

9c83a640ae489957b9179dfe4f20a90a.ppt
- Количество слайдов: 25
 Provincial Perspectives on Data Access, Management and Linkage Stafford Dean Senior Program Officer – Analytics Research, Innovation, and Analytics Alberta Health Services May 14, 2014 1
Provincial Perspectives on Data Access, Management and Linkage Stafford Dean Senior Program Officer – Analytics Research, Innovation, and Analytics Alberta Health Services May 14, 2014 1
 Outline • What has been accomplished since the formation of AHS • What we have learned so far • Where are we going from here 2
Outline • What has been accomplished since the formation of AHS • What we have learned so far • Where are we going from here 2
 Accomplishments – Created a Data Repository • A Data Repository for Secondary Use – data that is created from delivering and managing health care is made available to be used and re-used to support quality management, performance management and research • Administrative data (DAD/NACRs) and data from various transactional source systems are integrated, conformed , and put into one provincial file. • Contains the mainstream data sets – DAD, NACRs, Physician Claims, Registry, ADT, Lab, DI MIS expenditure reporting, Continuing care, patient experience and many more. . . • Analytical data sets – existing pre-mergers of data useful for analysis 3
Accomplishments – Created a Data Repository • A Data Repository for Secondary Use – data that is created from delivering and managing health care is made available to be used and re-used to support quality management, performance management and research • Administrative data (DAD/NACRs) and data from various transactional source systems are integrated, conformed , and put into one provincial file. • Contains the mainstream data sets – DAD, NACRs, Physician Claims, Registry, ADT, Lab, DI MIS expenditure reporting, Continuing care, patient experience and many more. . . • Analytical data sets – existing pre-mergers of data useful for analysis 3
 The AHS Data Repository – The Value – Increases efficiency • Analysts spend more time doing analytics, less time chasing data • Data is ready to analyze with formal data set documentation and (meta data), formal data quality assessments • Easy to use master reference tables – Increases the value of information generated by linking data sets across systems of care – Enables report automation 4
The AHS Data Repository – The Value – Increases efficiency • Analysts spend more time doing analytics, less time chasing data • Data is ready to analyze with formal data set documentation and (meta data), formal data quality assessments • Easy to use master reference tables – Increases the value of information generated by linking data sets across systems of care – Enables report automation 4
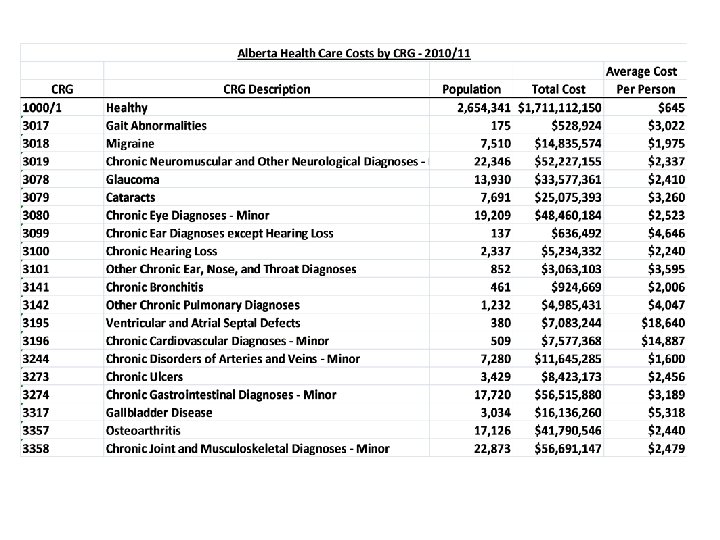
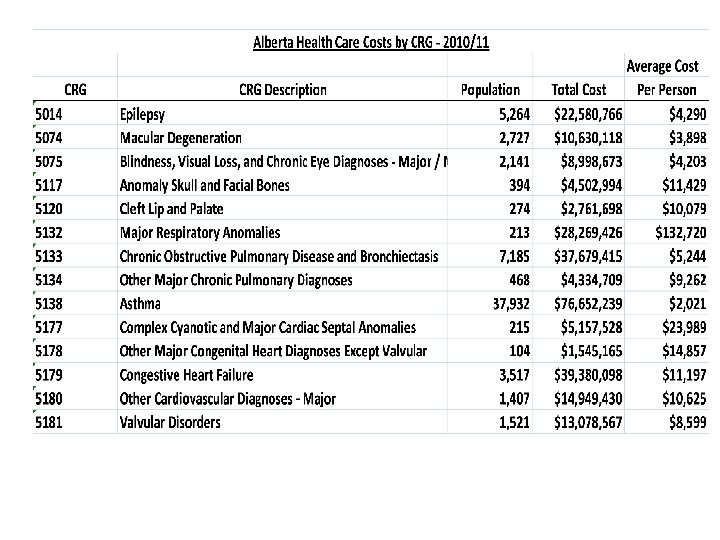
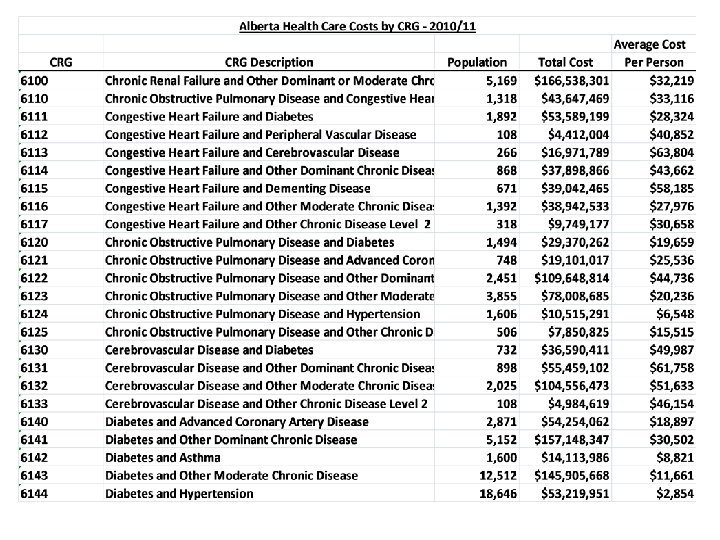
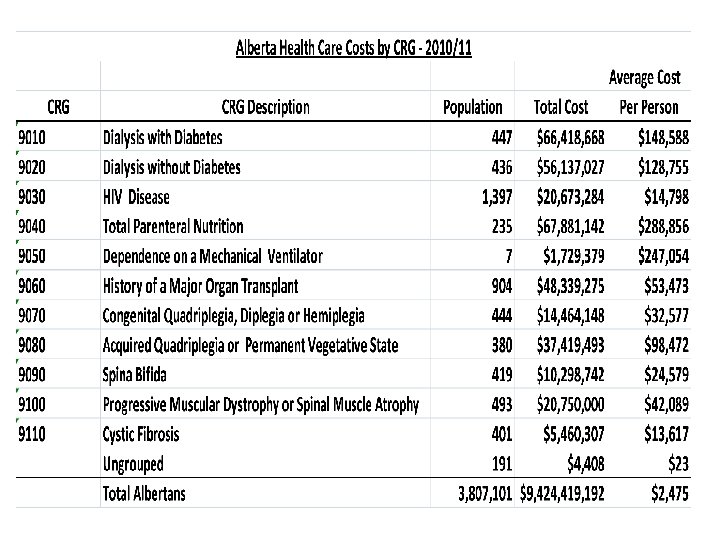
 • Data sets that are pre linked and") Analytical Data Sets (Linked Data Marts) • Data sets that are pre linked and made available to analysts for various analytic purposes: • Prevalence estimate file • Longitudinal master file • Population costing data 5
Analytical Data Sets (Linked Data Marts) • Data sets that are pre linked and made available to analysts for various analytic purposes: • Prevalence estimate file • Longitudinal master file • Population costing data 5
 • Developed a reporting environment that enables automated reporting") Accomplishments – Automated Reporting (Tableau) • Developed a reporting environment that enables automated reporting and exploratory analytics /drill downs • We started with the most common requests – re-admissions, utilization, LOS, . . . • Over 100 dashboards are now automated • We have over regular 50 tableau dashboard developers and 1, 000’s of users. • We have ‘freed’ analysts time spend on responding to adhoc requests can now address more strategic analytic needs. 10
Accomplishments – Automated Reporting (Tableau) • Developed a reporting environment that enables automated reporting and exploratory analytics /drill downs • We started with the most common requests – re-admissions, utilization, LOS, . . . • Over 100 dashboards are now automated • We have over regular 50 tableau dashboard developers and 1, 000’s of users. • We have ‘freed’ analysts time spend on responding to adhoc requests can now address more strategic analytic needs. 10
 11
11
 12
12
 13
13
 Accomplishments – Performance Reporting • We have developed standard definitions, formal public reporting process 14
Accomplishments – Performance Reporting • We have developed standard definitions, formal public reporting process 14
 Strategic Layer – Measures q Satisfaction with hospital care q Satisfaction with long term care q Hospital-acquired infections - C-Diff q Hand hygiene compliance rate q Hospital mortality rate q Early detection of cancer q Mental health readmissions q Surgery readmissions q Heart attack mortality q Stroke mortality q Emergency department wait to be seen by a physician (median) q ED length of stay - admitted (median) province's 16 busiest sites q ED length of stay - discharged (median) province's 17 busiest sites q Access to radiation therapy (90 th percentile) q Continuing care placement within 30 days q Actual length of hospital stay compared to expected stay http: //www. albertahealthservices. ca/performance. asp 15
Strategic Layer – Measures q Satisfaction with hospital care q Satisfaction with long term care q Hospital-acquired infections - C-Diff q Hand hygiene compliance rate q Hospital mortality rate q Early detection of cancer q Mental health readmissions q Surgery readmissions q Heart attack mortality q Stroke mortality q Emergency department wait to be seen by a physician (median) q ED length of stay - admitted (median) province's 16 busiest sites q ED length of stay - discharged (median) province's 17 busiest sites q Access to radiation therapy (90 th percentile) q Continuing care placement within 30 days q Actual length of hospital stay compared to expected stay http: //www. albertahealthservices. ca/performance. asp 15
 Progress made so far – data sharing • • Developed a shared data model program that develops relationships and facilitates data sharing among distributed analytic teams in AHS. Start with an analytic or reporting need that important to the particular area The data that is needed to address the need is not currently accessible to the distributed analytic/data team Work together in a formal way to develop the analytic product Develops relationships between DIMR analysts and the distributed analysts Distributed teams learn about data holdings in the repository and we learn about data holdings in the distributed teams Win - win – the potential value by working together is greater than working in isolation. 16
Progress made so far – data sharing • • Developed a shared data model program that develops relationships and facilitates data sharing among distributed analytic teams in AHS. Start with an analytic or reporting need that important to the particular area The data that is needed to address the need is not currently accessible to the distributed analytic/data team Work together in a formal way to develop the analytic product Develops relationships between DIMR analysts and the distributed analysts Distributed teams learn about data holdings in the repository and we learn about data holdings in the distributed teams Win - win – the potential value by working together is greater than working in isolation. 16
 The shared data model accommodates both enterprise and departmental data is a key roadmap enabler Cancer Care Repository Perinatal Population Health Operating Room Critical Care Personally identifiable data Cardiac Care Alberta Data Repository /DIMR Zone data Trauma Seniors Emergency Department Mental Health The Open Data Model has… § § § A centrally managed core Controlled access to personally identifiable data Distributed departmental / subject-area databases that can link with the core Robust master data and identifier keys that link central and departmental / subject-area data Open Data Model Privacy and Anonymization are foundational issues that must resolved early 17 in the Roadmap
The shared data model accommodates both enterprise and departmental data is a key roadmap enabler Cancer Care Repository Perinatal Population Health Operating Room Critical Care Personally identifiable data Cardiac Care Alberta Data Repository /DIMR Zone data Trauma Seniors Emergency Department Mental Health The Open Data Model has… § § § A centrally managed core Controlled access to personally identifiable data Distributed departmental / subject-area databases that can link with the core Robust master data and identifier keys that link central and departmental / subject-area data Open Data Model Privacy and Anonymization are foundational issues that must resolved early 17 in the Roadmap
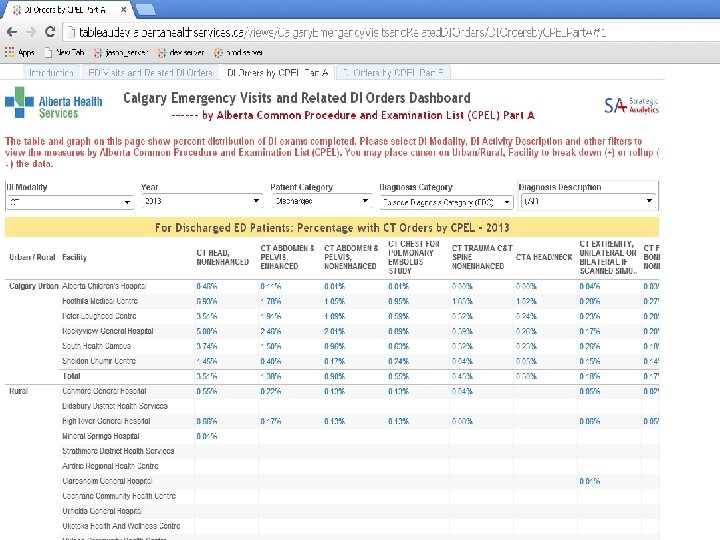
 Progress made so far – DI Example • What is the DI utilization relative to the number of ED visits what is that utilization relative to discharge diagnosis across Alberta? • What is the DI utilization relative to presenting complaint across Alberta? 18
Progress made so far – DI Example • What is the DI utilization relative to the number of ED visits what is that utilization relative to discharge diagnosis across Alberta? • What is the DI utilization relative to presenting complaint across Alberta? 18
 20
20
 Progress made so far – Access for research • Developed a process to enable access for investigator initiated research • Use a research agreement • Have a team (3) of dedicated talented analysts that act as the interface between the research community and AHS data assets 21
Progress made so far – Access for research • Developed a process to enable access for investigator initiated research • Use a research agreement • Have a team (3) of dedicated talented analysts that act as the interface between the research community and AHS data assets 21
 What we have learned so far • Shared data model is an attractive way to connect analytic teams • Adaptive data warehouse – staged levels of data access and late binding – bring all the data in with limited context or transformation (raw data materials) then make the data available in raw form up to very structured data • Analytics is different than traditional BI • Fully functioning Data Scientists are rare. We need to create more folks like these • Making sure secondary use of data is planned up front and is a requirement in any info system investments 22
What we have learned so far • Shared data model is an attractive way to connect analytic teams • Adaptive data warehouse – staged levels of data access and late binding – bring all the data in with limited context or transformation (raw data materials) then make the data available in raw form up to very structured data • Analytics is different than traditional BI • Fully functioning Data Scientists are rare. We need to create more folks like these • Making sure secondary use of data is planned up front and is a requirement in any info system investments 22
 What we have learned so far • Secondary use of EMR/EHR data is the key to truly be able to mange clinical service performance • We have limited experience in using EMR data – pockets exist, but generally very little. • EMR/EHR data is very complex • Trust the analysts. Allow access, let them be creative and do not use restriction as a means to minimize risk. Manage what is produced not just what is accessed. • Produce analytical products and reports with the data you have. It starts the discussion and makes the conversations meaningful. 23
What we have learned so far • Secondary use of EMR/EHR data is the key to truly be able to mange clinical service performance • We have limited experience in using EMR data – pockets exist, but generally very little. • EMR/EHR data is very complex • Trust the analysts. Allow access, let them be creative and do not use restriction as a means to minimize risk. Manage what is produced not just what is accessed. • Produce analytical products and reports with the data you have. It starts the discussion and makes the conversations meaningful. 23
 What we have learned so far • Data integration is easier than systems integration • Not everything needs to be real time • Getting an actual decision is tough, even when the data is available and it is obvious what is needed to happen. We need to build a data driven culture. 24
What we have learned so far • Data integration is easier than systems integration • Not everything needs to be real time • Getting an actual decision is tough, even when the data is available and it is obvious what is needed to happen. We need to build a data driven culture. 24
 Where are we going from here • • Focus on clinical data - need to further develop this capability Focus on outcome data – PROMs and disease specific clinical outcomes Focus on HR and cost data Bring these together so we can truly analyze relationships between clinical process, cost and outcomes Enable measurement from the bottom up – measuring at a meaningful level for our front line providers by developing balanced measurement sets across the domains of quality for specific clinical populations. Enable providers to see how they perform relative to there peers and relative to best practice. Accelerate de- identification to improve access to data • Leverage what AHS has done so far for other bigger initiatives such as PHAN 25
Where are we going from here • • Focus on clinical data - need to further develop this capability Focus on outcome data – PROMs and disease specific clinical outcomes Focus on HR and cost data Bring these together so we can truly analyze relationships between clinical process, cost and outcomes Enable measurement from the bottom up – measuring at a meaningful level for our front line providers by developing balanced measurement sets across the domains of quality for specific clinical populations. Enable providers to see how they perform relative to there peers and relative to best practice. Accelerate de- identification to improve access to data • Leverage what AHS has done so far for other bigger initiatives such as PHAN 25