

1077f7c64358cd58e482340e68ed8f6f.ppt
- Количество слайдов: 22
 Sensory causes of diplopia. Aniseikonia LIONEL KOWAL RVEEH MELBOURNE Financial involvement: Patients paid their bills
Sensory causes of diplopia. Aniseikonia LIONEL KOWAL RVEEH MELBOURNE Financial involvement: Patients paid their bills
 Diplopia 2 images, one seen by each eye, are separated and the patient’s motor and sensory fusion are inadequate to bring them together n Usually only consider the motor aspect of separation Motor fusion impaired by sensory problems - the 2 images need to be fairly similar to be fused: n Aniseikonia - difference in image size - will prevent fusion n n Metamorphopsia Field defect n Often treatable with glasses n
Diplopia 2 images, one seen by each eye, are separated and the patient’s motor and sensory fusion are inadequate to bring them together n Usually only consider the motor aspect of separation Motor fusion impaired by sensory problems - the 2 images need to be fairly similar to be fused: n Aniseikonia - difference in image size - will prevent fusion n n Metamorphopsia Field defect n Often treatable with glasses n
 You miss more by not asking than by not knowing …. . after John Colvin ASK EVERY PATIENT WHOSE DIPLOPIA IS NOT EASILY COMPENSATED FOR WITH PRISM: Is the image seen by the R n Larger / smaller than the L n The same shape as L n Paler / darker than L n Tilted [not aniseikonia: torsion]
You miss more by not asking than by not knowing …. . after John Colvin ASK EVERY PATIENT WHOSE DIPLOPIA IS NOT EASILY COMPENSATED FOR WITH PRISM: Is the image seen by the R n Larger / smaller than the L n The same shape as L n Paler / darker than L n Tilted [not aniseikonia: torsion]
 Materials and methods n Retrospective chart study n 11 patients n Aged 29 -86 n M: F 8: 3
Materials and methods n Retrospective chart study n 11 patients n Aged 29 -86 n M: F 8: 3
 Results n=11 n 10 vision 6/8 or better in the worse eye n 10 complained of diplopia n 1 had wobbling of words
Results n=11 n 10 vision 6/8 or better in the worse eye n 10 complained of diplopia n 1 had wobbling of words
 Results n=11 n Anisometropia in 7 n Macular causes in 4 2/4 had ERM on macula NO ERM SURGERY 1/4 had previous ERM peel with residual or recurrent ERM temporal to macula 1/4 had macular hole surgery & anisometropia RESPONDED TO GLASSES FOR ANISOMETROPIA
Results n=11 n Anisometropia in 7 n Macular causes in 4 2/4 had ERM on macula NO ERM SURGERY 1/4 had previous ERM peel with residual or recurrent ERM temporal to macula 1/4 had macular hole surgery & anisometropia RESPONDED TO GLASSES FOR ANISOMETROPIA
 Measuring aniseikonia n The least amount of aniseikonia causing disruption of fusion was 2% n Largest amount of aniseikonia was 20 % which was corrected with telescopic lenses (+CLs with equal – in glasses) Other techniques: Synoptophore Free space techniques
Measuring aniseikonia n The least amount of aniseikonia causing disruption of fusion was 2% n Largest amount of aniseikonia was 20 % which was corrected with telescopic lenses (+CLs with equal – in glasses) Other techniques: Synoptophore Free space techniques
 AWAYA’S NEW ANISEIKONIA TEST Use R-G glasses. Find the pair of semicircles where the difference in size compensates for the patient’s aniseikonia
AWAYA’S NEW ANISEIKONIA TEST Use R-G glasses. Find the pair of semicircles where the difference in size compensates for the patient’s aniseikonia
 Measuring aniseikonia Free space estimation Separate with prism. Which eye sees the bigger / smaller image? n If each bar of the E is ~20%, how much bigger / smaller is the image seen by L? R? n Check with prism in front of other eye - prisms can cause magnification CONFOUNDER: MEASUREMENT ARTEFACT - each technique can give a VERY different answer
Measuring aniseikonia Free space estimation Separate with prism. Which eye sees the bigger / smaller image? n If each bar of the E is ~20%, how much bigger / smaller is the image seen by L? R? n Check with prism in front of other eye - prisms can cause magnification CONFOUNDER: MEASUREMENT ARTEFACT - each technique can give a VERY different answer
 Ask pt to look @ both 6/60 ‘E’. RE sees the higher image. Which one is bigger? Does it look like an ‘E’ should? Are all parts of it bigger [m’morphopsia]? Is the ‘E’ Tilted? If a bar of the ‘E’ is worth 20%, how much bigger is it? Also check with BD prism in front of other eye - prisms can also cause magnification
Ask pt to look @ both 6/60 ‘E’. RE sees the higher image. Which one is bigger? Does it look like an ‘E’ should? Are all parts of it bigger [m’morphopsia]? Is the ‘E’ Tilted? If a bar of the ‘E’ is worth 20%, how much bigger is it? Also check with BD prism in front of other eye - prisms can also cause magnification
 Results n=11 n 7 /11 had vertical deviation ? vertical fusion is more fragile than horizontal n 3 /7 also had horizontal deviations n 2 had exophoria with poor FR
Results n=11 n 7 /11 had vertical deviation ? vertical fusion is more fragile than horizontal n 3 /7 also had horizontal deviations n 2 had exophoria with poor FR
 Results n=11 n 5 modified spectacles + prisms n 1 contact lenses n 1 reduced prescription of near add on one lens
Results n=11 n 5 modified spectacles + prisms n 1 contact lenses n 1 reduced prescription of near add on one lens
 FOR") Results n=11 n 1 had telescopic lenses (+ve CL and –ve spectacle lens) FOR 20% ANISEIKONIA n 2 had surgery for exotropia n 1 declined treatment
Results n=11 n 1 had telescopic lenses (+ve CL and –ve spectacle lens) FOR 20% ANISEIKONIA n 2 had surgery for exotropia n 1 declined treatment
 Results In most patients, aniseikonia precipitates small angle strabismus due to loss of sensory fusion wch in turn impairs motor fusion n Compensation for the strabismus with prisms along with lenses modified to compensate for the aniseikonia worked in 5/7 optically corrected patients n
Results In most patients, aniseikonia precipitates small angle strabismus due to loss of sensory fusion wch in turn impairs motor fusion n Compensation for the strabismus with prisms along with lenses modified to compensate for the aniseikonia worked in 5/7 optically corrected patients n
 Discussion n Two main clinical causes of Aniseikonia n Macular causes Anisometropia ~ 1% of aniseikonia per DS of anisometropia n
Discussion n Two main clinical causes of Aniseikonia n Macular causes Anisometropia ~ 1% of aniseikonia per DS of anisometropia n
 A Prospective Study of Binocular Visual Function before and after Successful Surgery to Remove a Unilateral Epiretinal Membrane Ophthalmology November 2008 n n n 2/27: diplopia Measured stereo, motor fusion & VA. Stereo & total motor fusion ranges reduced After successful surgery, stereo function, VA & motor fusion improved mainly in those with shorter duration of symptoms [esp < 18 mo] Stereo function improved mainly in those with better preoperative stereo
A Prospective Study of Binocular Visual Function before and after Successful Surgery to Remove a Unilateral Epiretinal Membrane Ophthalmology November 2008 n n n 2/27: diplopia Measured stereo, motor fusion & VA. Stereo & total motor fusion ranges reduced After successful surgery, stereo function, VA & motor fusion improved mainly in those with shorter duration of symptoms [esp < 18 mo] Stereo function improved mainly in those with better preoperative stereo
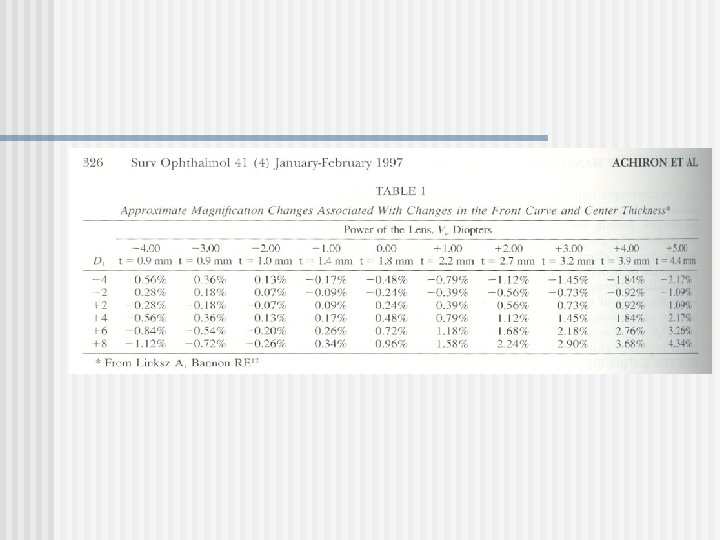
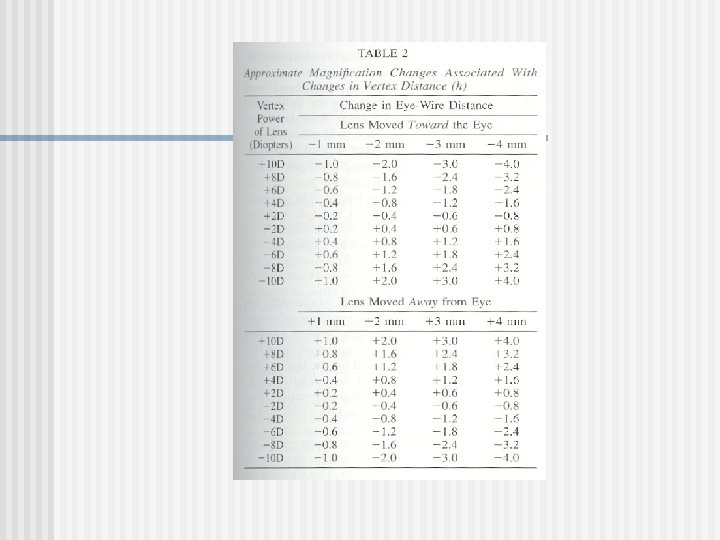
 Optical solutions to increase image size n n Increase front base curve Increase central thickness Decreased vertex distance increases image size in – lens [and decreases in +] increase refractive index …. often successful NOT known to average optometrist / dispenser
Optical solutions to increase image size n n Increase front base curve Increase central thickness Decreased vertex distance increases image size in – lens [and decreases in +] increase refractive index …. often successful NOT known to average optometrist / dispenser
 Aniseikonia as a substantial factor in causing diplopia n n n Probably rare Always unrecognised by referring doctor or optom Need to ask about it - pt always knows but needs to be asked the right Q Often fixable with prisms and aniseikonic modifications THANK YOU
Aniseikonia as a substantial factor in causing diplopia n n n Probably rare Always unrecognised by referring doctor or optom Need to ask about it - pt always knows but needs to be asked the right Q Often fixable with prisms and aniseikonic modifications THANK YOU
 Discussion
Discussion