
SEMEY STATE MEDICAL UNIVERSITY DEPARTMENT OF RUSSIAN AND






ang_siw_kanapin_210_gmf.ppt
- Размер: 1.9 Мб
- Автор:
- Количество слайдов: 30
Описание презентации SEMEY STATE MEDICAL UNIVERSITY DEPARTMENT OF RUSSIAN AND по слайдам
SEMEY STATE MEDICAL UNIVERSITY DEPARTMENT OF RUSSIAN AND FOREIGN LANGUAGE The theme: Child diseases. Pneumonia in infants. Checked by: Mukhametzhanova Z. A. Prepared by : Kanapin D. K 210 group GMFSIW SEMEY
PLAN: 1. Discuss the common causes of pneumonia in children of various ages; 2. Classifications of pneumonia in children; 3. Clinical manifestations of pneumonia in children; 4. Outline the approach to the diagnosis of pneumonia in children; 5. Select appropriate antibiotic therapy for a child with pneumonia based on child’s age and severity of illness; 6. Discuss the diagnosis and management of common complications of pneumonia
Pneumonia in pediatric patients Basic facts Childhood pneumonia remains an important cause of morbidity and mortality in developing world – 4 million deaths annually in the developing world; About 20% of all deaths in children under 5 ys are due to Acute Lower Respiratory Infections (ALRIs — pneumonia, bronchiolitis and bronchitis); 90% of these deaths are due to pneumonia. Annual incidence in the U. S. in: Children under 5 yo is ~ 40 cases/1000 Children age 12 -15 ~ 7 cases/1000 Mortality rate < 1/1. 000 in the U. S.
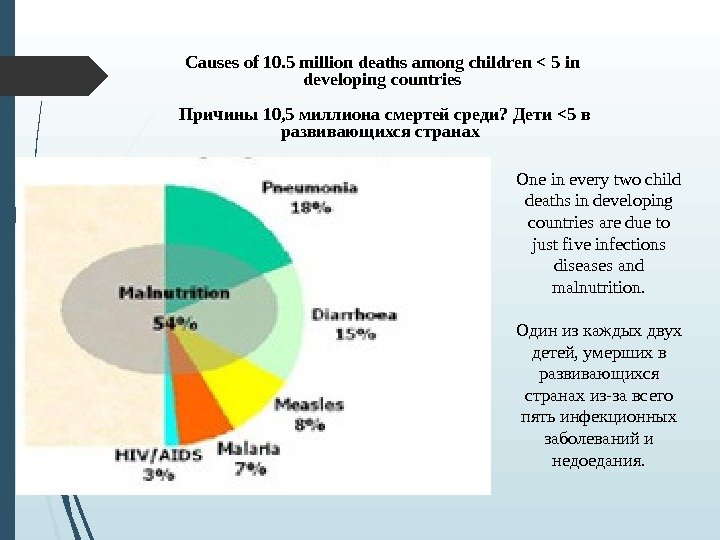
Causes of 10. 5 million deaths among children < 5 in developing countries Причины 10, 5 миллиона смертей среди? Дети <5 в развивающихся странах One in every two child deaths in developing countries are due to just five infections diseases and malnutrition. Один из каждых двух детей, умерших в развивающихся странах из-за всего пять инфекционных заболеваний и недоедания.
Pneumonia in pediatric patients Early recognition and prompt treatment of pneumonia is life saving. Low birth weight, malnourished and non-breastfed children and those living in overcrowded conditions are at higher risk of getting pneumonia. These children are also at a higher risk of death from pneumonia. About one-half of all children < 5 yo with community-acquired pneumonia will require hospitalization;
Pneumonia Is an acute infectious inflammatory disease of various nature with involving of lower respiratory tract into pathologic process and intra-alveolar inflammatory exudation; Э то острое инфекционное воспалительное заболевание различной природы с участием нижних отделов дыхательных путей в патологический процесс и внутри альвеол воспалительной экссудации;
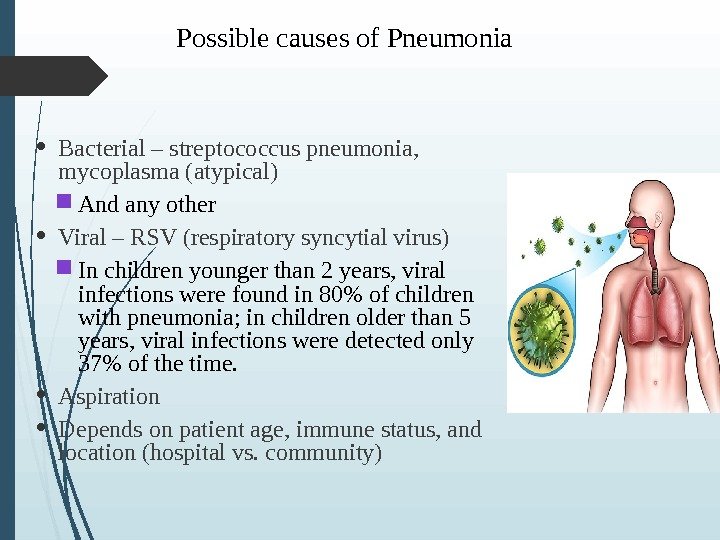
Possible causes of Pneumonia Bacterial – streptococcus pneumonia, mycoplasma (atypical) And any other Viral – RSV (respiratory syncytial virus) In children younger than 2 years, viral infections were found in 80% of children with pneumonia; in children older than 5 years, viral infections were detected only 37% of the time. Aspiration Depends on patient age, immune status, and location (hospital vs. community)
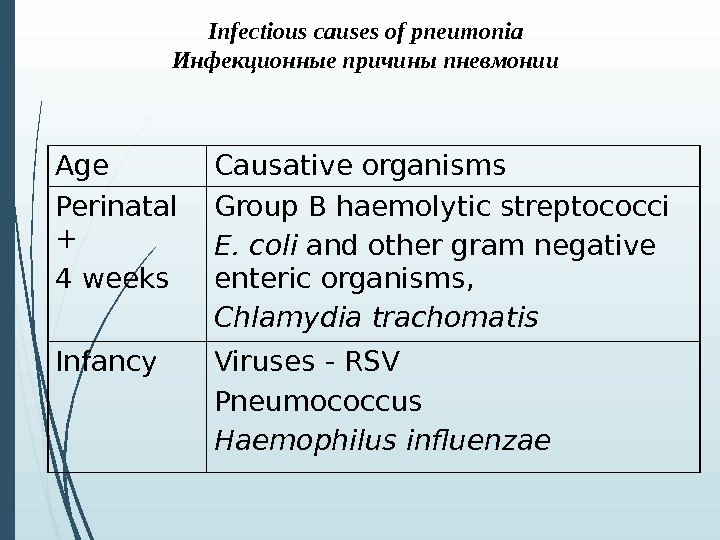
Infectious causes of pneumonia Инфекционные причины пневмонии Age Causative organisms Perinatal + 4 weeks Group B haemolytic streptococci E. coli and other gram negati ve enteric organisms , Chlamydia trachomatis Infancy Viruses — RSV Pneumococcus Haemophilus influenzae
Pathophysiology Often, follows upper respiratory tract infection; Lower respiratory tract invaded by bacteria, viruses or other pathogens; Preceding viral illness (influenza, parainfluenza, RSV, adenovirus) leads to increased incidence of pneumococcal pneumonia; Bacterial pneumonias usually due to spread of invasive organisms from the nasopharynx by inhalation or aspiration; In children, bacteremia may lead to hematogenous seeding of the pulmonary parenchyma and result in pneumonia
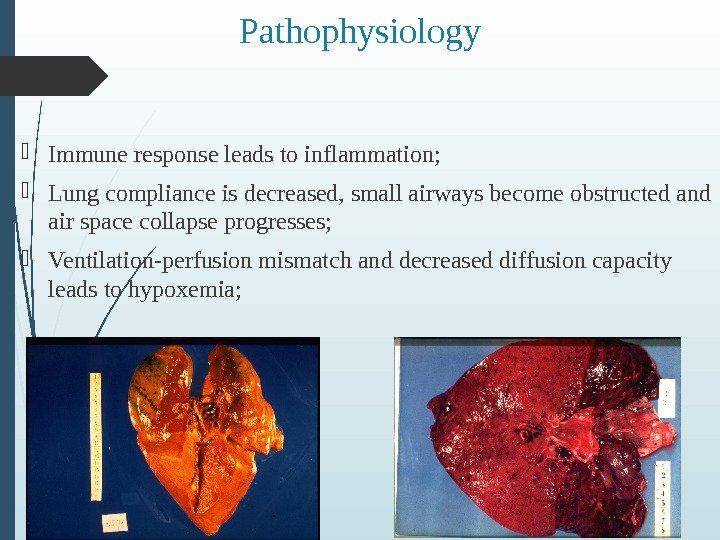
Pathophysiology Immune response leads to inflammation; Lung compliance is decreased, small airways become obstructed and air space collapse progresses; Ventilation-perfusion mismatch and decreased diffusion capacity leads to hypoxemia;
CLASSIFICATION: E tiology Morp h ological class — Bronchopneumonia — L obar pneumonia — Interstitial pneumonia — C o ngenital pneumonia — Community acquired pneumonia -N osocomial ( hospital acquired) pneumonia -Aspiration pneumonia -N on complicated pneumonia — C omplicated pneumonia
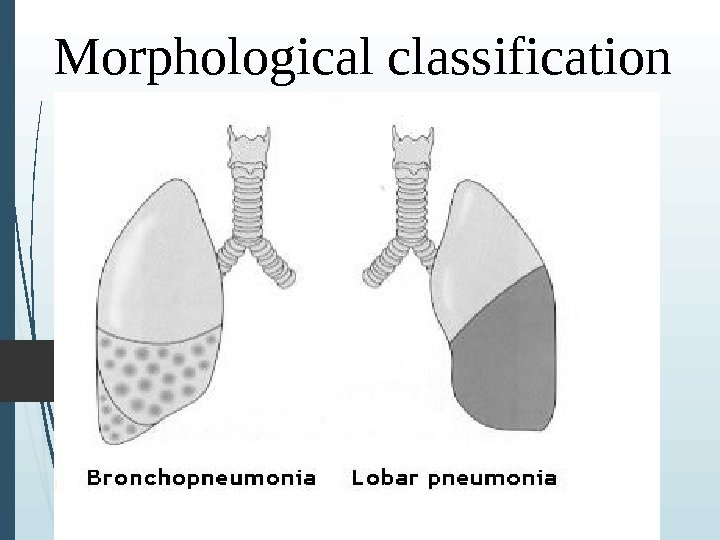
M orp h ological class ification
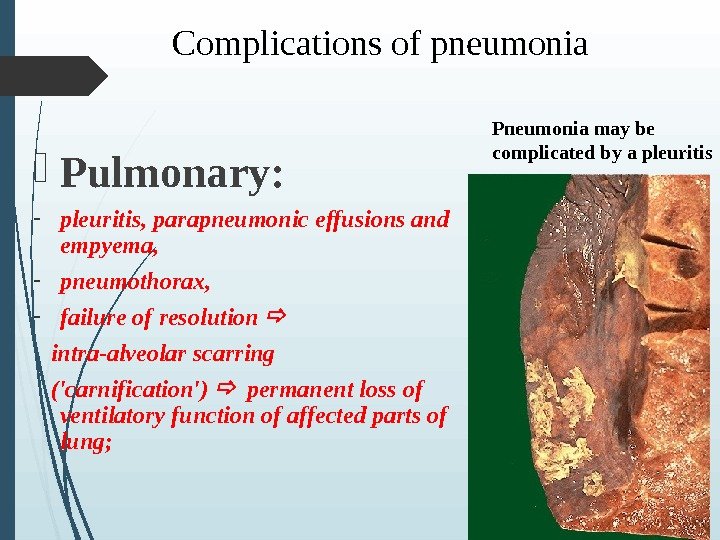
Complications of pneumonia Pulmonary: — pleuritis, parapneumonic effusions and empyema, — pneumothorax, — f ailure of resolution intra-alveolar scarring (‘carnification’) permanent loss of ventilatory function of affected parts of lung ; Pneumonia may be complicated by a pleuritis
Complications of pneumonia Extrapulmonary: — i nfective endocarditis — c erebral abscess / meningitis — s eptic arthritis — Infectious-toxic shock — DIC (disseminated intravascular coagulation) syndrome
Significant risk factors younger age (2 -6 months), low parental education, smoking at home, prematurity, weaning from breast milk at < 6 months, anaemia malnutrition Trop Doct 2001 Jul; 31(3): 139 —
Clinical case 1 2 y old boy with complaints of fever, cough, vomiting, decreased appetite, chest pain, right lower quadrant (RLQ) abdominal pain; T 39 C, chills, HR 140, RR 50; Retractions, signs of respiratory distress; Decreased breath sounds, rales, egophony, dullness to percussion rate; Symptoms since yesterday afternoon; Recent upper respiratory infection;
Clinical case 1 Physical examination Tachypnea Fever (T 39 C) – nonspecific and not 100% sensitive sign; Hypoxemia (pulse oximetry – 5 th vital sign) Signs of respiratory distress (retractions, flaring, grunting) X-ray: infiltrates of lung tissue
Clinical case 1 Physical examination Wheezing is rare with bacterial pneumonia – more common in pneumonia caused by atypical bacterial or viruses less than 5% of children with wheezing had pneumonia; only 2% of children without fever in the ED had pneumonia; hypoxemia (Sp. O 2 < 92 %) increased risk;
Atypical Pneumonia Chlamydia – – Diffuse intersitial markings – hyperinflation Mycoplasma – – Normal, or can look like viral or typical bacterial PNA CXR in:
Symptoms-pleuritic Referred pain to neck and back Abdominal pain if diaphragmatic involvement
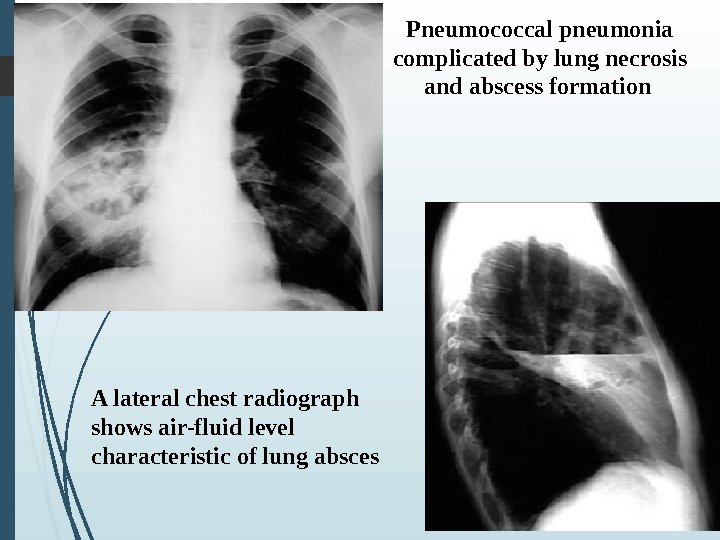
Pneumococcal pneumonia complicated by lung necrosis and abscess formation A lateral chest radiograph shows air-fluid level characteristic of lung absces
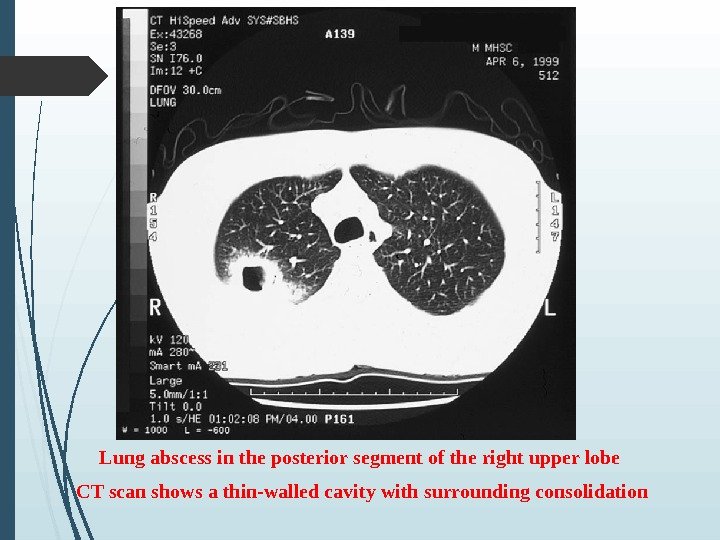
Lung abscess in the posterior segment of the right upper lobe CT scan shows a thin-walled cavity with surrounding consolidation
Disposition Admit if: Toxic appearance; Respiratory compromise, including marked tachypnea (>60 breaths/min in infant and > 40 -50 breaths/min in older children); Hypoxemia (Sp. O 2 < 92 -94% in room air); Dehydration or inability to maintain oral hydration or tolerate oral medications; Indications of severe disease;
Disposition Admit if: Young age — < 4 -6 months of age; Underlying diseases: — cardiac disease — renal disease — hematological disease Inability of family to provide care at home; Failure of outpatient therapy;
Antibiotic therapy I – beta-lactam : — Penicillin ; — Cephalosporin ; — Carbopenem ; Aminoglycoside Macrolide Linkozamide – linkomycin, clindomycin Vancomycin
Treatment • Bacterial 1 month Ampicillin 75– 100 mg/kg/day and Gentamicin 5 mg/kg d 1– 3 months Cefuroxime (75– 150 mg/kg/day) or co-amoxiclav (40 mg/kg/day) 3 months Benzylpenicillin or erythromycin (change to cefuroxime or amoxycillin if no response)
Treatment Supportive for atypical pneumonia • Chlamydia and mycoplasma should be treated with erythromycin 40– 50 mg/kg/day usually orally. • If pneumocystis carinii pneumonia is suspected co-trimoxazole 18– 27 mg/kg/day IV should be prescribed.
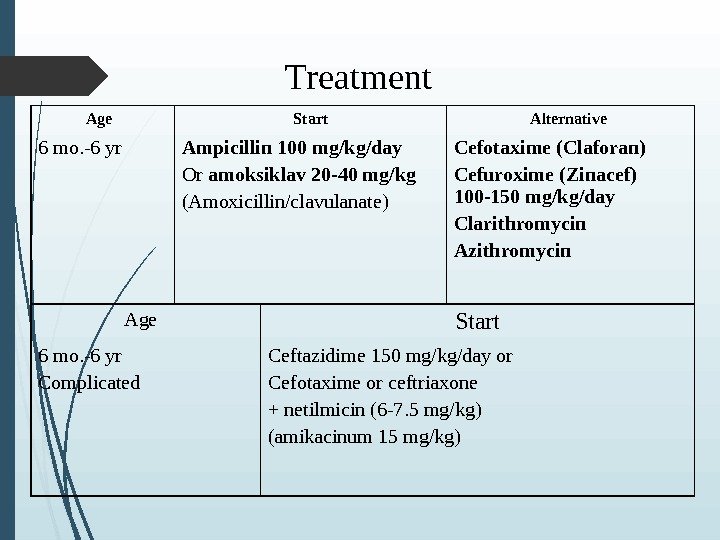
Treatment Age Start Alternative 6 mo. -6 yr Ampicillin 100 mg/kg/day Or amoksiklav 20 -40 mg/kg (Amoxicillin/clavulanate) Cefotaxime (Claforan) Cefuroxime (Zinacef) 100 -150 mg/kg/day Clarithromycin Azithromycin Age Start 6 mo. -6 yr Complicated Ceftazidime 150 mg/kg/day or Cefotaxime or ceftriaxone + netilmicin (6 -7. 5 mg/kg) ( amikacinum 15 mg/kg)
Literature: 1. A. M. Maslova, Z. I. Winestein, L. S. Plebeyskaya “ Essential English for medical students” 2003 2. www. yandex. ru 3. www. google. kz
THANKS FOR YOUR ATTENTION!