

745e0096ca4f660aab319c128ad77d0c.ppt
- Количество слайдов: 48
 Reforms in the Primary Health Care in Macedonia: Why and How? Assoc. Prof. Tozija Fimka MD, Ph. D Prof. Gjorgjev Dragan MD. Ph. D Republic Institute for Health Protection - Skopje
Reforms in the Primary Health Care in Macedonia: Why and How? Assoc. Prof. Tozija Fimka MD, Ph. D Prof. Gjorgjev Dragan MD. Ph. D Republic Institute for Health Protection - Skopje

 Independence : 8 September 1991 8 April 1993 - OUN; 12 May 1993 - WHO
Independence : 8 September 1991 8 April 1993 - OUN; 12 May 1993 - WHO
 AIM > current organization and functional activity of PHC in the health care delivery system > reform activities: WHY and HOW > PHC in future
AIM > current organization and functional activity of PHC in the health care delivery system > reform activities: WHY and HOW > PHC in future
 HEALTH STATUS OF THE POPULATION IN THE REPUBLIC OF MACEDONIA AND PRIORITY HEALTH PROBLEMS IN 2004
HEALTH STATUS OF THE POPULATION IN THE REPUBLIC OF MACEDONIA AND PRIORITY HEALTH PROBLEMS IN 2004
 BASIC INDICATORS IN 2004 Area Population Administrative division 25 713 sq. km 2. 049. 000 ( Urban 59. 6/Rural 40. 4) 84 municipalities Ethnicity/languages Macedonian 64, 2%, Albanian 25, 2%, Turkish 3, 9%, Roma 2, 7%, Serbian 1, 8%, Vlashos 1, 0%, Other 1, 2% Religions Orthodox Christian 67% , Muslim 30% Number of live births 27761 Literacy rate 94% Unemployment rate 39% Life expectancy at birth (2002) Mortality - rate per 1000: Infant mortality rate – per 1000 live births: Neonatal deaths per 1000 live births: * Health for all - WHO 73. 4 8. 9 10. 2 8. 6
BASIC INDICATORS IN 2004 Area Population Administrative division 25 713 sq. km 2. 049. 000 ( Urban 59. 6/Rural 40. 4) 84 municipalities Ethnicity/languages Macedonian 64, 2%, Albanian 25, 2%, Turkish 3, 9%, Roma 2, 7%, Serbian 1, 8%, Vlashos 1, 0%, Other 1, 2% Religions Orthodox Christian 67% , Muslim 30% Number of live births 27761 Literacy rate 94% Unemployment rate 39% Life expectancy at birth (2002) Mortality - rate per 1000: Infant mortality rate – per 1000 live births: Neonatal deaths per 1000 live births: * Health for all - WHO 73. 4 8. 9 10. 2 8. 6
 Health care resources , utilization and costs in 2004 Number of hospitals 54 Number of physicians, PP 4573 Number of general practitioners, PP 1619 Number of dentists, PP 1183 Number of pharmacists, PP 2 Number of nurses, PP Average length of stay in days, all hospitals Outpatient contact person per year GDP Health expenditure of GDP per capita Public health expenditure as % of total health expenditure 11056 11. 8 3 $ 1690 6% $ 106 93. 9
Health care resources , utilization and costs in 2004 Number of hospitals 54 Number of physicians, PP 4573 Number of general practitioners, PP 1619 Number of dentists, PP 1183 Number of pharmacists, PP 2 Number of nurses, PP Average length of stay in days, all hospitals Outpatient contact person per year GDP Health expenditure of GDP per capita Public health expenditure as % of total health expenditure 11056 11. 8 3 $ 1690 6% $ 106 93. 9
 HEALTH and SOCIO-ECONOMIC PROBLEMS • • • Poverty and unemployment High rates of mortality and morbidity from CVD High rates of mortality and morbidity from cancer Explosion of addictive drug abuse Increased violence and injuries Hyper production and surplus of staff (doctors) Lack of properly qualified experts in public health Lack of qualified managers of health programs Underutilization and deterioration of the health facilities
HEALTH and SOCIO-ECONOMIC PROBLEMS • • • Poverty and unemployment High rates of mortality and morbidity from CVD High rates of mortality and morbidity from cancer Explosion of addictive drug abuse Increased violence and injuries Hyper production and surplus of staff (doctors) Lack of properly qualified experts in public health Lack of qualified managers of health programs Underutilization and deterioration of the health facilities
 HEALTH CARE SYSTEM - MACEDONIA • • • Parliament Government Ministry of Health Insurance Fund Medical Chamber, Dentistry Chamber, Pharmaceutical Chamber Health Institutions – Tertiary health care: RIHP, Clinical Center, Special Hospital and Institutions – Secondary health care: IHP, Spec. consul. services, General and Special Hospitals, Rehabilitation Centres – Primary Health Care: Units of the IHP, Health stations, Health Centers, Medical centers-part of Health Centers, private health organizations, pharmacies
HEALTH CARE SYSTEM - MACEDONIA • • • Parliament Government Ministry of Health Insurance Fund Medical Chamber, Dentistry Chamber, Pharmaceutical Chamber Health Institutions – Tertiary health care: RIHP, Clinical Center, Special Hospital and Institutions – Secondary health care: IHP, Spec. consul. services, General and Special Hospitals, Rehabilitation Centres – Primary Health Care: Units of the IHP, Health stations, Health Centers, Medical centers-part of Health Centers, private health organizations, pharmacies
 Net of health organizations in PHC
Net of health organizations in PHC
 Medical units - PHC in 2000 Department: Medical units Facilities General medicine Children aged 0 -6 y. Schoolchildren Labor medicine Gynecology 51 457 82 78 91 Doctors Spec. 999 (19. %) 299 (53%) 175 (65%) 161 (69%) 101 (97%) Population/1 p 1401 680 2448 7830
Medical units - PHC in 2000 Department: Medical units Facilities General medicine Children aged 0 -6 y. Schoolchildren Labor medicine Gynecology 51 457 82 78 91 Doctors Spec. 999 (19. %) 299 (53%) 175 (65%) 161 (69%) 101 (97%) Population/1 p 1401 680 2448 7830
 Functional activity in PHC Insufficient preventive activities: General medicine only 0. 5%; Labor medicine 8. 8%; Health care of school children and youth 10. 4%; Health care of children aged 0 -6 y. is 20. 9%; Health care of women 40. 6%
Functional activity in PHC Insufficient preventive activities: General medicine only 0. 5%; Labor medicine 8. 8%; Health care of school children and youth 10. 4%; Health care of children aged 0 -6 y. is 20. 9%; Health care of women 40. 6%
 Most frequent diseases with the adult population in Macedonia in 2000
Most frequent diseases with the adult population in Macedonia in 2000
 Most frequent diseases with the children and youth in Macedonia in 2000
Most frequent diseases with the children and youth in Macedonia in 2000
 WHY REFORMS? > SWOT analysis > RAND’s research /survey Capitation Evaluation Program > Research in IPU > Needs assessment
WHY REFORMS? > SWOT analysis > RAND’s research /survey Capitation Evaluation Program > Research in IPU > Needs assessment
 > Well developed net of organizations in PHC") ADVANTAGES > Accessibility (geographical, financial, temporal) > Well developed net of organizations in PHC > Increasing number of private organizations > Large number of doctors with theoretical knowledge > Very high % of immunization > High rate of solidarity > Large package of health services
ADVANTAGES > Accessibility (geographical, financial, temporal) > Well developed net of organizations in PHC > Increasing number of private organizations > Large number of doctors with theoretical knowledge > Very high % of immunization > High rate of solidarity > Large package of health services
 > Disparity between urban and") WEAKNESSES > Hyper production and surplus of staff (doctors) > Disparity between urban and rural > Lack of CME and clinical protocols > Lack of therapeutically guidelines (non-rational prescribing) > Bad status of the clinics > Lack of equipment and drugs > Lack of information technology > Lack of financial motivation > Lack of managers
WEAKNESSES > Hyper production and surplus of staff (doctors) > Disparity between urban and rural > Lack of CME and clinical protocols > Lack of therapeutically guidelines (non-rational prescribing) > Bad status of the clinics > Lack of equipment and drugs > Lack of information technology > Lack of financial motivation > Lack of managers
 World Bank in the Health Sector 1996 -2004 ü 1996 -2002 - Health Sector Transition Project: Highly satisfactory ranked PHC CME and Perinatal Project ü 2002 - 2004 – Preparation of the Health Sector Management Project – PHRD Grant Government of Japan ü Public Sector Management Adjustment Credit - PSMAC) – support to the HIF and MOH- Grant Government of Netherlands ü 2004 - Health Sector Management Project – Loan agreement signed
World Bank in the Health Sector 1996 -2004 ü 1996 -2002 - Health Sector Transition Project: Highly satisfactory ranked PHC CME and Perinatal Project ü 2002 - 2004 – Preparation of the Health Sector Management Project – PHRD Grant Government of Japan ü Public Sector Management Adjustment Credit - PSMAC) – support to the HIF and MOH- Grant Government of Netherlands ü 2004 - Health Sector Management Project – Loan agreement signed
 Health Sector Transition Project 1996 -2002 Key dates: ü Approved: ü Revised: ü Closed: 20/06/1996 24/03/1999 31/03/2002 Costs and financing: 17. 1 million USD 14. 5 World Bank IDA Credit 2. 6 Government contribution
Health Sector Transition Project 1996 -2002 Key dates: ü Approved: ü Revised: ü Closed: 20/06/1996 24/03/1999 31/03/2002 Costs and financing: 17. 1 million USD 14. 5 World Bank IDA Credit 2. 6 Government contribution
 HEALTH SECTOR TRANSITION PROJECT 1996 -2002 AIMS: > Better health of the population > Better choice for patients > Better quality of services > Better efficiency of PHC > Better fiscal sustainability of PHC
HEALTH SECTOR TRANSITION PROJECT 1996 -2002 AIMS: > Better health of the population > Better choice for patients > Better quality of services > Better efficiency of PHC > Better fiscal sustainability of PHC
 PHC Reform activities 1. Component: Financing and management > Defining a new package of health services > New method of payment – capitation for private physicians > Contracting of private physicians > Establishing of Information System in HIF
PHC Reform activities 1. Component: Financing and management > Defining a new package of health services > New method of payment – capitation for private physicians > Contracting of private physicians > Establishing of Information System in HIF
 Reform activities 2. Basic health services >Improvement of the net of primary health organizations >Improvement of the infrastructure in PHC - rural >Professional development of the doctors: CPD, CME
Reform activities 2. Basic health services >Improvement of the net of primary health organizations >Improvement of the infrastructure in PHC - rural >Professional development of the doctors: CPD, CME
 Reform activities 3. Pharmaceutical policy and supply >Promotion of rational pharmacotherapy >Training for rational prescribing >Therapeutical guidelines
Reform activities 3. Pharmaceutical policy and supply >Promotion of rational pharmacotherapy >Training for rational prescribing >Therapeutical guidelines
 ACHIEVED RESULTS - REGULATION >Selected doctor - 1997 >Capitation - private doctors - July 2001 (contracted 500 private doctors) >Basic Benefit Package - By-law 2000 >New By-law on Co-payment - 2001 >Provision of staff in the rural clinics: prepared plan for redistribution of 200 doctors in 169 rural clinics, 1998 >Establishing teams in PHC - plan for reorganization of services -2001
ACHIEVED RESULTS - REGULATION >Selected doctor - 1997 >Capitation - private doctors - July 2001 (contracted 500 private doctors) >Basic Benefit Package - By-law 2000 >New By-law on Co-payment - 2001 >Provision of staff in the rural clinics: prepared plan for redistribution of 200 doctors in 169 rural clinics, 1998 >Establishing teams in PHC - plan for reorganization of services -2001
 ACHIEVED RESULTS – EQUIPMENT Prepared standard for equipment in PHC (for the doctors and clinics) Procurement of EQUIPMENT through bidding (tenders) (value of 3 M $) > for 4 CME Centers > for attendees > for PHC clinics
ACHIEVED RESULTS – EQUIPMENT Prepared standard for equipment in PHC (for the doctors and clinics) Procurement of EQUIPMENT through bidding (tenders) (value of 3 M $) > for 4 CME Centers > for attendees > for PHC clinics
 ACHIEVED RESULTS – CONTINUOUS MEDICAL EDUCATION Pilot Project: November 1998 - September 2000 Second phase: October 2000 - December 2001 > 4 CME Centres > 32 Educators > 15 Guidelines > Courses - Foundation course and short courses > 1086 attendees Strategy for specialization in PHC and CME Strategy for accreditation of the doctors in MK
ACHIEVED RESULTS – CONTINUOUS MEDICAL EDUCATION Pilot Project: November 1998 - September 2000 Second phase: October 2000 - December 2001 > 4 CME Centres > 32 Educators > 15 Guidelines > Courses - Foundation course and short courses > 1086 attendees Strategy for specialization in PHC and CME Strategy for accreditation of the doctors in MK
 CME CENTERS
CME CENTERS
 CLINICAL SKILLS HANDS-ON- education
CLINICAL SKILLS HANDS-ON- education
 15 GUIDELINES W For most frequent medical problems and diseases W Prepared by team of CME educators – local and international W Customised, translated, peer reviewed, edited and published
15 GUIDELINES W For most frequent medical problems and diseases W Prepared by team of CME educators – local and international W Customised, translated, peer reviewed, edited and published
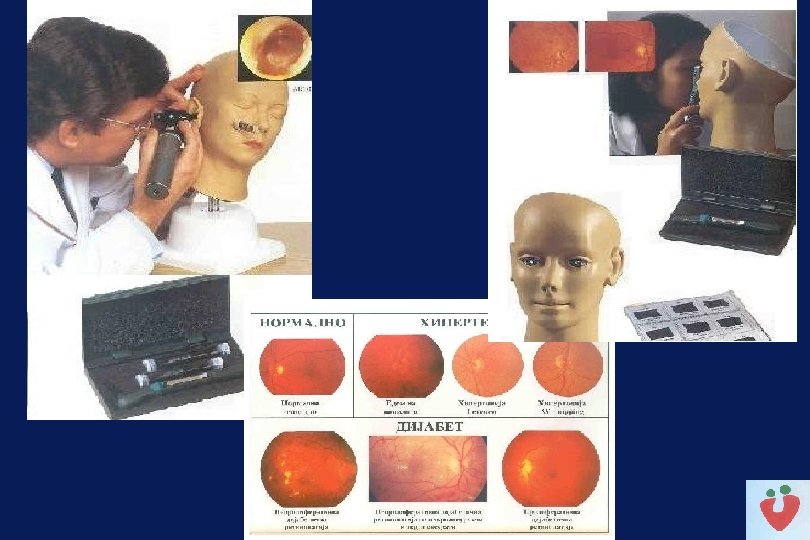
 OTHER MATERIALS W Tables for cardiovascular risks: males/females W Normogram for Body Mass Index W Changes on the eye fundus for the most important diseases in PHC
OTHER MATERIALS W Tables for cardiovascular risks: males/females W Normogram for Body Mass Index W Changes on the eye fundus for the most important diseases in PHC
 MEDICAL DOCUMENTATION W Draft forms for record keeping for chronic diseases the W Final version customised, edited and published
MEDICAL DOCUMENTATION W Draft forms for record keeping for chronic diseases the W Final version customised, edited and published
 LONG TERM CME STRATEGY Produced by: · Doctors, educators · Professors from UK · Professors from Medical Faculty Skopje, · Doctors Chamber · Macedonian Medical Association
LONG TERM CME STRATEGY Produced by: · Doctors, educators · Professors from UK · Professors from Medical Faculty Skopje, · Doctors Chamber · Macedonian Medical Association
 MEMORANDUM OF UNDERSTANDING 17. 12. 99 i 26. 12. 2001 W W Minister of health President of Doctors Chamber President of Macedonian Medical Association Dean of Medical Faculty W Improve the Standards of PHC in accordance with EU
MEMORANDUM OF UNDERSTANDING 17. 12. 99 i 26. 12. 2001 W W Minister of health President of Doctors Chamber President of Macedonian Medical Association Dean of Medical Faculty W Improve the Standards of PHC in accordance with EU
 INSTITUTIONALISATION OF CME W Strategy for CME and specialisation W International Centre for studies in PHC and CME within the Medical School (New Statute) W Department for PHC within the Medical Faculty
INSTITUTIONALISATION OF CME W Strategy for CME and specialisation W International Centre for studies in PHC and CME within the Medical School (New Statute) W Department for PHC within the Medical Faculty
 ACCREDITATION - LICENCING ü STRATEGY for ACCREDITATION ü AMANDMANS FOR THE HEALTH CARE LAW - delegated by the Minister of health ü DOCTORS CHAMBER STATUTE üBY-LAWS: ü By-Law for Basic Licence ü By-Law for Practicing Licence ü By-Law for Register of doctors ü By-Law for CME
ACCREDITATION - LICENCING ü STRATEGY for ACCREDITATION ü AMANDMANS FOR THE HEALTH CARE LAW - delegated by the Minister of health ü DOCTORS CHAMBER STATUTE üBY-LAWS: ü By-Law for Basic Licence ü By-Law for Practicing Licence ü By-Law for Register of doctors ü By-Law for CME
 PROJECT CLOSED IN JUNE 2002 HIGHLY SATISFACTORY CHALLENGES FOR FUTURE REFORMS
PROJECT CLOSED IN JUNE 2002 HIGHLY SATISFACTORY CHALLENGES FOR FUTURE REFORMS
 Primary Health Care - challenges üDifferent payment mechanisms in private and public PHC clinics: üDifferent motivation and limitations for private and public health providers in PHC üDifferent levels and quality of health care private üUnequal distribution of recourses
Primary Health Care - challenges üDifferent payment mechanisms in private and public PHC clinics: üDifferent motivation and limitations for private and public health providers in PHC üDifferent levels and quality of health care private üUnequal distribution of recourses
 Center for PHC and CME after the completion of the CME Project “Status quo” situation results with: ü Potential loses of the investments in the HSTP ü Discontinuity of the CME activities ü Problems with Capacity building – educators for specialisation in PHC ü Lower quality of PHC services ü Slower EU integration ü Support from the Second World Bank Project is needed
Center for PHC and CME after the completion of the CME Project “Status quo” situation results with: ü Potential loses of the investments in the HSTP ü Discontinuity of the CME activities ü Problems with Capacity building – educators for specialisation in PHC ü Lower quality of PHC services ü Slower EU integration ü Support from the Second World Bank Project is needed
 Priorities for the Health Sector Management Project ü Implementation of the contracts based on capitation for all PHC providers – private and public ü Institutional development of PHC (CME and PHC specialization) ü CME Centers – sustainability and financing of the operational costs
Priorities for the Health Sector Management Project ü Implementation of the contracts based on capitation for all PHC providers – private and public ü Institutional development of PHC (CME and PHC specialization) ü CME Centers – sustainability and financing of the operational costs
 Priorities for the Health Sector Management Project ü Support for central institution responsible for developing evidence based medicine guidelines ü Health Strategy Development – Strategy for Primary Health Care
Priorities for the Health Sector Management Project ü Support for central institution responsible for developing evidence based medicine guidelines ü Health Strategy Development – Strategy for Primary Health Care
 PHC IN FUTURE >Accessible >Well organized >Continuous >Comprehensive >Coordinated >Oriented towards: >Patient, family, community >Cost-effective
PHC IN FUTURE >Accessible >Well organized >Continuous >Comprehensive >Coordinated >Oriented towards: >Patient, family, community >Cost-effective
 WHO - Strategy Health for All in 21 Century Target 15: Integrated health system Until 2 010 people from the Region will have a much better access to the primary health care oriented towards the family and community, supported by a flexible and responsible health system.
WHO - Strategy Health for All in 21 Century Target 15: Integrated health system Until 2 010 people from the Region will have a much better access to the primary health care oriented towards the family and community, supported by a flexible and responsible health system.
 EXPECTED OUTCOMES ! Better primary health care ! Better health for all
EXPECTED OUTCOMES ! Better primary health care ! Better health for all