

2d0af35365cbd623844266f22a943179.ppt
- Количество слайдов: 59
 Risk Assessment and Risk Management of Emerging and Re-emerging Infectious Diseases: Public Health / Risk Assessors Perspective Susie El. Saadany, Chief, Statistics and Risk Assessment & Adjunct Professor, Faculty of Medicine, University of Ottawa Blood Safety Surveillance and Health Care Acquired Infections Division Centre for Communicable Diseases and Infection Control Infectious Diseases and Emergency Preparedness Branch Public Health Agency of Canada Mathematics in Emerging Infectious Disease Management, Cuernavaca, Mexico, January 10 -14, 2011
Risk Assessment and Risk Management of Emerging and Re-emerging Infectious Diseases: Public Health / Risk Assessors Perspective Susie El. Saadany, Chief, Statistics and Risk Assessment & Adjunct Professor, Faculty of Medicine, University of Ottawa Blood Safety Surveillance and Health Care Acquired Infections Division Centre for Communicable Diseases and Infection Control Infectious Diseases and Emergency Preparedness Branch Public Health Agency of Canada Mathematics in Emerging Infectious Disease Management, Cuernavaca, Mexico, January 10 -14, 2011
 Outline • Background Blood Safety Programme at The Public Health Agency of Canada • Challenges and Responsibility • Risk Assessment Tools • Expert Elicitation (as an Informative Process) • Examples
Outline • Background Blood Safety Programme at The Public Health Agency of Canada • Challenges and Responsibility • Risk Assessment Tools • Expert Elicitation (as an Informative Process) • Examples
 The Blood Safety Program
The Blood Safety Program
 Parenteral Transmission Nosocomial Transmission (Bloodborne Pathogens) SEPSIS Nosocomial jurisdiction, if") Healthcare Associated Infections (HAI) Parenteral Transmission Nosocomial Transmission (Bloodborne Pathogens) SEPSIS Nosocomial jurisdiction, if microbes cultured and/or identified. If no microbes can be cultured or identified, then the case becomes Bloodborne Pathogen’s jurisdiction, usually related to an unknown virus. [The syringe issue related to a nosocomial transmission of bloodborne pathogens (BBP) by reuse of a single syringe. This requires a BBP risk assessment along with nosocomial and BBP risk mitigation strategies. ]
Healthcare Associated Infections (HAI) Parenteral Transmission Nosocomial Transmission (Bloodborne Pathogens) SEPSIS Nosocomial jurisdiction, if microbes cultured and/or identified. If no microbes can be cultured or identified, then the case becomes Bloodborne Pathogen’s jurisdiction, usually related to an unknown virus. [The syringe issue related to a nosocomial transmission of bloodborne pathogens (BBP) by reuse of a single syringe. This requires a BBP risk assessment along with nosocomial and BBP risk mitigation strategies. ]
 Sources of Emerging Pathogens Transmitted via Blood Clotting Factors Platelets Cryoprecipitate Fresh/Frozen Plasma Emerging Blood Pathogens Cells, tissues, organs, semen Zoonotic, parasitic, viral, bacterial and prion infections Correctional Facilities Community Prevalence Xenotransplantation Immigration and population movement Climate change and vector movement
Sources of Emerging Pathogens Transmitted via Blood Clotting Factors Platelets Cryoprecipitate Fresh/Frozen Plasma Emerging Blood Pathogens Cells, tissues, organs, semen Zoonotic, parasitic, viral, bacterial and prion infections Correctional Facilities Community Prevalence Xenotransplantation Immigration and population movement Climate change and vector movement
 Sources of Emerging Pathogens Transmitted Parenterally via Healthcare Blood, Components & Products Cells, Tissues, Organs & Semen Surgical Implants of Animal Tissues Medical Devices Healthcare Associated Infections (HAI) (TPD) Biologics Emerging Technologies Surveillance initiated and/or under development: high risk (includes vaccines) (BGTD) Grandfathered-in Biologics* Surveillance not yet initiated: high risk & significant gaps * eg. , heparins TPD: Therapeutic Products Directorate, Health Canada BGTD: Biologics and Genetic Therapies Directorate, Health Canada Considered low risk except for CJD/v. CJD and other prion diseases
Sources of Emerging Pathogens Transmitted Parenterally via Healthcare Blood, Components & Products Cells, Tissues, Organs & Semen Surgical Implants of Animal Tissues Medical Devices Healthcare Associated Infections (HAI) (TPD) Biologics Emerging Technologies Surveillance initiated and/or under development: high risk (includes vaccines) (BGTD) Grandfathered-in Biologics* Surveillance not yet initiated: high risk & significant gaps * eg. , heparins TPD: Therapeutic Products Directorate, Health Canada BGTD: Biologics and Genetic Therapies Directorate, Health Canada Considered low risk except for CJD/v. CJD and other prion diseases
 within Blood") SRA Section Roles and Responsibilities • Statistics and Risk Assessment Section (SRA) within Blood Safety Surveillance and Health Care Acquired Infections Division: – Special focus on risk assessments for rare and emerging diseases to meet modern health care needs for better knowledge in the face of little to no scientific information – Promoting the development of statistical techniques surrounding issues of modeling uncertainty. – Facilitating iterative communication between regulators (Health Canada, Biologics and Genetic Therapies Directorate) and policy makers
SRA Section Roles and Responsibilities • Statistics and Risk Assessment Section (SRA) within Blood Safety Surveillance and Health Care Acquired Infections Division: – Special focus on risk assessments for rare and emerging diseases to meet modern health care needs for better knowledge in the face of little to no scientific information – Promoting the development of statistical techniques surrounding issues of modeling uncertainty. – Facilitating iterative communication between regulators (Health Canada, Biologics and Genetic Therapies Directorate) and policy makers
 Data Limitations for Rare and Emerging Diseases Scientific information required to model the public health risks for rare and emerging diseases and events may be limited or unavailable due to: • • • poor understanding of the disease / event limited case numbers lack of scientific study lack of valid information in the bio-medical literature obstacles in communicating what information is known These limitations need to be managed against urgent needs for risk assessment and regulatory policy development to mitigate public health risks.
Data Limitations for Rare and Emerging Diseases Scientific information required to model the public health risks for rare and emerging diseases and events may be limited or unavailable due to: • • • poor understanding of the disease / event limited case numbers lack of scientific study lack of valid information in the bio-medical literature obstacles in communicating what information is known These limitations need to be managed against urgent needs for risk assessment and regulatory policy development to mitigate public health risks.
 SRA Experience • Have encountered 3 types of “insufficient data” 1. 2. 3. • Data do not exist Data cannot be published (proprietary) Data exist, but are incomplete Dealing with two kinds of uncertainty in modelling public health threats: – – heterogeneity or stochasticity incomplete knowledge and/or systematic measurement errors
SRA Experience • Have encountered 3 types of “insufficient data” 1. 2. 3. • Data do not exist Data cannot be published (proprietary) Data exist, but are incomplete Dealing with two kinds of uncertainty in modelling public health threats: – – heterogeneity or stochasticity incomplete knowledge and/or systematic measurement errors
 SRA Experience & Tools Bacterial infections from ureteroscope v. CJD and Islet cell Risk v. CJD and Vaccine Risk • Viral Infections Due to Improper Re-use of Syringes International and National Expert Advisory Group providing inputs – Expert Elicitation as a tool to gather quantitative information, but also excellent qualitative tool for identification of knowledge gaps in science • Fuzzy Logic and Analysis for modeling of infectious diseases (uncertainty) • Linear deterministic models (variability) • Logical Data Analysis (data mining, artificial intelligence, pattern recognition)
SRA Experience & Tools Bacterial infections from ureteroscope v. CJD and Islet cell Risk v. CJD and Vaccine Risk • Viral Infections Due to Improper Re-use of Syringes International and National Expert Advisory Group providing inputs – Expert Elicitation as a tool to gather quantitative information, but also excellent qualitative tool for identification of knowledge gaps in science • Fuzzy Logic and Analysis for modeling of infectious diseases (uncertainty) • Linear deterministic models (variability) • Logical Data Analysis (data mining, artificial intelligence, pattern recognition)
 Decision-Making Framework for Identifying, Processing and Managing Health Risks Collect Assumptions to Input in Model: -Published literature -Expert consensus Identify the Issue and Its Context Monitor and Evaluate Results Assess Risks and Benefits Run Model Calculations INVOLVE INTERESTED AND AFFECTED PARTIES Implement the Strategy Identify and Analyze Options Select a Strategy Consideration of other Parameters outside of Model, by decision-makers
Decision-Making Framework for Identifying, Processing and Managing Health Risks Collect Assumptions to Input in Model: -Published literature -Expert consensus Identify the Issue and Its Context Monitor and Evaluate Results Assess Risks and Benefits Run Model Calculations INVOLVE INTERESTED AND AFFECTED PARTIES Implement the Strategy Identify and Analyze Options Select a Strategy Consideration of other Parameters outside of Model, by decision-makers
 Risk Analysis Framework 1. 2. 3. Assessment of effectiveness of measures taken Review risk management and/or assessment as necessary D. Monitoring and review Risk Communication 1. 4. B. Risk management and option assessment 3. A. Risk Evaluation 2. 3. C. Implementation of management decision 1. 2. Risk Management Identification of available management options Selection of preferred management option, including consideration of an appropriate safety standard Final management decision 5. 5. 6. 7. A brief description of the situation Product or commodity involved The values expected to be placed at risk (e. g. human health, economic concerns) Potential consequences Consumer perception of the risks The distribution of risks and benefits Identification of TSE/ Blood, cells, tissues and organs safety problem Establishment of a risk profile Ranking of the hazard for risk assessment and risk management priority 4. Establishment of the risk assessment policy for conduct of risk assessment Commitment of resources Commissioning of risk assessment Consideration of risk assessment result ·Risk perception ·Value judgement ·Precautionary principle ·Benefits/ costs ·Other technical factors Regulatory or other control measures Value judgements and policy choices for the risk assessment process ·Hazard identification ·Hazard characterisation ·Exposure assessment ·Risk characterisation Risk Assessment
Risk Analysis Framework 1. 2. 3. Assessment of effectiveness of measures taken Review risk management and/or assessment as necessary D. Monitoring and review Risk Communication 1. 4. B. Risk management and option assessment 3. A. Risk Evaluation 2. 3. C. Implementation of management decision 1. 2. Risk Management Identification of available management options Selection of preferred management option, including consideration of an appropriate safety standard Final management decision 5. 5. 6. 7. A brief description of the situation Product or commodity involved The values expected to be placed at risk (e. g. human health, economic concerns) Potential consequences Consumer perception of the risks The distribution of risks and benefits Identification of TSE/ Blood, cells, tissues and organs safety problem Establishment of a risk profile Ranking of the hazard for risk assessment and risk management priority 4. Establishment of the risk assessment policy for conduct of risk assessment Commitment of resources Commissioning of risk assessment Consideration of risk assessment result ·Risk perception ·Value judgement ·Precautionary principle ·Benefits/ costs ·Other technical factors Regulatory or other control measures Value judgements and policy choices for the risk assessment process ·Hazard identification ·Hazard characterisation ·Exposure assessment ·Risk characterisation Risk Assessment
 Risk Assessment to Risk Management: The Process Perspective • At the highest level, the logic underlying a risk assessment is always the same: Seriousness of Consequences Low High Top concern High Probability of Event Medium Low concern Risk Matrix as a tool for priority setting, Health Canada 2010
Risk Assessment to Risk Management: The Process Perspective • At the highest level, the logic underlying a risk assessment is always the same: Seriousness of Consequences Low High Top concern High Probability of Event Medium Low concern Risk Matrix as a tool for priority setting, Health Canada 2010
 Risk Assessment Structure - Data Requirements * Template developed by TSE Science and Policy Teams under the TSE Secretariat, HPFB
Risk Assessment Structure - Data Requirements * Template developed by TSE Science and Policy Teams under the TSE Secretariat, HPFB
 The concept of De minimis risk
The concept of De minimis risk
 Zooming in… Bloodborne pathogens and health care acquired infection
Zooming in… Bloodborne pathogens and health care acquired infection
 Emerging Infectious Disease Current Activities • Emerging infections are a continuing threat to human health: – – Some transmissible by blood Others show evidence of possible transmissibility • • • HIV HBV/HCV, Burden of illness studies West Nile virus, SARS Babesia species, Dengue virus, and v. CJD Xenotropic murine leukemia related virus (XMRV) and blood H 5 N 1 and blood safety H 1 N 1 and pandemic influenzas in Relation to PPE Anti-microbial resistance (AMR) Chronic Wasting Diseases (CWD) Lyme disease
Emerging Infectious Disease Current Activities • Emerging infections are a continuing threat to human health: – – Some transmissible by blood Others show evidence of possible transmissibility • • • HIV HBV/HCV, Burden of illness studies West Nile virus, SARS Babesia species, Dengue virus, and v. CJD Xenotropic murine leukemia related virus (XMRV) and blood H 5 N 1 and blood safety H 1 N 1 and pandemic influenzas in Relation to PPE Anti-microbial resistance (AMR) Chronic Wasting Diseases (CWD) Lyme disease
 Expert Elicitation for Risk & Disease Models • N 95 masks and infection of healthcare workers by SARS • Dose-response of the Anthrax • v. CJD carried out in March 2009 (funded by Prio. Net Canada and PHAC) • XMRV carried out in September 2010 (PHAC) • CWD to be carried out in 2011 (funded by Prio. Net Canada)
Expert Elicitation for Risk & Disease Models • N 95 masks and infection of healthcare workers by SARS • Dose-response of the Anthrax • v. CJD carried out in March 2009 (funded by Prio. Net Canada and PHAC) • XMRV carried out in September 2010 (PHAC) • CWD to be carried out in 2011 (funded by Prio. Net Canada)
 Structured Expert Elicitation Approach
Structured Expert Elicitation Approach
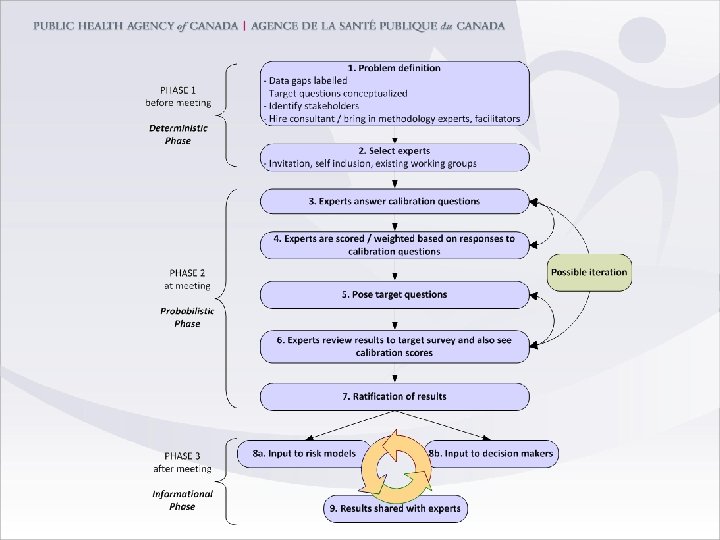
 1. A group of problem domain experts (e) is selected. “E”") Method Overview (1) 1. A group of problem domain experts (e) is selected. “E” is the number of experts participating. 2. Experts meet in person to assess a set of ‘calibration items’, whose true values are known. Each expert expressing his or her views as elemental uncertainty distributions. 3. Expert responses are treated as statistical hypotheses and scored for statistical likelihood that they are correct and display an appropriate ability to gauge uncertainty in their own responses. 4. Calibration and Information scores are computed for each expert e.
Method Overview (1) 1. A group of problem domain experts (e) is selected. “E” is the number of experts participating. 2. Experts meet in person to assess a set of ‘calibration items’, whose true values are known. Each expert expressing his or her views as elemental uncertainty distributions. 3. Expert responses are treated as statistical hypotheses and scored for statistical likelihood that they are correct and display an appropriate ability to gauge uncertainty in their own responses. 4. Calibration and Information scores are computed for each expert e.
 5. The two measures (calibration and information) are combined to form") Method Overview (2) 5. The two measures (calibration and information) are combined to form a weight for each expert. This is done using strictly proper scoring rules: experts receive their maximal expected weight only by stating their true degrees of belief over all the items 6. Experts are then elicited individually regarding their uncertainty judgments in relation to questions of interest, and the performance -based calibration scores obtained in Step 4 are applied to the individual responses. The result is a combined output, which displays the “best answer” but more importantly, weighted poolings of the group of experts’ uncertainty distributions around the best answer
Method Overview (2) 5. The two measures (calibration and information) are combined to form a weight for each expert. This is done using strictly proper scoring rules: experts receive their maximal expected weight only by stating their true degrees of belief over all the items 6. Experts are then elicited individually regarding their uncertainty judgments in relation to questions of interest, and the performance -based calibration scores obtained in Step 4 are applied to the individual responses. The result is a combined output, which displays the “best answer” but more importantly, weighted poolings of the group of experts’ uncertainty distributions around the best answer
 Method Expert Elicitation and the Quantification of risk estimation and uncertainty in relation to infection disease risk • Dr. Roger Cooke (TU Delft, Resources for the Future) – – • “Classical model” Methodology for combining expert opinion Rational Consensus Dr. Willy Aspinall (Aspinall & Associates) – Facilitator and consultant
Method Expert Elicitation and the Quantification of risk estimation and uncertainty in relation to infection disease risk • Dr. Roger Cooke (TU Delft, Resources for the Future) – – • “Classical model” Methodology for combining expert opinion Rational Consensus Dr. Willy Aspinall (Aspinall & Associates) – Facilitator and consultant
 The Software EXCALIBUR TU Delft http: //dutiosc. twi. tudelft. nl/~risk/
The Software EXCALIBUR TU Delft http: //dutiosc. twi. tudelft. nl/~risk/
 The five steps 1. Experts Selection A group of problem") Expert Elicitation (Cooke’s method) The five steps 1. Experts Selection A group of problem domain experts (E) is selected 2. Calibration These experts assess a set of (n) variables within their field (‘seed items’), the true values of which are known Each expert expressing his or her views as elemental uncertainty distributions with quantitative support across selected inter-quantile ranges …
Expert Elicitation (Cooke’s method) The five steps 1. Experts Selection A group of problem domain experts (E) is selected 2. Calibration These experts assess a set of (n) variables within their field (‘seed items’), the true values of which are known Each expert expressing his or her views as elemental uncertainty distributions with quantitative support across selected inter-quantile ranges …
 E Number of experts responding e One representative expert The set of seed/calibration variables to be assessed, where n is the number of seed variables i One representative calibration question The set of true values for X (recall: calibration requires a set of carefully chosen assessment questions with known values) Ex. The set of an expert’s best estimate (median) and 5 -95% confidence bounds for each calibration question i
E Number of experts responding e One representative expert The set of seed/calibration variables to be assessed, where n is the number of seed variables i One representative calibration question The set of true values for X (recall: calibration requires a set of carefully chosen assessment questions with known values) Ex. The set of an expert’s best estimate (median) and 5 -95% confidence bounds for each calibration question i
 Given , the 5, 50, and 95 percentiles split up the variable x’s range into 4 intervals The intrinsic range and of variable i is the smallest interval such that for all , and. He: Expert e is well-calibrated if: Each of is drawn independently according to p distribution,
Given , the 5, 50, and 95 percentiles split up the variable x’s range into 4 intervals The intrinsic range and of variable i is the smallest interval such that for all , and. He: Expert e is well-calibrated if: Each of is drawn independently according to p distribution,
 Experts are scored via two measures: Calibration score: likelihood that expert distributions over the set of seed items correspond to the observed or measured results based on a chi-squared test Information score: measure of “informativeness” compared to a given background distribution, usually a uniform or log-uniform distribution
Experts are scored via two measures: Calibration score: likelihood that expert distributions over the set of seed items correspond to the observed or measured results based on a chi-squared test Information score: measure of “informativeness” compared to a given background distribution, usually a uniform or log-uniform distribution
 2. Calibration (Cont’d) Each expert gives his/her best guess within") Expert Elicitation (Cooke’s method) 2. Calibration (Cont’d) Each expert gives his/her best guess within the intrinsic range [m, M] the median (X 50%), the 5% (X 5%) and 95% (X 95%) confidence bounds 5% m X 5% 45% X 50% 5% X 95% M
Expert Elicitation (Cooke’s method) 2. Calibration (Cont’d) Each expert gives his/her best guess within the intrinsic range [m, M] the median (X 50%), the 5% (X 5%) and 95% (X 95%) confidence bounds 5% m X 5% 45% X 50% 5% X 95% M
 True value for variable 2. Calibration (Cont’d) 1 m 1") Expert Elicitation (Cooke’s method) True value for variable 2. Calibration (Cont’d) 1 m 1 X 1, 5% X 1, 50% X 1, 95% M 1 n mn Xn, 5% Xn, 50% Xn, 95% Mn Ti is the number of times the true values lie in the ith interval out of n
Expert Elicitation (Cooke’s method) True value for variable 2. Calibration (Cont’d) 1 m 1 X 1, 5% X 1, 50% X 1, 95% M 1 n mn Xn, 5% Xn, 50% Xn, 95% Mn Ti is the number of times the true values lie in the ith interval out of n
 2. Calibration (Cont’d) H 0: Expert is well Calibrated Density") Expert Elicitation (Cooke’s method) 2. Calibration (Cont’d) H 0: Expert is well Calibrated Density of Chisquare distribution with 3 degrees of freedom H 0: (S 1, S 2, S 3, S 4)= (. 05, . 45, . 05) p-value 2 n I(s|p)
Expert Elicitation (Cooke’s method) 2. Calibration (Cont’d) H 0: Expert is well Calibrated Density of Chisquare distribution with 3 degrees of freedom H 0: (S 1, S 2, S 3, S 4)= (. 05, . 45, . 05) p-value 2 n I(s|p)
 3. Scoring Based on two measures of performance Calibration Score") Expert Elicitation (Cooke’s method) 3. Scoring Based on two measures of performance Calibration Score (CS) X Information Score (IS) X Indicator (CS>α) = Score of the Expert mis of X 5% that 50% α value X maximizes the. X 95% M scores of the decision maker
Expert Elicitation (Cooke’s method) 3. Scoring Based on two measures of performance Calibration Score (CS) X Information Score (IS) X Indicator (CS>α) = Score of the Expert mis of X 5% that 50% α value X maximizes the. X 95% M scores of the decision maker
 4. Experts Elicitation Experts are then elicited individually regarding their") Expert Elicitation (Cooke’s method) 4. Experts Elicitation Experts are then elicited individually regarding their uncertainty judgments in relation to questions of interest (‘target items’), again within their domain of expertise. 5. Aggregation The weighted pooling of the group of experts’ uncertainty distributions (hi, e) gives the so-called ‘Global decision maker’ (DM). There are several forms that the DM can take, the weighted average is one of them
Expert Elicitation (Cooke’s method) 4. Experts Elicitation Experts are then elicited individually regarding their uncertainty judgments in relation to questions of interest (‘target items’), again within their domain of expertise. 5. Aggregation The weighted pooling of the group of experts’ uncertainty distributions (hi, e) gives the so-called ‘Global decision maker’ (DM). There are several forms that the DM can take, the weighted average is one of them
 Risk Management of TSE’s: Structured Expert Elicitation Following calibration, the experts were asked to answer 22 target questions
Risk Management of TSE’s: Structured Expert Elicitation Following calibration, the experts were asked to answer 22 target questions
 1. What is the dose in") Seven Questions out of the Twenty Two (1/2) 1. What is the dose in grams that would result in 50% of the exposed population becoming infected from human consumption of BSE cervical spinal cord or brain stem from near clinical or clinical cases? (grams) 2. What is the current prevalence of v. CJD infection in the Canadian population? (1 in xxx) 3. What is the mean incubation period for a primary v. CJD infected human [by oral route]? (years) 4. What is the median length of time in months between the oral infection of a human with BSE agent and the capability of one unit of his/her blood to transmit v. CJD? (months)
Seven Questions out of the Twenty Two (1/2) 1. What is the dose in grams that would result in 50% of the exposed population becoming infected from human consumption of BSE cervical spinal cord or brain stem from near clinical or clinical cases? (grams) 2. What is the current prevalence of v. CJD infection in the Canadian population? (1 in xxx) 3. What is the mean incubation period for a primary v. CJD infected human [by oral route]? (years) 4. What is the median length of time in months between the oral infection of a human with BSE agent and the capability of one unit of his/her blood to transmit v. CJD? (months)
 5. What is the mean incubation") Seven Questions out of the Twenty Two (2/2) 5. What is the mean incubation period for a secondary v. CJD infected human [by transfusion]? (years) 6. What is the probability of transmission of v. CJD by contaminated neurosurgery instruments if reused in neurosurgery after one cycle of standard sterilization procedures? (%) 7. How long is the incubation period for secondary transmission of v. CJD by v. CJD contaminated neurosurgical instruments [brain to brain usage]? (months)
Seven Questions out of the Twenty Two (2/2) 5. What is the mean incubation period for a secondary v. CJD infected human [by transfusion]? (years) 6. What is the probability of transmission of v. CJD by contaminated neurosurgery instruments if reused in neurosurgery after one cycle of standard sterilization procedures? (%) 7. How long is the incubation period for secondary transmission of v. CJD by v. CJD contaminated neurosurgical instruments [brain to brain usage]? (months)
 What did the experts say?
What did the experts say?
 Target Question #1 What is the dose in grams that would result in 50% of the exposed population becoming infected from human consumption of BSE cervical spinal cord or brain stem from near clinical or clinical cases? (grams) Best expert judgment: about 1 gram.
Target Question #1 What is the dose in grams that would result in 50% of the exposed population becoming infected from human consumption of BSE cervical spinal cord or brain stem from near clinical or clinical cases? (grams) Best expert judgment: about 1 gram.
 Target Question #2 What is the current prevalence of v. CJD infection in the Canadian population? (1 in xxx) Best expert judgement: the current prevalence of v. CJD in Canada is less than 1 in 500, 000.
Target Question #2 What is the current prevalence of v. CJD infection in the Canadian population? (1 in xxx) Best expert judgement: the current prevalence of v. CJD in Canada is less than 1 in 500, 000.
 Twelve Risks and Pairwise Comparisons
Twelve Risks and Pairwise Comparisons
 Twelve Risks and Pairwise Comparisons 6 FFP plasma transfusion 4 Platelet transfusion 2 1 5 12 Corneal transplant 3 Hematopoietic stem cell transplant 10 Whole blood transfusion Human derived urine fertility products Dura Mater transplant Bone marrow transplant Packed red blood cells Dental tissue graft 8 pd. FVIII pd. FXI 9 7 11
Twelve Risks and Pairwise Comparisons 6 FFP plasma transfusion 4 Platelet transfusion 2 1 5 12 Corneal transplant 3 Hematopoietic stem cell transplant 10 Whole blood transfusion Human derived urine fertility products Dura Mater transplant Bone marrow transplant Packed red blood cells Dental tissue graft 8 pd. FVIII pd. FXI 9 7 11
 Twelve Risks and Pairwise Comparisons Platelet transfusion FFP plasma transfusion Whole blood transfusion Dura Mater transplant Packed red blood cells Dental tissue graft Whole blood transfusion Dura Mater transplant Packed red blood cells Dental tissue graft
Twelve Risks and Pairwise Comparisons Platelet transfusion FFP plasma transfusion Whole blood transfusion Dura Mater transplant Packed red blood cells Dental tissue graft Whole blood transfusion Dura Mater transplant Packed red blood cells Dental tissue graft
 Twelve Risks and Pairwise Comparisons Platelet transfusion FFP plasma transfusion Whole blood transfusion Dura Mater transplant Packed red blood cells Platelet transfusion > FFP plasma transfusion Platelet transfusion > < = Dental tissue graft > > > FFP plasma transfusion > Whole blood > transfusion < < FFP plasma Whole blood transfusion > > < > > Platelet transfusion < Whole blood transfusion > Circular triads Dura Mater transplant Packed red blood cells > Dental tissue graft
Twelve Risks and Pairwise Comparisons Platelet transfusion FFP plasma transfusion Whole blood transfusion Dura Mater transplant Packed red blood cells Platelet transfusion > FFP plasma transfusion Platelet transfusion > < = Dental tissue graft > > > FFP plasma transfusion > Whole blood > transfusion < < FFP plasma Whole blood transfusion > > < > > Platelet transfusion < Whole blood transfusion > Circular triads Dura Mater transplant Packed red blood cells > Dental tissue graft
 Preliminary Analysis • Test of Inconsistency To test whether each expert gave his/her responses randomly Chi-square test with 21 degrees of freedom 11 tests are significant with p-value<. 01 • Measure of consistence 2 experts 9 8 0. 71 0 5. 6 9 42 42 7 0. 0 1. 8 9 0. 43 0 1. 9 9 42 79 43 0 6. 9 9 0. 4 71 2 experts 1
Preliminary Analysis • Test of Inconsistency To test whether each expert gave his/her responses randomly Chi-square test with 21 degrees of freedom 11 tests are significant with p-value<. 01 • Measure of consistence 2 experts 9 8 0. 71 0 5. 6 9 42 42 7 0. 0 1. 8 9 0. 43 0 1. 9 9 42 79 43 0 6. 9 9 0. 4 71 2 experts 1
 Preliminary Analysis • Statistical Test of Agreement To test whether the agreement between the group of experts is due to chance Chi-square test with 90 degrees of freedom Test is significant with p-value<. 01 • Coefficient of Agreement Co. A=. 3218
Preliminary Analysis • Statistical Test of Agreement To test whether the agreement between the group of experts is due to chance Chi-square test with 90 degrees of freedom Test is significant with p-value<. 01 • Coefficient of Agreement Co. A=. 3218
") Probabilistic Inversion • Assign a random utility function (U 1 , …, U 12) to each item • Scale the utilities to the interval [0, 1] • From the aggregated preference matrices
Probabilistic Inversion • Assign a random utility function (U 1 , …, U 12) to each item • Scale the utilities to the interval [0, 1] • From the aggregated preference matrices
 Probabilistic Inversion Given the joint density function f, we can find Pij Given Pij , we want to find the joint density function f Space of Pairwise Ordered Utilities I( Ui >Uj ) and Pij
Probabilistic Inversion Given the joint density function f, we can find Pij Given Pij , we want to find the joint density function f Space of Pairwise Ordered Utilities I( Ui >Uj ) and Pij
 2. Parameter Fitting for") Probabilistic Inversion • Numerical algorithms 1. Iterative Proportional Fitting (IPF) 2. Parameter Fitting for Uncertain Models (PARFUM) • UNIBALANCE TU Delft http: //dutiosc. twi. tudelft. nl/~risk/
Probabilistic Inversion • Numerical algorithms 1. Iterative Proportional Fitting (IPF) 2. Parameter Fitting for Uncertain Models (PARFUM) • UNIBALANCE TU Delft http: //dutiosc. twi. tudelft. nl/~risk/
") Probabilistic Inversion • Marginal distributions • Items’ scores (the mean of the random utility) • Correlation
Probabilistic Inversion • Marginal distributions • Items’ scores (the mean of the random utility) • Correlation
 Results Transmission Route Score St. dev. 1 Platelet transfusion 0. 5599 0. 2318 2 FFP plasma transfusion 0. 6266 0. 2501 3 Whole blood transfusion 0. 7384 0. 2075 4 Dura Mater transplant 0. 9520 0. 0370 5 Packed red blood cells 0. 6002 0. 2742 6 Dental tissue graft 0. 2756 0. 2484 7 Corneal transplant 0. 6953 0. 2263 8 Hematopoietic stem cell transplant 0. 3197 0. 1752 9 Human derived urine fertility products 0. 3160 0. 2034 10 Bone marrow transplant 0. 4966 0. 2195 11 pd. FVIII 0. 4353 0. 2524 12 pd. FXI 0. 3992 0. 2340
Results Transmission Route Score St. dev. 1 Platelet transfusion 0. 5599 0. 2318 2 FFP plasma transfusion 0. 6266 0. 2501 3 Whole blood transfusion 0. 7384 0. 2075 4 Dura Mater transplant 0. 9520 0. 0370 5 Packed red blood cells 0. 6002 0. 2742 6 Dental tissue graft 0. 2756 0. 2484 7 Corneal transplant 0. 6953 0. 2263 8 Hematopoietic stem cell transplant 0. 3197 0. 1752 9 Human derived urine fertility products 0. 3160 0. 2034 10 Bone marrow transplant 0. 4966 0. 2195 11 pd. FVIII 0. 4353 0. 2524 12 pd. FXI 0. 3992 0. 2340
 1. Dura Mater transplant 1. 0000 2.") Results Relative Ranking Transmission Route Score (normalized) 1. Dura Mater transplant 1. 0000 2. Whole blood transfusion 0. 6842 3. Corneal transplant 0. 6206 4. FFP plasma transfusion 0. 5190 5. Packed red blood cells 0. 4799 6. Platelet transfusion 0. 4203 7. Bone marrow transplant 0. 3268 8. pd. FVIII 0. 2360 9. pd. FXI 0. 1827 10. Hematopoietic stem cell transplant 0. 0652 11. Human derived urine fertility products 0. 0597 12. Dental tissue graft 0. 0000
Results Relative Ranking Transmission Route Score (normalized) 1. Dura Mater transplant 1. 0000 2. Whole blood transfusion 0. 6842 3. Corneal transplant 0. 6206 4. FFP plasma transfusion 0. 5190 5. Packed red blood cells 0. 4799 6. Platelet transfusion 0. 4203 7. Bone marrow transplant 0. 3268 8. pd. FVIII 0. 2360 9. pd. FXI 0. 1827 10. Hematopoietic stem cell transplant 0. 0652 11. Human derived urine fertility products 0. 0597 12. Dental tissue graft 0. 0000
 Results
Results
 Results
Results
 BSE and v. CJD EE Exercises in Ottawa March 2008, 2009 • What is the size of the bovine to human species barrier in the MM genotype for oral exposure to the classical BSE agent? 2008 2009
BSE and v. CJD EE Exercises in Ottawa March 2008, 2009 • What is the size of the bovine to human species barrier in the MM genotype for oral exposure to the classical BSE agent? 2008 2009
 More research is needed • Opinion aggregation for different inter-dependent schools • Testing inconsistency of experts’ opinions • Finding numerical algorithms for probabilistic inversion method • Fuzzy logic in EE
More research is needed • Opinion aggregation for different inter-dependent schools • Testing inconsistency of experts’ opinions • Finding numerical algorithms for probabilistic inversion method • Fuzzy logic in EE
 Submitted … 1. Comparative Expert Judgment Elicitation using the Classical Model and EXCALIBUR under Conditions of Uncertainty for Prion Disease Risks 2. Expert Elicitation for the Judgment of Prion Disease Risk Uncertainties using the Classical Model and , EXCALIBUR and UNIBALANCE By Michael G. Tyshenko, Susie El. Saadany, , Tamer Oraby, Shalu Darshan, Willy Aspinall, Roger Cooke, and Daniel Krewski
Submitted … 1. Comparative Expert Judgment Elicitation using the Classical Model and EXCALIBUR under Conditions of Uncertainty for Prion Disease Risks 2. Expert Elicitation for the Judgment of Prion Disease Risk Uncertainties using the Classical Model and , EXCALIBUR and UNIBALANCE By Michael G. Tyshenko, Susie El. Saadany, , Tamer Oraby, Shalu Darshan, Willy Aspinall, Roger Cooke, and Daniel Krewski
 Conclusion • • • Best communication of complex methods to stakeholders? Validity of complex methods when high uncertainty involved? Best contribution in the name of precautionary principle? – National – international collaboration in development of specific tools Involvement of all partners – – Face to face meetings, scientific and policy networks combined.
Conclusion • • • Best communication of complex methods to stakeholders? Validity of complex methods when high uncertainty involved? Best contribution in the name of precautionary principle? – National – international collaboration in development of specific tools Involvement of all partners – – Face to face meetings, scientific and policy networks combined.
 If you will begin with certainties, you shall end in doubts, but if you will content to begin with doubts, you shall end in almost certainties. - Francis Bacon
If you will begin with certainties, you shall end in doubts, but if you will content to begin with doubts, you shall end in almost certainties. - Francis Bacon
 Funded by High Impact Grant Project teams from: • Public Health Agency of Canada, Statistics and Risk Assessment Section Dr. Susie El. Saadany Angela Catford Caroline Desjardins • Mc. Laughlin Centre for Population Health Risk Assessment, University of Ottawa Dr. Daniel Krewski Dr. Michael Tyshenko Dr. Shalu Darshan Dr. Mustafa Al-Zoughool Dr. Tamer Oraby
Funded by High Impact Grant Project teams from: • Public Health Agency of Canada, Statistics and Risk Assessment Section Dr. Susie El. Saadany Angela Catford Caroline Desjardins • Mc. Laughlin Centre for Population Health Risk Assessment, University of Ottawa Dr. Daniel Krewski Dr. Michael Tyshenko Dr. Shalu Darshan Dr. Mustafa Al-Zoughool Dr. Tamer Oraby