

450b2f06d63f35f78811833d31396052.ppt
- Количество слайдов: 20
 Readmissions: Process Improvement using the INTERACT II Tools Linda Denison Bub MSN, RN, GCNS-BC Director of Senior Health Services
Readmissions: Process Improvement using the INTERACT II Tools Linda Denison Bub MSN, RN, GCNS-BC Director of Senior Health Services
 SNF Readmissions Objectives • Describe nurses role in influencing readmissions • Explain the INTERACT tool for SNF
SNF Readmissions Objectives • Describe nurses role in influencing readmissions • Explain the INTERACT tool for SNF
 SNF Readmissions Why is this important? • Unplanned/unnecessary re-hospitalizations are prevalent and costly (Jencks et al, 2009) • Medicare: 20% in 30 days; 34% in 90 days • 50. 2% had no bill for MD visit between index admission and readmission • LOS for second stay is longer • About 10% of readmissions are planned • Cost to Medicare = $17. 4 billion (2004)
SNF Readmissions Why is this important? • Unplanned/unnecessary re-hospitalizations are prevalent and costly (Jencks et al, 2009) • Medicare: 20% in 30 days; 34% in 90 days • 50. 2% had no bill for MD visit between index admission and readmission • LOS for second stay is longer • About 10% of readmissions are planned • Cost to Medicare = $17. 4 billion (2004)
 SNF Readmission In one year nearly 30, 000 people in Wisconsin experienced a potentially preventable readmission
SNF Readmission In one year nearly 30, 000 people in Wisconsin experienced a potentially preventable readmission
 National Admissions per 1000 Beneficiaries 1/2011 -12/2011
National Admissions per 1000 Beneficiaries 1/2011 -12/2011
 National el Readmissions per 1000 Beneficiaries 1/2011 -12/2011
National el Readmissions per 1000 Beneficiaries 1/2011 -12/2011
 SNF Readmissions Wisconsin DC Dispositions • Self Care 52% • Skilled Nursing Facility 22. 7% • Home Health Care 10% • Inpatient Rehab Facility (IRF) 2. 4% • Other Hospital 2. 2% • Intermediate Care Facility (ICF) 2%
SNF Readmissions Wisconsin DC Dispositions • Self Care 52% • Skilled Nursing Facility 22. 7% • Home Health Care 10% • Inpatient Rehab Facility (IRF) 2. 4% • Other Hospital 2. 2% • Intermediate Care Facility (ICF) 2%
 SNF Readmissions Retrospective study on rehospitalization rates, diagnoses and DC location for 75+yo between 7 -30 days post DC (Hain, 2012) • 6809 patients • 12% re-hospitalization rate • SNF 15% • HH 13% • Home 8% • Conclusion: Nursing has a significant impact on re-hospitalization rates
SNF Readmissions Retrospective study on rehospitalization rates, diagnoses and DC location for 75+yo between 7 -30 days post DC (Hain, 2012) • 6809 patients • 12% re-hospitalization rate • SNF 15% • HH 13% • Home 8% • Conclusion: Nursing has a significant impact on re-hospitalization rates
 • • • 2007 -2008 Medicare") SNF Readmissions SNF 30 day readmissions (Ouslander 2011) • • • 2007 -2008 Medicare FFS beneficiaries 75 yo+ 30% DC to SNF 18% Readmitted with 30 days Of the readmissions, 1/3 readmitted in 7 days Index admission with highest readmissions • GU (30%) • CV (25%) • Readmission reasons • HF, UTI, Renal Failure, Pnuemonia/COPD
SNF Readmissions SNF 30 day readmissions (Ouslander 2011) • • • 2007 -2008 Medicare FFS beneficiaries 75 yo+ 30% DC to SNF 18% Readmitted with 30 days Of the readmissions, 1/3 readmitted in 7 days Index admission with highest readmissions • GU (30%) • CV (25%) • Readmission reasons • HF, UTI, Renal Failure, Pnuemonia/COPD
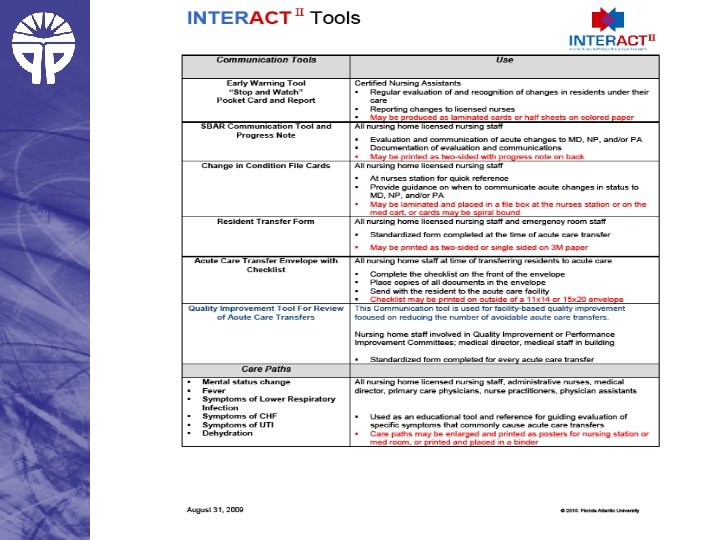
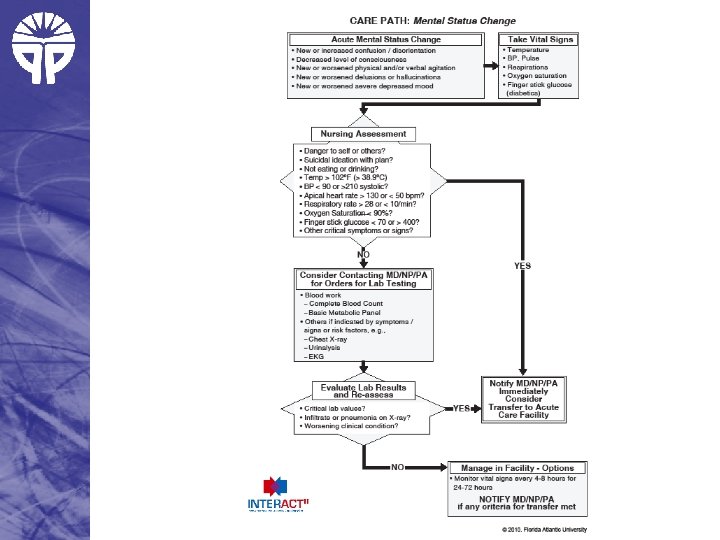
 Nursing Impact on SNF Readmissions • Acuity of SNF is increasing with SAR transfers • Nursing can impact transitions through education, protocols and collaboration • INTERACT II designed as a quality improvement intervention for SNF/LTC • reduce readmissions • improve care and outcomes
Nursing Impact on SNF Readmissions • Acuity of SNF is increasing with SAR transfers • Nursing can impact transitions through education, protocols and collaboration • INTERACT II designed as a quality improvement intervention for SNF/LTC • reduce readmissions • improve care and outcomes
 INTERACT II "Interventions to Reduce Acute Care Transfers“ (Ouslander 2011) • 25 SNF in 3 states over 6 months • Provided • • Tools (protocols) On site education for staff Teleconference every 2 weeks Facilitated by an NP
INTERACT II "Interventions to Reduce Acute Care Transfers“ (Ouslander 2011) • 25 SNF in 3 states over 6 months • Provided • • Tools (protocols) On site education for staff Teleconference every 2 weeks Facilitated by an NP
 • 17% reduction in readmissions • Fully engaged SNFs;") INTERACT II impact (Ouslander 2011) • 17% reduction in readmissions • Fully engaged SNFs; 24% reduction • Not engaged SNFs 6% • Comparison group 3% • Cost savings $7700 • Projected Medicare savings $125, 000
INTERACT II impact (Ouslander 2011) • 17% reduction in readmissions • Fully engaged SNFs; 24% reduction • Not engaged SNFs 6% • Comparison group 3% • Cost savings $7700 • Projected Medicare savings $125, 000
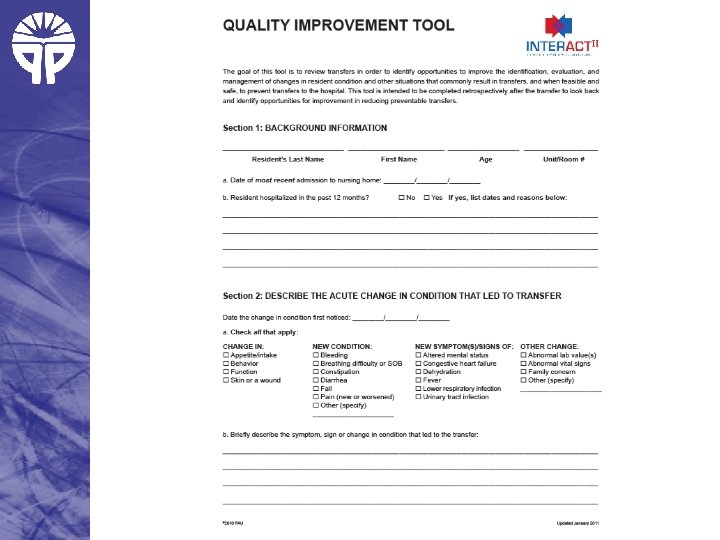
 WFH journey Initial work • October 2011 • General look at readmissions • Began identifying trends • Develop action plans (December) • January 2012 • Created word document for QI tool • Nurses responsible for filling out within 24 hours
WFH journey Initial work • October 2011 • General look at readmissions • Began identifying trends • Develop action plans (December) • January 2012 • Created word document for QI tool • Nurses responsible for filling out within 24 hours
 WFH Journey • February 2011 • Developed a goal for each facility (10% reduction from previous year average) • April 2011 • First cross sight communication • June 2011 • CNA and RN education on early warning signs of CHF • August/September 2012 • Collaborative meetings with other health systems
WFH Journey • February 2011 • Developed a goal for each facility (10% reduction from previous year average) • April 2011 • First cross sight communication • June 2011 • CNA and RN education on early warning signs of CHF • August/September 2012 • Collaborative meetings with other health systems
 WFH Journey Continued work • Identify true evaluation of readmissions • Focus on Palliative Care education for all staff • Quarterly reporting of readmissions to system workgroups • Continued communication across settings and health systems • Participation in Dr Ouslander NIH study of phase two INTERACT
WFH Journey Continued work • Identify true evaluation of readmissions • Focus on Palliative Care education for all staff • Quarterly reporting of readmissions to system workgroups • Continued communication across settings and health systems • Participation in Dr Ouslander NIH study of phase two INTERACT
 Lessons Learned • Need a champion to promote work and continue enthusiasm • Include staff from beginning • Make work meaningful, how will this impact residents • This is where care is going, leave comfort zone • Get involved in local, state and national projects
Lessons Learned • Need a champion to promote work and continue enthusiasm • Include staff from beginning • Make work meaningful, how will this impact residents • This is where care is going, leave comfort zone • Get involved in local, state and national projects
 References • Hain, D. J. , Tappen, R. , Diaz, S. , Ouslander, J. G. (2012). Characteristics of older adults rehospitalized within 7 and 30 days of discharge: implications for nursing practice. Journal of Gerontological Nursing: 38(8): 32 -44. • Jencks, S. F. , Williams, M. V. , Coleman, E. A. (2009) Rehospitalizations among Patients in the Medicare Fee-for-Service Program. New England Journal of Medicine; 360: 1418 -1428 • Ouslander, J. G. , Diaz S. , Hain, D. , Tappen R. (2011). Frequency and Diagnoses Associated With 7 - and 30 -Day Readmission of Skilled Nursing Facility Patients to a Nonteaching Community Hospital. Journal of the American Medical Director Association: 12 (3): 195 -203. • Ouslander, J. G. , Lamb, G. , Tappen, R. , Herndon L. , Diaz S. , Roos B. , Grabowski D. , Bonner A. (2011). Interventions to Reduce Hospitalizations from Nursing Homes: Evaluation of the INTERACT II Collaborative Quality Improvement Project. Journal of the American Geriatrics Society: 59(4): 745 -753.
References • Hain, D. J. , Tappen, R. , Diaz, S. , Ouslander, J. G. (2012). Characteristics of older adults rehospitalized within 7 and 30 days of discharge: implications for nursing practice. Journal of Gerontological Nursing: 38(8): 32 -44. • Jencks, S. F. , Williams, M. V. , Coleman, E. A. (2009) Rehospitalizations among Patients in the Medicare Fee-for-Service Program. New England Journal of Medicine; 360: 1418 -1428 • Ouslander, J. G. , Diaz S. , Hain, D. , Tappen R. (2011). Frequency and Diagnoses Associated With 7 - and 30 -Day Readmission of Skilled Nursing Facility Patients to a Nonteaching Community Hospital. Journal of the American Medical Director Association: 12 (3): 195 -203. • Ouslander, J. G. , Lamb, G. , Tappen, R. , Herndon L. , Diaz S. , Roos B. , Grabowski D. , Bonner A. (2011). Interventions to Reduce Hospitalizations from Nursing Homes: Evaluation of the INTERACT II Collaborative Quality Improvement Project. Journal of the American Geriatrics Society: 59(4): 745 -753.