

21d368e49ed7ecb07f1018bb46293d55.ppt
- Количество слайдов: 46
 Quality Metrics at the VA Allison Zhang M. D. Chief Medical Resident in Quality and Patient Safety
Quality Metrics at the VA Allison Zhang M. D. Chief Medical Resident in Quality and Patient Safety
 Quality Metrics at the VA 1. Anticipated Discharge 2. Clinical Pathways 3. Alcohol and Tobacco Use Assessment 4. Medication Reconciliation 5. Hospital Acquired Infections (HAI) 6. Discharge Appointments 7. Discharge Navigator 8. ACSC Related Admissions 9. Discharge Efficiency 10. Stroke Metrics
Quality Metrics at the VA 1. Anticipated Discharge 2. Clinical Pathways 3. Alcohol and Tobacco Use Assessment 4. Medication Reconciliation 5. Hospital Acquired Infections (HAI) 6. Discharge Appointments 7. Discharge Navigator 8. ACSC Related Admissions 9. Discharge Efficiency 10. Stroke Metrics
 1. Anticipated Discharge • Directly follows from Admission Template
1. Anticipated Discharge • Directly follows from Admission Template
 2. Clinical Pathways • Integrated into Admission Template and Progress Note • Two major clinical pathways: CHF and Pneumonia • Activates nursing resources dedicated to those diagnoses, streamlines care management • Can initiate on admission or during hospital stay
2. Clinical Pathways • Integrated into Admission Template and Progress Note • Two major clinical pathways: CHF and Pneumonia • Activates nursing resources dedicated to those diagnoses, streamlines care management • Can initiate on admission or during hospital stay
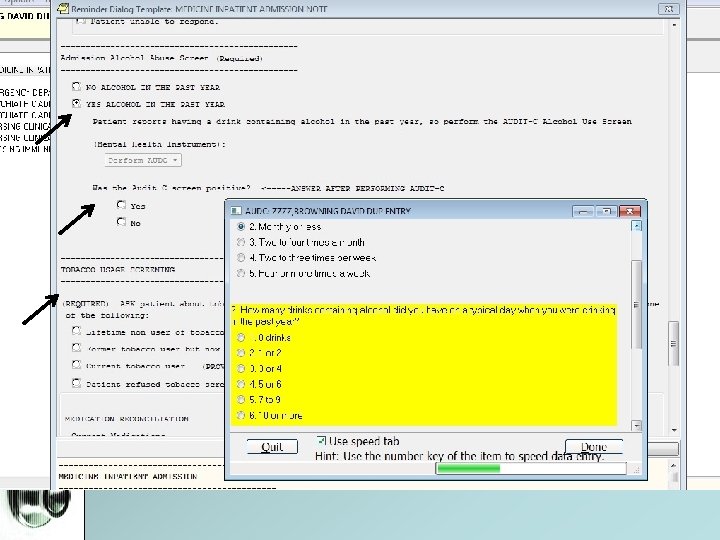
 3. Alcohol and Tobacco Use Assessment • Part of Admission Template • If positive alcohol history, must conduct AUDIT-C • If negative alcohol history, click “No Alcohol”; no AUDIT-C needed.
3. Alcohol and Tobacco Use Assessment • Part of Admission Template • If positive alcohol history, must conduct AUDIT-C • If negative alcohol history, click “No Alcohol”; no AUDIT-C needed.
 1, 2, &3 1. Anticipated Discharge 2. Clinical Pathways 3. Alcohol and Tobacco Assessment • All the above are integrated into the Admission Template • If you click through ALL check boxes and buttons (NO omission or copying and pasting), you will not miss them.
1, 2, &3 1. Anticipated Discharge 2. Clinical Pathways 3. Alcohol and Tobacco Assessment • All the above are integrated into the Admission Template • If you click through ALL check boxes and buttons (NO omission or copying and pasting), you will not miss them.
 Your documentation will be monitored for completion
Your documentation will be monitored for completion
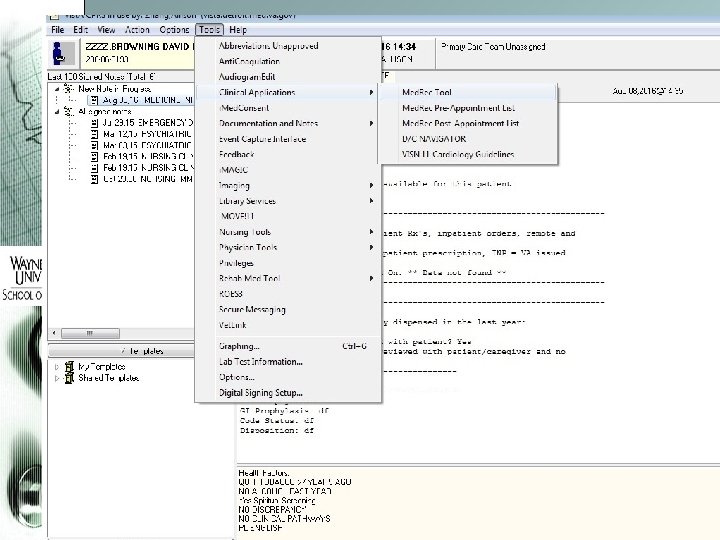
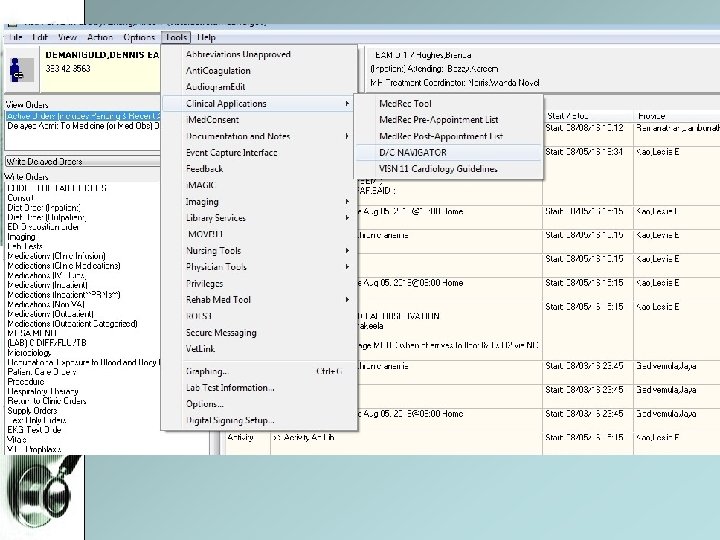
 4. Medication Reconciliation • Accessible via Clinical Applications or D/C Navigator • Essential for safe and accurate care management, and transition of care.
4. Medication Reconciliation • Accessible via Clinical Applications or D/C Navigator • Essential for safe and accurate care management, and transition of care.
 Refine your display Perform for each patient on admission
Refine your display Perform for each patient on admission
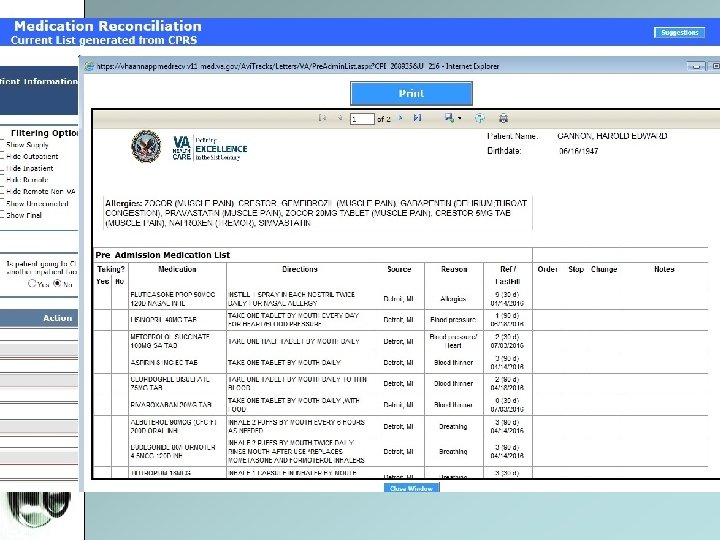
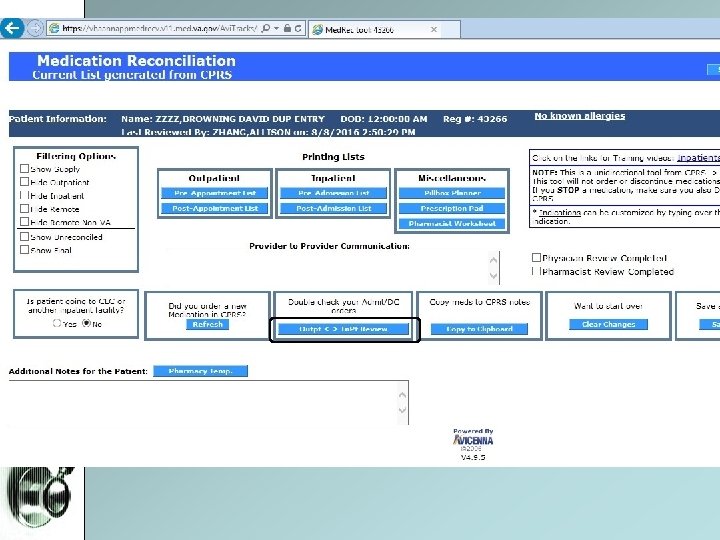
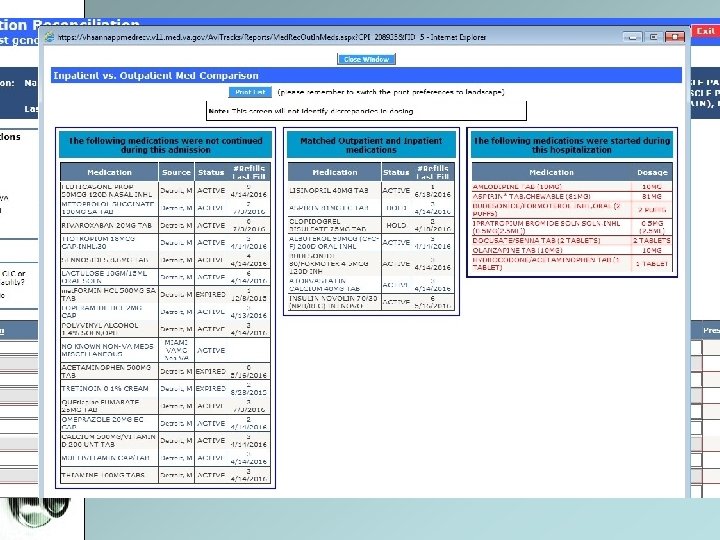
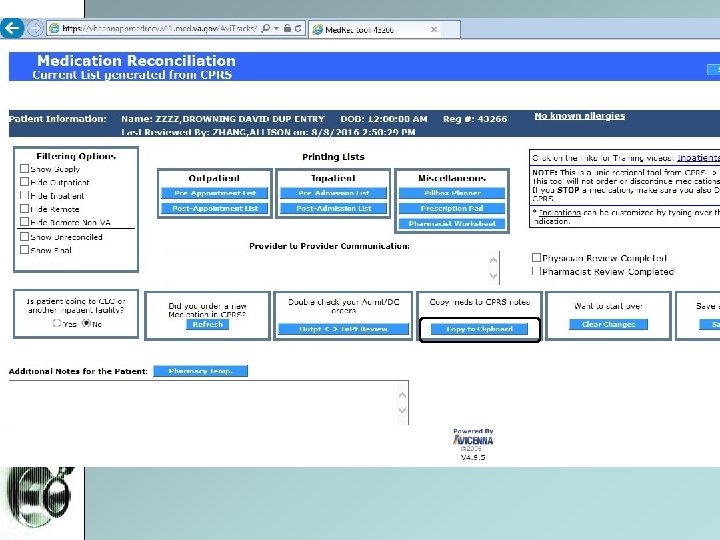
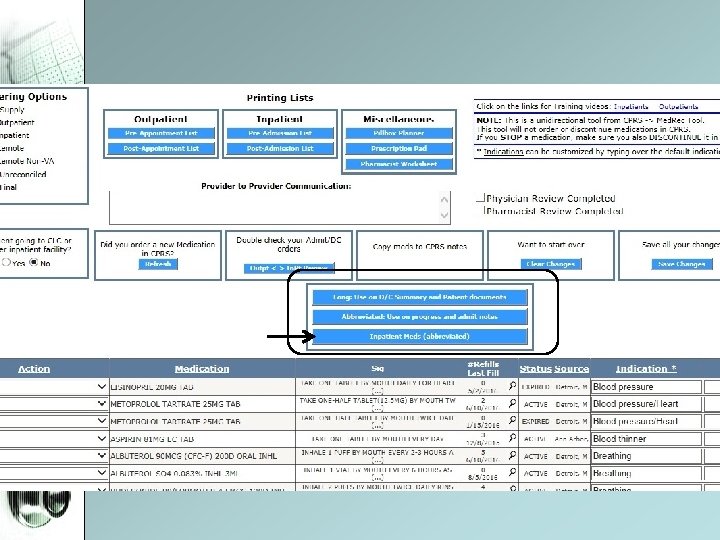
 Reconciliation and generation of discharge medication list
Reconciliation and generation of discharge medication list
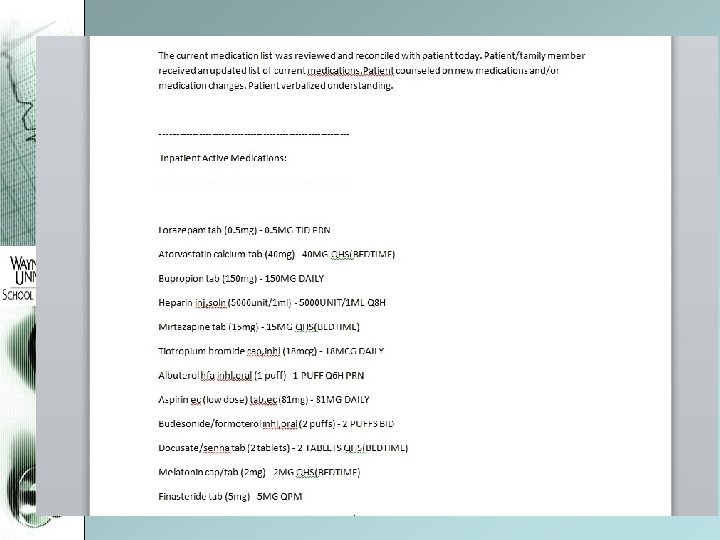
 Double click on each medication for administration history
Double click on each medication for administration history
 • C. Diff - If patient has diarrhea and") 5. Hospital Acquired Infections (HAI) • C. Diff - If patient has diarrhea and C. diff is suspected, MUST place C. Diff PCR order WITHIN 48 hours - If testing is delayed(>48 hrs), infection will be considered as hospital acquired (HAI). - Comprehensive ROS, community acquired C. diff in veterans is on the rise • CLABSI - Ensure all central lines are removed if no longer indicated (for MCIU transfers especially). • CAUTI - Remove urinary catheter if there is no indication.
5. Hospital Acquired Infections (HAI) • C. Diff - If patient has diarrhea and C. diff is suspected, MUST place C. Diff PCR order WITHIN 48 hours - If testing is delayed(>48 hrs), infection will be considered as hospital acquired (HAI). - Comprehensive ROS, community acquired C. diff in veterans is on the rise • CLABSI - Ensure all central lines are removed if no longer indicated (for MCIU transfers especially). • CAUTI - Remove urinary catheter if there is no indication.
 6. Discharge Appointments • CHF Exacerbation - One week f/u with PCP or Cardiology - Place Telehealth Consult on day of discharge • COPD Exacerbation - One week f/u with PCP or Clinical Pharmacist • PCP - If patient does not have PCP on admission, please assign one on discharge. Sign Ambulatory /Primary Care Administrative Note to Dr. Gappy. Under Return to Clinic Orders. Simply input order, MSA will take care of scheduling.
6. Discharge Appointments • CHF Exacerbation - One week f/u with PCP or Cardiology - Place Telehealth Consult on day of discharge • COPD Exacerbation - One week f/u with PCP or Clinical Pharmacist • PCP - If patient does not have PCP on admission, please assign one on discharge. Sign Ambulatory /Primary Care Administrative Note to Dr. Gappy. Under Return to Clinic Orders. Simply input order, MSA will take care of scheduling.
 1 CHF and COPD
1 CHF and COPD
 Assign PCP
Assign PCP
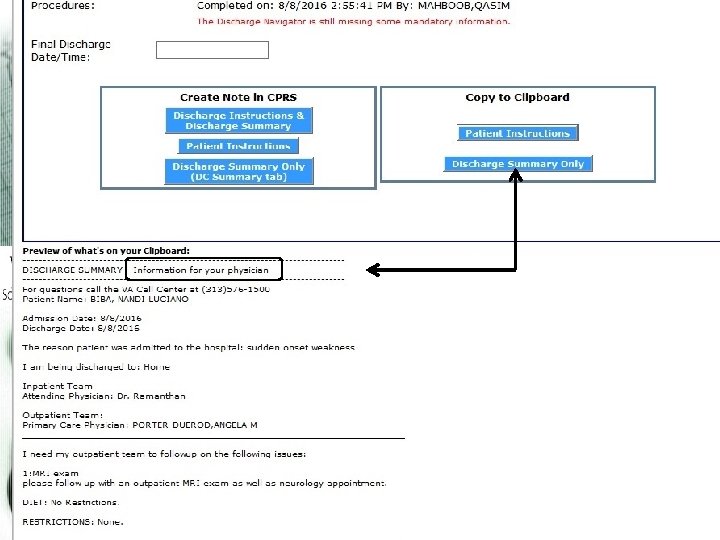
 7. Discharge Navigator • Simplify the process of D/C Summary and Note generation. • Can populate from day 1; serves as a template. • Can copy and paste Discharge Summary / Note from D/C Navigator onto blank note in CPRS • D/C Summary is for other providers to view • D/C Note is for the patient to view
7. Discharge Navigator • Simplify the process of D/C Summary and Note generation. • Can populate from day 1; serves as a template. • Can copy and paste Discharge Summary / Note from D/C Navigator onto blank note in CPRS • D/C Summary is for other providers to view • D/C Note is for the patient to view
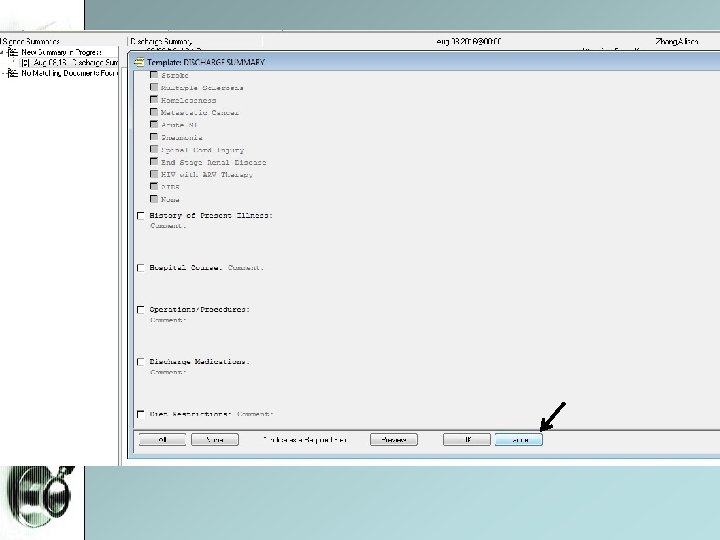
 Populate all fields under each tab. Very user-friendly and self-explanatory
Populate all fields under each tab. Very user-friendly and self-explanatory
 Discharge Note Discharge Summary
Discharge Note Discharge Summary
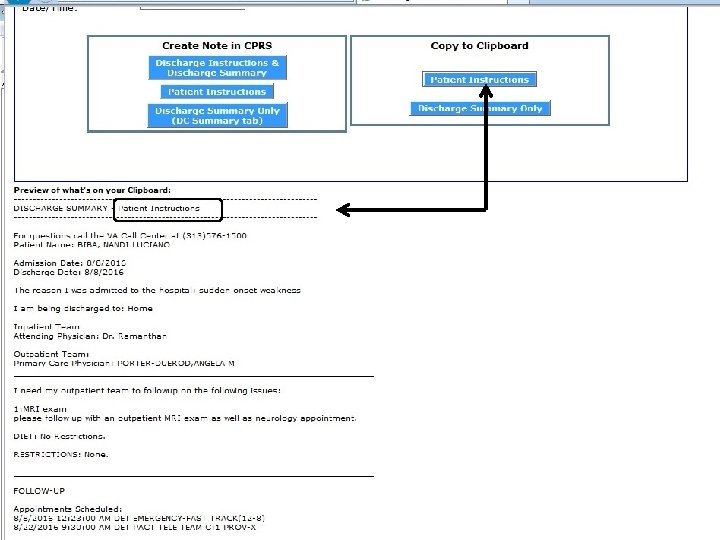
 Pasted Discharge Note
Pasted Discharge Note
 Pasted Discharge Note
Pasted Discharge Note
 are managed") 8. ACSC Related Admissions • Ambulatory Care Sensitive Conditions (ACSC, next slide) are managed on an outpatient basis • ACSC related admissions should be preventable if there is adequate outpatient care. • Such an admission negatively impacts the hospital’s reimbursement and star ratings • Many times, the primary discharge diagnosis is INCORRECTLY labeled as an ACSC • Need to be cognizant in documenting the most accurate discharge diagnosis. • Please list ONE primary D/C diagnosis, not multiple (what did you devote the most resources to? )
8. ACSC Related Admissions • Ambulatory Care Sensitive Conditions (ACSC, next slide) are managed on an outpatient basis • ACSC related admissions should be preventable if there is adequate outpatient care. • Such an admission negatively impacts the hospital’s reimbursement and star ratings • Many times, the primary discharge diagnosis is INCORRECTLY labeled as an ACSC • Need to be cognizant in documenting the most accurate discharge diagnosis. • Please list ONE primary D/C diagnosis, not multiple (what did you devote the most resources to? )
 8. ACSC Related Admissions
8. ACSC Related Admissions
 9. Discharge Efficiency • Most admissions take place between 1 -5 pm -> lumping admissions for on-call team • Early (morning) discharges facilitate patients’ allocation from ED to the floor. • The Longer patients stay in the ED, the worse their overall outcome • Discharge before 1 pm also reduces 14 day readmission rate • Goal is discharge before noon (12 PM)
9. Discharge Efficiency • Most admissions take place between 1 -5 pm -> lumping admissions for on-call team • Early (morning) discharges facilitate patients’ allocation from ED to the floor. • The Longer patients stay in the ED, the worse their overall outcome • Discharge before 1 pm also reduces 14 day readmission rate • Goal is discharge before noon (12 PM)
 • This means:") 9. Discharge Efficiency • Goal is discharge before noon (12 PM) • This means: – – – – Planning ahead ! Start planning for D/C from admission Make astute clinical decisions Know your patient’s transport needs Know the discharge destination Have medication reconciliation completed ahead of time Contact family / update patient day before discharge Seniors: pre-round with attending to OK the day discharges and place orders before formal rounds. – You have the entire morning dedicated to facilitating discharge (admission pager on NP) – Discharge order placed by 10: 00 AM so patient can be physically out by 12: 00 PM
9. Discharge Efficiency • Goal is discharge before noon (12 PM) • This means: – – – – Planning ahead ! Start planning for D/C from admission Make astute clinical decisions Know your patient’s transport needs Know the discharge destination Have medication reconciliation completed ahead of time Contact family / update patient day before discharge Seniors: pre-round with attending to OK the day discharges and place orders before formal rounds. – You have the entire morning dedicated to facilitating discharge (admission pager on NP) – Discharge order placed by 10: 00 AM so patient can be physically out by 12: 00 PM
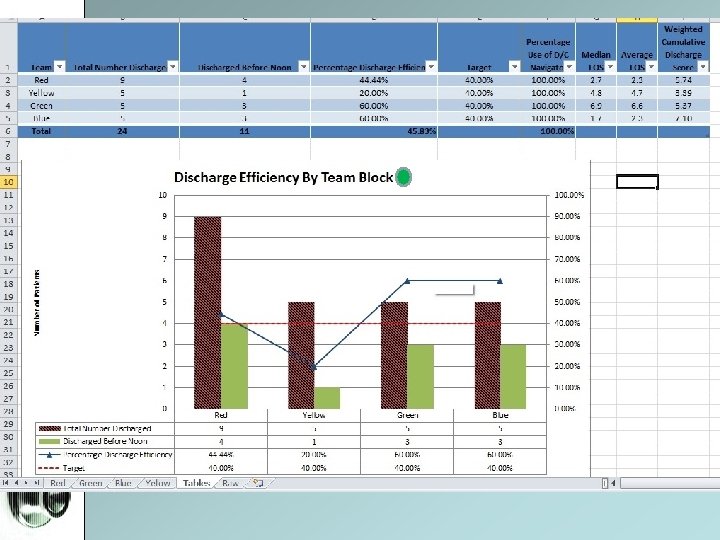
 9. Discharge Efficiency • Goal is 40% discharges before noon (meaning patient is physically off the unit by 12 pm) • Team percentages will be reported weekly via email. • Highest performing team will earn Biggby gift cards; all teams reaching 40% d/c goal will be awarded certificate of distinction from IM service • All teams will have end-of-block lunch provided.
9. Discharge Efficiency • Goal is 40% discharges before noon (meaning patient is physically off the unit by 12 pm) • Team percentages will be reported weekly via email. • Highest performing team will earn Biggby gift cards; all teams reaching 40% d/c goal will be awarded certificate of distinction from IM service • All teams will have end-of-block lunch provided.
 10. Stroke Metrics 1. 2. 3. 4. 5. VTE prophylaxis: – w/in 24 hours starting anticoag or SCDs – document reason for holding Discharged with antithrombotic therapy – ASA, warfarin, heparin, clopidogrel, ticlopidine, dabigatran, enoxaparin, fonda, zorprin. – Document reason for holding Atrial Fibrillation: – Anticoagulation prescribed at discharge – Documentation of reason for holding IV thrombolytic therapy w/in 3 hours of last known well – ED / Neuro/ ICU – Document that last known well time if > 3 hours Anti-platelets by end of hospital day 2 1. ASA, Plavix, etc given by day 2 2. Document reason for holding
10. Stroke Metrics 1. 2. 3. 4. 5. VTE prophylaxis: – w/in 24 hours starting anticoag or SCDs – document reason for holding Discharged with antithrombotic therapy – ASA, warfarin, heparin, clopidogrel, ticlopidine, dabigatran, enoxaparin, fonda, zorprin. – Document reason for holding Atrial Fibrillation: – Anticoagulation prescribed at discharge – Documentation of reason for holding IV thrombolytic therapy w/in 3 hours of last known well – ED / Neuro/ ICU – Document that last known well time if > 3 hours Anti-platelets by end of hospital day 2 1. ASA, Plavix, etc given by day 2 2. Document reason for holding
 10. Stroke Metrics 6. Statin at time of discharge. – Must document reason for holding 7. Inpatient assessment for rehab: – Must be assessed for or receive rehabilitation services during the hospitalization. 8. Stroke education: 5 components – Activation of EMS – Follow up scheduled – All d/c meds – Risk factors for stroke – Warning signs and symptoms of stroke NOTE: If stroke was ruled out, discharge diagnosis should not be RULE OUT STROKE, discharge summary should clearly state that diagnosis was ruled out.
10. Stroke Metrics 6. Statin at time of discharge. – Must document reason for holding 7. Inpatient assessment for rehab: – Must be assessed for or receive rehabilitation services during the hospitalization. 8. Stroke education: 5 components – Activation of EMS – Follow up scheduled – All d/c meds – Risk factors for stroke – Warning signs and symptoms of stroke NOTE: If stroke was ruled out, discharge diagnosis should not be RULE OUT STROKE, discharge summary should clearly state that diagnosis was ruled out.
 The End • Questions ? ? ?
The End • Questions ? ? ?