condoms use; co-infection with another STI c – high rate of partner change D – access to screening n n n Male sexuality – sex drive etc. Heterosexism Homophobia
Priority Group: Gay or other homosexually active men R 0 = βc. D β– Good degree condoms use; co-infection with another STI c – high rate of partner change D – access to screening n n n Male sexuality – sex drive etc. Heterosexism Homophobia
 and condom use (β) Heterosexual") MSM attending MSHC 2005– Rate of Partner Change (c) and condom use (β) Heterosexual men MSM Rate of Partner Change 3 mths Mean 1. 7 Mean 5. 3 100% Condom use past 12 months 18 % 51 % (20% no anal sex at all)
MSM attending MSHC 2005– Rate of Partner Change (c) and condom use (β) Heterosexual men MSM Rate of Partner Change 3 mths Mean 1. 7 Mean 5. 3 100% Condom use past 12 months 18 % 51 % (20% no anal sex at all)
 Gonorrhoea: Symptoms / Signs / Tests / Treatment /Sequelae / Follow Up
Gonorrhoea: Symptoms / Signs / Tests / Treatment /Sequelae / Follow Up
 HIV Victorian Prevalence § Calculation of possible HIV transmission if source is unknown is based on prevalence in local population: § § Homosexual men: 3 -15% Injecting Drug Users: 1% If IDU and gay: 17% Heterosexuals blood donors: 0. 0005%, STI clinic attendees 0. 1%
HIV Victorian Prevalence § Calculation of possible HIV transmission if source is unknown is based on prevalence in local population: § § Homosexual men: 3 -15% Injecting Drug Users: 1% If IDU and gay: 17% Heterosexuals blood donors: 0. 0005%, STI clinic attendees 0. 1%
 Sexual transmission probability Anderson, RM Sex Transm Disases 1999, pg 26 Transmission probability (per partnership, no account of type, frequency) Mean duration Transmission of infection if by oral sex untreated in years Salient points Gonorrhoea 0. 5 yes Antimicrobial resistance chlamydia 0. 2 1. 0 yes In women, long term complications Syphilis 0. 6 1. 0 yes In women, long term complications HIV 0. 05 - 0. 15 8 - 12 No (very low risk) AIDS *Presence of any STI ↑ risk of acquiring and transmitting HIV
Sexual transmission probability Anderson, RM Sex Transm Disases 1999, pg 26 Transmission probability (per partnership, no account of type, frequency) Mean duration Transmission of infection if by oral sex untreated in years Salient points Gonorrhoea 0. 5 yes Antimicrobial resistance chlamydia 0. 2 1. 0 yes In women, long term complications Syphilis 0. 6 1. 0 yes In women, long term complications HIV 0. 05 - 0. 15 8 - 12 No (very low risk) AIDS *Presence of any STI ↑ risk of acquiring and transmitting HIV
 STI / HIV Prevention • • • condoms for vaginal, anal and oral sex non-penetrative contact partner notification and treatment raised awareness and education about STI’s regular screening and treatment with antibiotics if detected • early detection may prevent complications and transmission of the STI to other sexual partners • regular screening encouraged amongst MSM
STI / HIV Prevention • • • condoms for vaginal, anal and oral sex non-penetrative contact partner notification and treatment raised awareness and education about STI’s regular screening and treatment with antibiotics if detected • early detection may prevent complications and transmission of the STI to other sexual partners • regular screening encouraged amongst MSM
 Other Viral STIs ? Importance Hepatitis A - oral to feacal transmission Hepatitis B - blood, semen, vaginal fluids, breastmilk HCV = BBV – > Not classified as STI HSV (Skin-to-skin) HPV (Skin-to-skin)
Other Viral STIs ? Importance Hepatitis A - oral to feacal transmission Hepatitis B - blood, semen, vaginal fluids, breastmilk HCV = BBV – > Not classified as STI HSV (Skin-to-skin) HPV (Skin-to-skin)
 Interactive Session • Scenario 1 – You have had 3 days of a urethral discharge associated with a dysuria. You present to your local SHC and the diagnosis of gonorrhoea is made and you are treated. You are advised to bring your partner in for testing and treatment. – What goes through your mind?
Interactive Session • Scenario 1 – You have had 3 days of a urethral discharge associated with a dysuria. You present to your local SHC and the diagnosis of gonorrhoea is made and you are treated. You are advised to bring your partner in for testing and treatment. – What goes through your mind?
 Interactive Session 2 • Scenario 2 – Your partner tells you in a ‘round about way’ that he needs you to attend your GP for treatment of gonorrhoea. You have been together for 5 years and you ‘know’ that the relationship is ‘monogamous’ but you have never really had to talk about the ‘boundaries’. – When you see your GP, she tells you that you have a noticeable discharge O/E (mucopurulent pus) despite remaining asymptomatic. She also states that there is a ‘gonorrhoea’ rise but in Melbourne but it is mainly in men who have sex with other men. – What goes through your mind?
Interactive Session 2 • Scenario 2 – Your partner tells you in a ‘round about way’ that he needs you to attend your GP for treatment of gonorrhoea. You have been together for 5 years and you ‘know’ that the relationship is ‘monogamous’ but you have never really had to talk about the ‘boundaries’. – When you see your GP, she tells you that you have a noticeable discharge O/E (mucopurulent pus) despite remaining asymptomatic. She also states that there is a ‘gonorrhoea’ rise but in Melbourne but it is mainly in men who have sex with other men. – What goes through your mind?

 MSHC Resources and Supports www. mshc. org. au • Web-based Patient Information ‘Check Your Risk’ http: //checkyourrisk. org. au/ • Web-based GP resources www. mshc. org. au/gpassist • Sexual Health Physician Advice Line: 1800 009 903 (Toll Free) Hours available: Monday - Friday 09. 00 12. 30 and 13. 30 - 17. 00
MSHC Resources and Supports www. mshc. org. au • Web-based Patient Information ‘Check Your Risk’ http: //checkyourrisk. org. au/ • Web-based GP resources www. mshc. org. au/gpassist • Sexual Health Physician Advice Line: 1800 009 903 (Toll Free) Hours available: Monday - Friday 09. 00 12. 30 and 13. 30 - 17. 00
 Outreach • Rh. ED-Researching Health and Education in the Sex Industry – Shop-front clinic – Mobile clinic • SOPV – Men-only sex venues, MSM, gay – Privately owned business/club – Clinics – male nurses only • Prisons • Web site – www. mshc. org. au
Outreach • Rh. ED-Researching Health and Education in the Sex Industry – Shop-front clinic – Mobile clinic • SOPV – Men-only sex venues, MSM, gay – Privately owned business/club – Clinics – male nurses only • Prisons • Web site – www. mshc. org. au
 • • • On") Resources and Supports MSHC Services – WITS (Walk-In Triage Service) • • • On site clinical services General Clinic Green Room Special Clinics (Thai, Korean, Chinese Sex Workers; Vulval, Dermatology Clinic) – and MSM Clinics (Thursday Evening) Results and Information Line (9341 6200 and follow prompts) Outreach Sex-On Premises Venue Street based Sex workers (Rh. ED) VACCHO and CALD Projects Prisons Project Partner Notification Officers (DHS) – Ph: 9347 1899
Resources and Supports MSHC Services – WITS (Walk-In Triage Service) • • • On site clinical services General Clinic Green Room Special Clinics (Thai, Korean, Chinese Sex Workers; Vulval, Dermatology Clinic) – and MSM Clinics (Thursday Evening) Results and Information Line (9341 6200 and follow prompts) Outreach Sex-On Premises Venue Street based Sex workers (Rh. ED) VACCHO and CALD Projects Prisons Project Partner Notification Officers (DHS) – Ph: 9347 1899