
Renal Pathology Introduction: 150gm: each kidney 1700 liters












 Children: minimal change disease Characterized by loss of foot processes")



 glomeruli show partial (segmental) hyalinization Unknown")







 Upper Respiratory Infection IgA in")



























540-6-_renal_pathophysiology.ppt
- Количество слайдов: 57
Renal Pathology
Introduction: 150gm: each kidney 1700 liters of blood filtered 180 L of G. filtrate 1.5 L of urine / day. Kidney is a retro-peritoneal organ Blood supply: Renal Artery & Vein One half of kidney is sufficient – reserve kidney function: Filtration, Excretion, Secretion, Hormone synthesis.
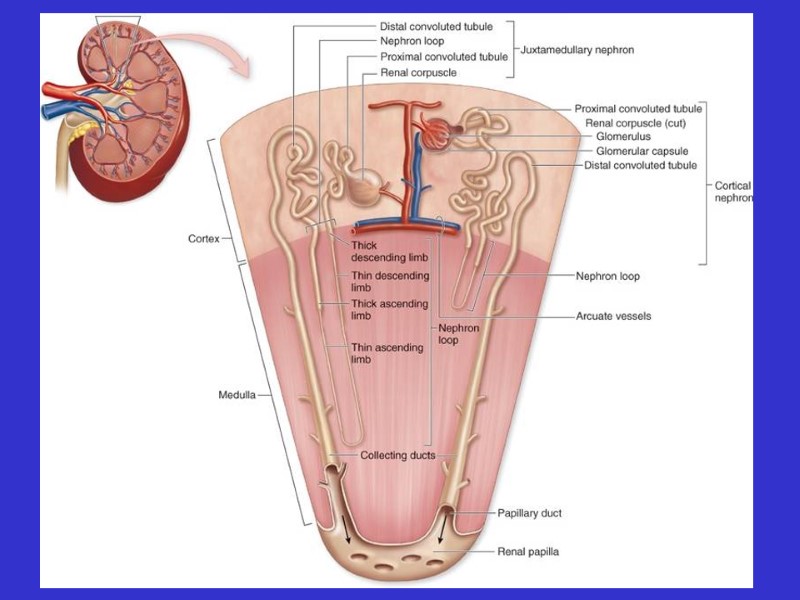
Kidney Location:
Kidney Anatomy:
Renal Pathology Outline Glomerular diseases: Glomerulonephritis Tubular diseases: Acute tubular necrosis interstitial diseases: Pyelonephritis Diseases involving blood vessels: Nephrosclerosis Cystic diseases Tumors
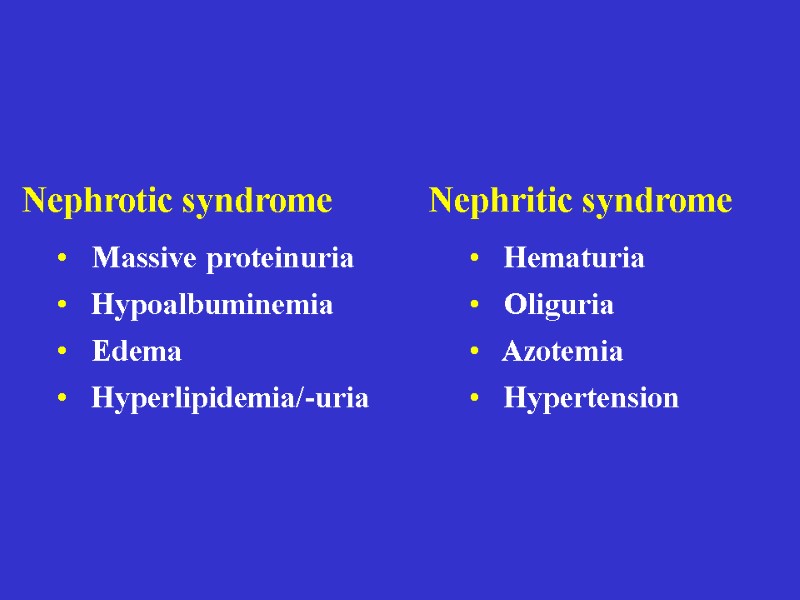
Clinical Syndromes: Nephritic syndrome. Oliguria, Haematuria, Proteinuria, Oedema. Nephrotic syndrome. Gross proteinuria, hyperlipidemia, Acute renal failure Oliguria, loss of Kidney function - within weeks Chronic renal failure. Over months and years - Uremia
Introduction Functions of the kidney: excretion of waste products regulation of water/salt maintenance of acid/base balance secretion of hormones Diseases of the kidney glomeruli tubules interstitium vessels
Azotemia: BUN, creatinine Uremia: azotemia + more problems Acute renal failure: oliguria Chronic renal failure: prolonged uremia Abnormal findings
Glomerular diseases Nephrotic syndrome Minimal change disease Focal segmental glomerulosclerosis Membranous nephropathy Nephritic syndrome Post-infectious GN IgA (immune) nephropathy
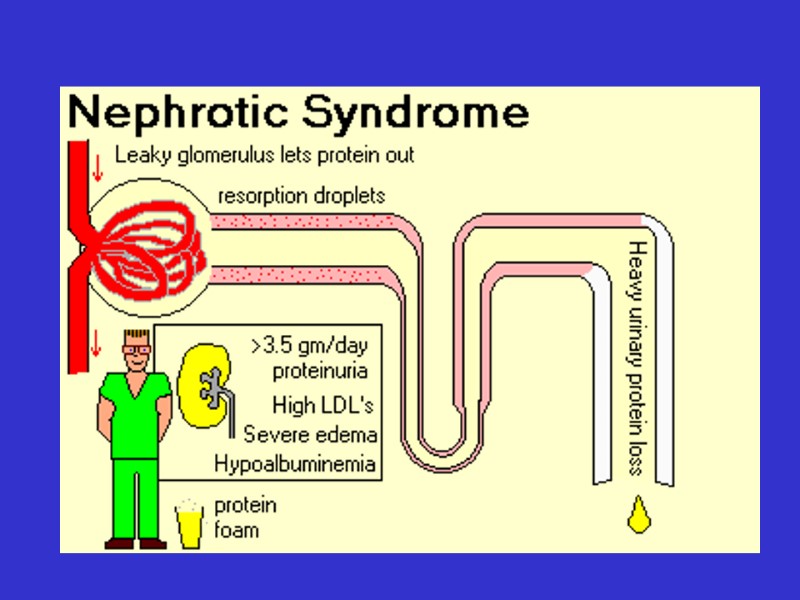
Nephrotic Syndrome Massive proteinuria Hypoalbuminemia Edema Hyperlipidemia
Adults: systemic disease (diabetes) Children: minimal change disease Characterized by loss of foot processes Good prognosis Causes
Minimal change disease
Minimal change disease Normal glumerular structure
Normal glomerulus Minimal change disease
Focal Segmental Glomerulosclerosis Primary or secondary Some (focal) glomeruli show partial (segmental) hyalinization Unknown pathogenesis Poor prognosis
Focal segmental glomerulosclerosis
Membranous Glomerulonephritis Autoimmune reaction against unknown renal antigen Immune complexes Thickened GBM Subepithelial deposits
Membranous glomerulonephritis
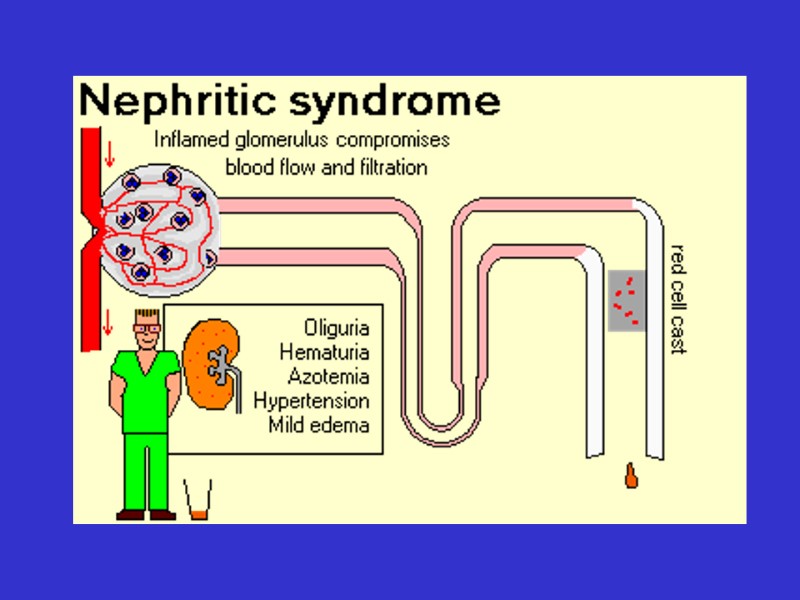
Nephritic Syndrome Hematuria Oliguria, azotemia Hypertension
Post-infectious GN, IgA nephropathy Immunologically-mediated Characterized by proliferative changes and inflammation Causes
Post-Infectious Glomerulonephritis Child after streptococcal throat infection Immune complexes Hypercellular glomeruli Subepithelial humps
Post-infectious glomerulonephritis
IgA Nephropathy Common! Child with hematuria after (URI) Upper Respiratory Infection IgA in mesangium Variable prognosis
IgA nephropathy
Tubular and interstitial diseases Inflammatory lesions pyelonephritis
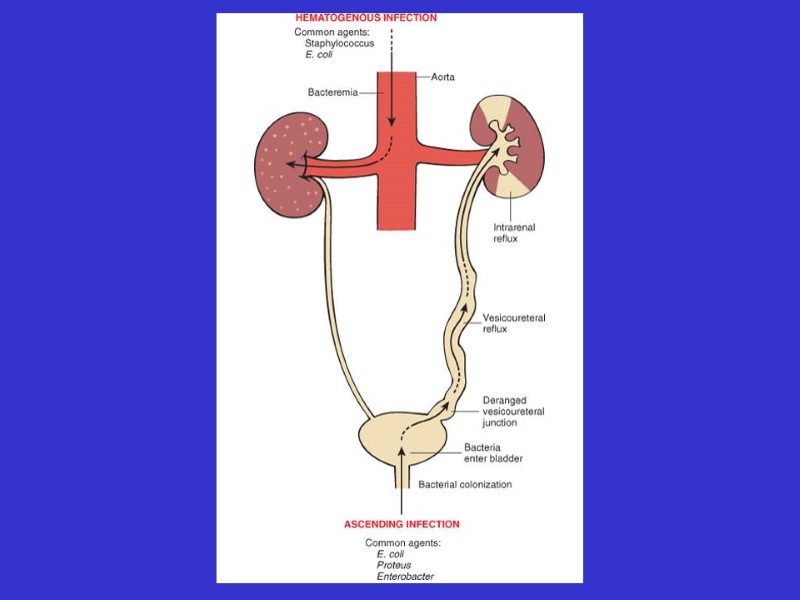
Pyelonephritis Invasive kidney infection Usually ascends from UTI Fever, flank pain Organisms: E. coli, Proteus
Women, elderly Patients with catheters or mal-formations Dysuria, frequency Organisms: E. coli, Proteus Urinary Tract Infection
Acute pyelonephritis with abscesses
Pyelonephritis
Cellular cast
Chronic pyelonephritis
Drug-Induced Interstitial Nephritis Antibiotics, NSAIDS IgE and T-cell-mediated immune reaction Fever, eosinophilia, hematuria Patient usually recovers Analgesic nephritis is different (bad)
Drug-induced interstitial nephritis
Acute Tubular Necrosis The most common cause of ARF! Reversible tubular injury Many causes: ischemic (shock), toxic (drugs) Most patients recover
Acute tubular necrosis
Benign Nephrosclerosis Found in patients with benign hypertension Hyaline thickening of arterial walls Leads to mild functional impairment Rarely fatal
Benign nephrosclerosis
Malignant nephrosclerosis Arises in malignant hypertension Hyperplastic vessels Ischemia of kidney Medical emergency
5% of cases of hypertension Super-high blood pressure, encephalopathy, heart abnormalities First sign often headache, scotomas Decreased blood flow to kidney leads to increased renin, which leads to increased BP! 5y survival: 50% Malignant Hypertension
Malignant hypertension
Adult Polycystic Kidney Disease Autosomal dominant Huge kidneys full of cysts Usually no symptoms until 30 years Associated with brain aneurysms.
Adult polycystic kidney disease
Childhood Polycystic Kidney Disease Autosomal recessive Numerous small cortical cysts Associated with liver cysts Patients often die in infancy
Childhood polycystic kidney disease
Medullary Cystic Kidney Disease Chronic renal failure in children Complex inheritance Kidneys contracted, with many cysts Progresses to end-stage renal disease
Tumors Renal cell carcinoma Bladder carcinoma
Renal Cell Carcinoma Derived from tubular epithelium Smoking, hypertension, cadmium exposure Hematuria, abdominal mass, flank pain If metastatic, 5y survival = 5%
Renal cell carcinoma
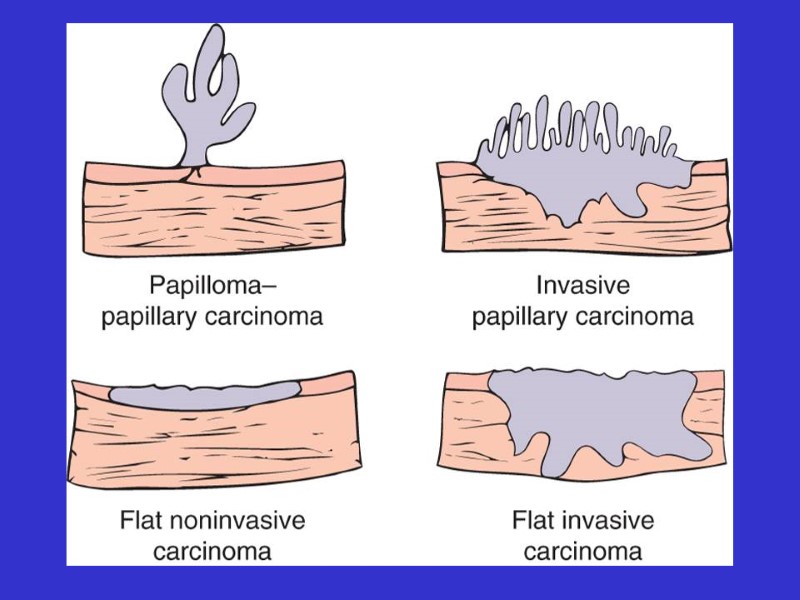
Bladder Carcinoma Derived from transitional epithelium Present with painless hematuria Prognosis depends on grade and depth of invasion Overall 5y survival = 50%
Bladder carcinoma