b5eea7aa42ff56a466a6f7b6bebc0ef5.ppt
- Количество слайдов: 118



Proposed Alaska Children’s Behavioral Health System of Care Submitted by: OPEN MINDS November 16, 2009 Dan M. Aune, Senior Consultant

Children’s Behavioral Health System of Care Outline I. III. IV. V. VI. VII. 2 VIII. Executive Summary Background of Alaska System of Care Initiative Current Child and Youth Service System Project Methodology Coordinated & Sequenced Transition Plan to the Proposed Alaska Children’s Behavioral Health System of Care Sources of Funding Methods Outcome Measure Recommendations Sustaining the Proposed Alaska SOC OPEN MINDS © 2009. All rights reserved.

I. Executive Summary 3 OPEN MINDS © 2009. All rights reserved.

The Goal A behavioral health services system that would be functional as welcoming, accessible, integrated, comprehensive and continuous at a client/consumer, clinician, program, and system level. 4 OPEN MINDS © 2009. All rights reserved.

Key Findings 1. Alaska has a demonstrated history of: ü commitment and creativity in providing services for children, youth, and families ü funding a service system with a multitude of funding entities (e. g. federal, state general funds, Indian Health Services, private grants). ü addressing the issues of children placed out-of-state through the Bring The Kids Home initiative (BTKH) 5 OPEN MINDS © 2009. All rights reserved.
 One result of BTKH in bringing children and youth back")
Key Findings (Cont. ) One result of BTKH in bringing children and youth back to Alaska has been the development of residential service facilities beyond the current placement demands 3. The Joint Management Team (JMT) is actively: 2. ü Involved in working on the children’s service system ü Advocating for the Behavioral Rehabilitation Services (BRS) to be moved from the Office of Children’s Services (OCS) to the Division of Behavior Health (DBH)
 4. OCS currently provides the Medicaid billing for the providers")
Key Findings (Cont. ) 4. OCS currently provides the Medicaid billing for the providers 5. The Division of Behavioral Health initiated the Alaska Automated Information Management System (AKIMS) was initiated in 2003 and continues to move toward integration of clinical and billing medical record system
 6. The Division of Juvenile Justice, Office of Children’s Services,")
Key Findings (Cont. ) 6. The Division of Juvenile Justice, Office of Children’s Services, and Senior Disabilities Services Division all have information management systems different from AKIMS and are in the process of working with DBH to provide for some inter-operability between information management systems. 7. Workforce development continues to be a critical factor for providers of services within the SOC

Recommendations 1. 2. 3. 4. 5. 9 Accept the proposed Alaska SOC model which has a heavy emphasis on service development in the community or village Develop a universal care plan model for children and youth (treatment plans, LOC instrument assessments, progress reports, crisis plans, and community resources) Adopt the behavioral health treatment model as the center of the planning efforts for the SOC Accept DBH as the division managing the proposed Alaska SOC Adopt the Education/Training Plan OPEN MINDS © 2009. All rights reserved.
 6. 7. 8. 10 Develop the proposed Alaska SOC framework of")
Recommendations (Cont. ) 6. 7. 8. 10 Develop the proposed Alaska SOC framework of stakeholders (Local Advisory Councils on Children’s Services, State Collaborative, DBH as SOC manager, Policy Performa Group, Family Teams, and Children/Youth/Families) Develop structure and the flow of accountability for all groups (LACs, State Collaborative, DBH, PPG, and Children, Youth and Families) within the proposed framework Develop a strong case management model to lead the Family Teams of the proposed framework OPEN MINDS © 2009. All rights reserved.
 Accept the transfer of BRS from OCS to DBH 10. Determine")
Recommendations (Cont. ) Accept the transfer of BRS from OCS to DBH 10. Determine the Level of Care instrument that best meets the needs of the proposed Alaska SOC 11. Develop relationships with providers to ensure rewards for providers achieving outcomes, increase creativity in meeting new service needs within the SOC, and developing accountability in the care of children, youth, and families 12. Initiate an informed development of evidence-based practices (EBP) group 9. 11 OPEN MINDS © 2009. All rights reserved.
 Adopt strategies for financing the proposed Alaska SOC: 13. ü Set")
Recommendations (Cont. ) Adopt strategies for financing the proposed Alaska SOC: 13. ü Set up an extensive provider network with performance based contracts ü Implement shared-risk contracts between the state of Alaska and Grantees with a focus on flexibility, creative collaboration, and risk management in regards to immediate needs of the SOC ü Implement a model ‘one care plan’ model that is coordinated through a single accountable entity
 14. Adopt strategies for financing the proposed Alaska SOC (cont. ):")
Recommendations (Cont. ) 14. Adopt strategies for financing the proposed Alaska SOC (cont. ): ü Establish a blended or braided model of funding or a combination of both ü Establish a SOC planning team made up of DBH, OCS, & DJJ to provide oversight of funding for the SOC
 15. The Policy Performa Group and State Collaborative need to go")
Recommendations (Cont. ) 15. The Policy Performa Group and State Collaborative need to go beyond memoranda of agreement among child-serving agencies at the State and be put into State of Alaska statute to ensure the roles, accountability and authority of each group are clearly specified
 16. Develop a central case or care manager for each case")
Recommendations (Cont. ) 16. Develop a central case or care manager for each case to provide continuity in decision making and offer each child, youth and family a key contact person in the Family Teams to the SOC 17. Strengthen organizational partnerships across traditional child-serving service sectors 18. Make use of key system stabilizers such as relationships with community and family organizations
 19. Support Care Coordination Functions as essential to the SOC ü")
Recommendations (Cont. ) 19. Support Care Coordination Functions as essential to the SOC ü Case load limitations ü Administrative support ü Statewide training • • • 20. Introduction to case management Case management supervision Advanced case management strategies Establish twice a year meetings to review and assess the progress in the implementation of the proposed Alaska SOC through DBH and the Policy Performa Group
 21. Invest in community voice and buy-in through the development of")
Recommendations (Cont. ) 21. Invest in community voice and buy-in through the development of Local Advisory Councils on Children’s Services in communities and villages across Alaska. Develop this model in the form of a state statute to ensure the model has a state and SOC value that is reported on in the Legislative process.
 22. Establish a cross-division training initiative which encourages and promotes understanding")
Recommendations (Cont. ) 22. Establish a cross-division training initiative which encourages and promotes understanding of the goals of the divisions under DHSS, the funding models utilized to support service delivery, and develop potential future leadership for DHSS and the SOC 23. Enhance the utilization of AK-AIMs throughout the proposed Alaska SOC. Mobilize the clinical and financial components to AK-AIMs to establish a data driven decision-making SOC 24. Continue to sponsor the Change Agent Conferences for SOC stakeholders to promote the SOC and enhance the effectiveness of the SOC

II. Background of Alaska System of Care Initiative 19 OPEN MINDS © 2009. All rights reserved.

History of Children’s System Initiatives Alaska Youth Initiative Established in the mid 1980’s § Improve care to Alaska children, youth, and family system of care by: ü providing community-based care ü individualized services to children and youth who would otherwise be institutionalized outside the state § By 1990 the initiative had developed into: ü full service delivery model with a philosophy dependent on individualized or wraparound services 20 OPEN MINDS © 2009. All rights reserved.
 Bring The Kids Home - Established in")
History of Children’s System Initiatives (Cont. ) Bring The Kids Home - Established in 2004 § Sponsored by the DHSS in partnership with the Alaska Mental Health Trust Authority (AMHTA), the Denali Commission and other stakeholders § Mission is to return children being served in out-of-state facilities back to in-state residential or community-based care § Goals of BTKH: ü Build/develop and sustain the community-based and residential capacity ü Develop an integrated, seamless service system in Alaska ü Reduce the existing numbers of children and youth in out-of-state care 21 OPEN MINDS © 2009. All rights reserved.
 Figure One. Timeline: Alaska System of Care")
History of Children’s System Initiatives (Cont. ) Figure One. Timeline: Alaska System of Care Development 1985 § 1991 § 1993 § 2002 § 2003 § 2005 § § 2008 § 2009 Alaska Youth Initiative (AYI) begins AYI ends Alaska became eligible for Medicaid funding Children and Youth Needs Assessment (CAYNA) introduced Bring The Kids Home initiated Alaska Partnership for Health Communities: Governance & Financing White Paper Alaska Children's Policy Work Group recommendation for SOC development SOC RFIP solicitation by DHSS - DBH

III. Current Child and Youth Service System 23 OPEN MINDS © 2009. All rights reserved.

A. Alaska in Context Alaska is the largest state in the United States in terms of land area at 570, 380 square miles (1, 477, 300 km²), over twice as large as Texas, the next largest state. § Alaska’s estimated 2008 population is 686, 293 people, with 7. 5% under the age of five years and 26. 7% under the age of 18 years § The racial/ethnic composition of Alaska is: § ü Caucasian 70. 8% ü American Indian and Alaska Native (AIAN) 15. 2% ü African American 4. 1% ü Asian 4. 6% ü Native Hawaiian and Other Pacific Islander 0. 6% ü Persons of Hispanic or Latino origin 5. 9% *(U. S. Census Bureau, 2000) 24 OPEN MINDS © 2009. All rights reserved.

B. Alaska System of Care Partners § Department of Health and Social Services – Division of Behavioral Health (Project Lead Division) § Division of Juvenile Justice § Office of Children’s Services § Senior Disabilities Services Division § Joint Management Team ü Senior leadership of OCS, SDSD, DJJ, & DBH ü Established to maintain a collaborative decision-making process in support of staff who are working to create a cohesive, smoothly operating system of care for children in Alaska ü Charged with oversight in the redesign of the current levels of care into a seamless system of care 25 OPEN MINDS © 2009. All rights reserved.
 § § §")
B. Alaska System of Care Partners External Stakeholder Advisory Group (ESAG) § § § DHSS / Juvenile Justice Department of Corrections Alaska Mental Health Board Alaska Board of Alcohol and Drug Addiction The Alaska Mental Health Trust Authority Grantee Organizations (Representative of the four DBH Regions and Funded Services) Alaska Behavioral Health Association Substance Abuse Directors Association National Alliance on Mental Illness Alaska Native Tribal Health Consortium University of Alaska
 Division of Behavioral Health § DBH")
B. Alaska System of Care Partners (cont. ) Division of Behavioral Health § DBH is responsible for the State's public behavioral health programs. § DBH administers the statewide system of community mental health programs for: ü Delivery of residential and community-based treatment and recovery services ü Manages the state's only public psychiatric hospital ü Administers grants to the state's network of local community mental health programs (Grantees) ü Coordinates with other government, tribal, and private providers of mental health services to ensure the provision of comprehensive mental health services to Alaska residents. 27 OPEN MINDS © 2009. All rights reserved.
 DBH Grantee breakdown by region: Anchorage")
B. Alaska System of Care Partners (cont. ) DBH Grantee breakdown by region: Anchorage region – 25 Grantees (17 treatment, 8 early intervention) § Northern region – 32 Grantees (16 treatment, 16 early intervention) § South central region – 34 Grantees (22 treatment, 12 early intervention) § Southeast region – 27 Grantees (20 treatment, 7 early intervention) § 28 OPEN MINDS © 2009. All rights reserved.
 Division of Juvenile Justice § DJJ")
B. Alaska System of Care Partners (cont. ) Division of Juvenile Justice § DJJ is responsible for: ü Holding juvenile offenders accountable for their behaviors ü Promoting the safety and restoration of victims and communities ü Assisting offenders and their families in developing skills to prevent crime. DJJ mission is based on the “restorative justice” model § DJJ also works to prevent crime by supporting competency and skill development for offenders so they have alternatives to law-breaking behavior § DJJ has sixteen field offices and eight youth facilities, divided into four geographical management areas (Anchorage, Northern, Southcentral, and Southeast Alaska) § 29 OPEN MINDS © 2009. All rights reserved.
 Office of Children’s Services § OCS")
B. Alaska System of Care Partners (cont. ) Office of Children’s Services § OCS has four broad goals for children 0 – 18 years: 1. 2. 3. 4. 30 Cultural Continuity for Children Permanency for Children Child Safety Child and Family Well-being OPEN MINDS © 2009. All rights reserved.
 Senior and Disabilities Services Division §")
B. Alaska System of Care Partners (cont. ) Senior and Disabilities Services Division § SDSD promotes: ü Personal dignity and respect ü Provides an opportunity for individuals to receive services that further their physical, mental, spiritual and emotional health § 31 Children within the SOC that SDSD would serve include those children with developmental disabilities and those challenged with physical and emotional disabilities OPEN MINDS © 2009. All rights reserved.

C. Current Alaska System of Care Medicaid Based § Alaska SOC has a focus of serving children and youth who are Medicaid eligible, meaning they fit the diagnosis for seriously emotionally disturbed (SED) § DHSS made a strategic policy shift to: ü Increase utilization of Medicaid funding ü Re-mobilize the general fund dollars to create new programs ü Enhance the SOC development ü Create a flexible funding stream for programs like the Individualized Service Agreements (ISA) 32 OPEN MINDS © 2009. All rights reserved.
 Core Values § § Community-based §")
C. Current Alaska System of Care (cont. ) Core Values § § Community-based § 33 Child centered and family focused Culturally and linguistically competent OPEN MINDS © 2009. All rights reserved.
 Guiding Principles: 1. 2. Strengthen families")
C. Current Alaska System of Care (cont. ) Guiding Principles: 1. 2. Strengthen families first (strength based, preventative) 3. Families and youth are equal partners (family driven, youth driven) 4. 34 Kids belong in their homes (least restrictive, most appropriate setting, community based) Help is accessible (coordinated and collaborative) OPEN MINDS © 2009. All rights reserved.
 Guiding Principles: 5. 6. Consumers are")
C. Current Alaska System of Care (cont. ) Guiding Principles: 5. 6. Consumers are satisfied and collaborative meaningful outcomes are achieved (emphasis on research, evidence, quality improvement, accountability) 7. 35 Normalize the situation (meet the child where they are, respect normal life cycles, promote normal and healthy development Respect individual, family and community values (culturally competent, individualized care, communityspecific solutions) OPEN MINDS © 2009. All rights reserved.
 Out-of-state residential placements Office of Children’s")
C. Current Alaska System of Care (cont. ) Out-of-state residential placements Office of Children’s Services Division of Juvenile Justice Education Grantees Current Alaska DHSS Children’s SOC Alaska Native & American Indian Corporations Key Informant SOC Stakeholders Children, Youth, Families & Advocates Senior & Disabilities Services Division of Behavioral Health
 Current System Roadblocks § Intra-division fragmentation")
C. Current Alaska System of Care (cont. ) Current System Roadblocks § Intra-division fragmentation § Failure to address children and youth outside the SED diagnostic population § Lack of the ability to use ‘cross-division’ resources

D. 2009 System of Care Initiative Why develop a SOC? § § § Meet the demands of the children, youth, and families seeking services in Alaska Develop a delivery system that is efficient and maximizes DHSS division’s resources Create a comprehensive system with an emphasis on services being provided in the community/village Emphasis wellness and prevention in orientation to more intense levels of service Utilize an array of financing Develop a system that is coordinated, responsive, and creative

IV. System of Care Development Methodology 39 OPEN MINDS © 2009. All rights reserved.

A. Project Activities § § § 40 A structured process for planning, prioritizing, and documenting the progress of the coordinated, sequenced transition plan for a children’s system of care initiative activities. A multimodal, redundant communication and information sharing process with convenient access for JMT, key informant stakeholder groups, and work groups. Use of the OPEN MINDS team’s extensive knowledge of, and experience with, a range of state children’s services and funding sources – at both the state policy level and at the community level – for early identification of both problems for resolution and opportunities for service delivery synergy. OPEN MINDS © 2009. All rights reserved.

A. Project Activities Project Deliverables Deliverable One Deliverable Two Deliverable Three Joint Management Meetings Communication Plan Deliverable Four Project Plan Deliverable Five System of Care Model Deliverable Six Stakeholder Workgroups Deliverable Seven Education and Training Plan Deliverable Eight 41 Initial Work Plan Final Report OPEN MINDS © 2009. All rights reserved. Team

V. Coordinated and Sequenced Transition Plan for a New Alaska Behavioral Health System of Care for Children “First comes thought; then organization of that thought, into ideas and plans; then transformation of those plans into reality. The beginning, as you will observe, is in your imagination. ” Napoleon Hill 42 OPEN MINDS © 2009. All rights reserved.

A. The Framework of the Proposed Alaska System of Care Local Advisory Councils of Children’s Services State Collaborative Division of Behavioral Health Policy Performa Group Family Teams Children, Youth, & Families 43 OPEN MINDS © 2009. All rights reserved.
 Local Advisory")
A. The Framework of the Proposed Alaska System of Care (cont. ) Local Advisory Councils on Children’s Services § Members are consumers (children, youth, and families), providers, advocates, and government (local and state) officials § Responsible for identifying the system needs and resources at the local level and communicating this to the State Collaborative and DBH § LAC will hold regular monthly meetings and have a representative at the State Collaborative meetings
 State Collaborative")
A. The Framework of the Proposed Alaska System of Care (cont. ) State Collaborative § § Responsible for communicating system needs and resources from the LACs and from the greater Grantee stakeholders to DBH § 45 Members are external stakeholders of the SOC, including Grantees, advocates, children, youth and families State Collaborative will hold regular monthly meetings and invite DHSS divisions to attend and be on the regular agenda OPEN MINDS © 2009. All rights reserved.
 Division of")
A. The Framework of the Proposed Alaska System of Care (cont. ) Division of Behavioral Health § § 46 Responsible for the governance of the SOC and overseeing the roles and operations of the participating DHSS divisions Ensure the development or promotion of the range of services within the five levels of the SOC Participate in the State Collaborative and when available the LAC meetings Enlist both the State Collaborative and the LACs to assist in evaluating the SOC, identifying local needs, and in the development of new services within the SOC. OPEN MINDS © 2009. All rights reserved.
 Policy Performa")
A. The Framework of the Proposed Alaska System of Care (cont. ) Policy Performa Group § § Modeled after the current Joint Management Team (JMT) § Purpose of this group will be to resolve system issues that develop in the operation of the SOC § 47 Members are made up of key leadership from DBH, DJJ, and OCS PPG will meet bi-weekly and include key leaders from DBH in an effort to work through points of accountability for the SOC and the DHSS divisions OPEN MINDS © 2009. All rights reserved.
 Family Team")
A. The Framework of the Proposed Alaska System of Care (cont. ) Family Team Name emulates the vision of the SOC § Members are made up of the child or youth family, DHSS division staff, advocates, and providers in the SOC § Family Team makes decisions about the level of care most appropriate for a child, youth, and their families § Meet initially when a child enters the SOC and then quarterly to review the status of the child or youth and determine the needed resources in the SOC to meet the needs of the child or youth most effectively §
 Family Team")
A. The Framework of the Proposed Alaska System of Care (cont. ) Family Team § Meet more frequently for children or youth that are involved in level five services in the SOC § Case manager on the Family Team is responsible to coordinate the meetings, coordinate and monitor services provided, and advocate for the needs of the child, youth, and family
 Children, Youth,")
A. The Framework of the Proposed Alaska System of Care (cont. ) Children, Youth, & Families § Foundation of the SOC is the children, youth, and families the SOC is designed to serve § Children and families have multiple paths to participate in and impact the SOC, including the Family Teams, State Collaborative, and the LACs

B. The Infrastructure of the Proposed Alaska System of Care Vision § Creating a comprehensive sustainable continuum of family centered care through efficient and effective partnerships with children, youth, and families Core Values Child-centered and family-focused care § Community-based decision-making § Culturally and linguistically competent §
 Guiding Principles")
B. The Infrastructure of the Proposed Alaska System of Care (cont. ) Guiding Principles § § § Kids belong in their homes (least restrictive, most appropriate setting, community based) Strengthen families first (strength based, preventative) Families and youth are equal partners (family driven, youth driven); Normalize the situation (meet the child where they are, respect normal life cycles, promote normal and healthy development Help is accessible (coordinated and collaborative) Consumers are satisfied and collaborative meaningful outcomes are achieved (emphasis on research, evidence, quality improvement, accountability) Respect individual, family and community values (culturally competent, individualized care, community-specific solutions)
 Level One:")
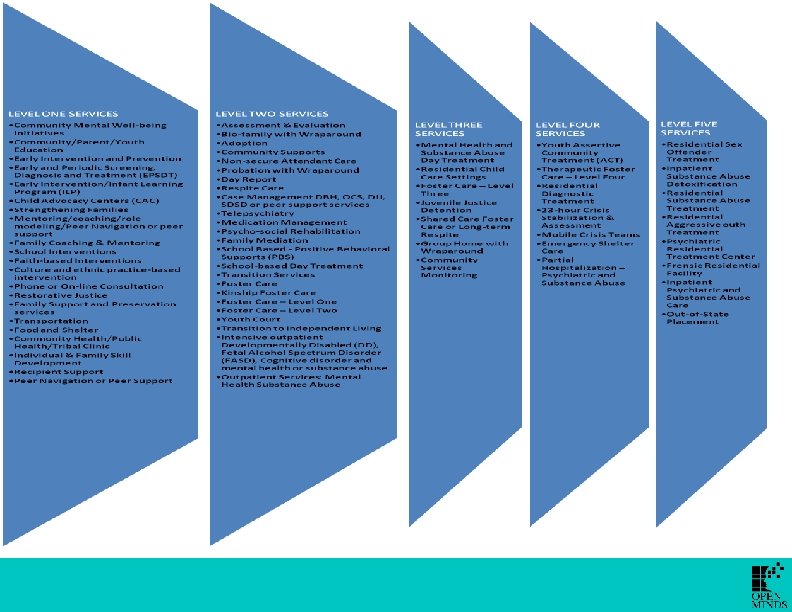
B. The Infrastructure of the Proposed Alaska System of Care (cont. ) Level One: Recovery, Maintenance, & Health Management § Community and family. Services provide wellness, prevention, and follow-up care to mobilize family strengths and reinforce linkages to natural supports. Those appropriate for this level may be either substantially recovered from an emotional disorder or service needs require minimal system involvement and are manageable within the consumer’s family and community.

Level One - Sample Service Community Mental Wellbeing Initiatives Service Definition Community mental well-being initiatives involve any action taken to enhance the mental well-being of individuals, families, organizations, and communities. These actions work to prevent mental health problems and aim to reduce the stigma associated with mental illness. Effective mental health promotion always presupposes respect for consumers, their rights, and their recovery. Some specific goals of mental health promotion: • • • Improve physical health and well-being Prevent or reduce the risk of mental health problems Assist with recovery from mental health problems Improve mental health services Improve quality of life for people with mental health problems Strengthen community capacity to support social inclusion Reduce vulnerability to social and economic stresses Improve health at work, thereby increasing productivity and reducing sick leave Assisting parents, caregivers with developing sustainable supports for their children Clinical Profile of Child & Youth Profile: • Any child or youth in the community who participates in the defined service Medical Necessity Criteria: • Child or youth who are able to live with minimal external interventions related to mental health or substance abuse
 Level Two:")
B. The Infrastructure of the Proposed Alaska System of Care (cont. ) Level Two: Low-Intensity Community Based Services § Community support and wraparound: Services provide follow-up care to children, youth and their families who need ongoing treatment within the community. Those appropriate for this level need minimal assistance and do not require frequent contact and supervision.

Level Two - Sample Service Assessment & Evaluation Service Definition Assessment and evaluation includes screening, diagnostic, and treatment planning services. Included is a continuum of assessment services ranging from a comprehensive psychiatric or psychological evaluation to the administration of one or a combination of psychological tests to examine a particular personality variable. Services may be provided in a variety of settings including hospitals and community-based clinics. There are other assessments as well. Office of Children’s Services (OCS) uses a safety assessment tool/process to assess safety threats and impending danger for children. There assessment processes and tools utilized for resource families, some of which dovetail with the licensing process. Clinical Profile of Child & Youth Profile: • Child or youth that is experiencing behavioral and emotional problems in their daily living to include school, peers, community, and family settings. • Children/youth who have a family history of mental health and substance abuse. Medical Necessity Criteria: • Impairment in daily functioning is not stabilized by structure of home or school environment • Behavioral acting out identified in home and school settings • Complex medical problems may have an underlying impact in behavior
 Level Three:")
B. The Infrastructure of the Proposed Alaska System of Care (cont. ) Level Three: High-Intensity Community-Based Services § Services are provided to children and youth who need intensive support and treatment, but who are living with their families with natural supports or living in an alternative family home or group home. Service coordination is essential to supplement natural supports with daily supervision of client provided by family or staff. Wraparound plans include informal community supports, i. e. , church or self-help groups, family support.

Level Three - Sample Service Mental Health and Substance Abuse Day Treatment Service Definition Mental Health and Substance Abuse Day Treatment provides day based psychiatric services in a school or residential setting to children/youth diagnosed with severe and persistent mental illness, behavioral problems, and those struggling with substance abuse. The goal is to optimize independent living skills and offer support in the recovery process with emphasis on developing healthy coping skills. Clinical Profile of Child & Youth Profile: • Child or youth with an impairment in psychosocial functioning due to the presence of severe symptoms and or behaviors caused by a mental health or substancerelated disorder, which cannot be safely managed on a traditional outpatient basis. Medical Necessity Criteria: • Demonstrates symptomatology consistent with DSM-IV diagnosis • Co-occurring medical conditions, if any, can be safely managed in an outpatient setting. • Co-occurring mental health conditions, if present, can be treated in a dual diagnosis program, or can be safely managed at this level of care. • There is no indication of severe withdrawal, or the symptoms of withdrawal can be safely managed. • The child or youth’s condition requires a coordinated multi-modal treatment plan as well as the structure and intensity of services offered in a Day Treatment Program. • The child or youth or his/her support system understands and can comply with the requirements of a Day Treatment.
 Level Four:")
B. The Infrastructure of the Proposed Alaska System of Care (cont. ) Level Four: Medically Monitored Non-Residential Services § Services are provided to children and youth who need intensive support and treatment but are capable of living in the community either in their family or community placements. Intensive case management by a multidisciplinary treatment team is required to coordinate interventions, provide a wraparound plan, and provide formal supports and crisis intervention services.
 Clinical Profile of Child")
Level Four - Sample Service Youth Assertive Community Treatment (ACT) Clinical Profile of Child & Youth Service Definition Youth ACT is an intensive community-based program that uses a multidisciplinary team of behavioral health professionals and trained peers to provide or coordinate treatment, rehabilitation, and community support services for members who are recovering from severe behavioral health conditions. Profile: • a. b. c. d. Youth who are under 18 years of age: 1. Have severe and persistent mental illness 2. Have a history of: Multiple hospitalizations Poor performance in school Placement in emergency shelters or residential treatment facilities Chemical dependency or abuse 1. Have been placed on probation by a juvenile court Medical Necessity Criteria: • Youth with a diagnosis of schizophrenia, schizoaffective disorder, bipolar, and depression recurrent • History of psychiatric hospitalization, residential placement, and therapeutic foster care • Youth who is impaired in activities of daily living and benefits from participation with intensive supportive services
 Level Five:")
B. The Infrastructure of the Proposed Alaska System of Care (cont. ) Level Five: Medically Monitored and Managed Residential Services § Services are provided to children and youth who need the most intensive support and treatment in a secure/locked in-patient psychiatric setting or highly programmed residential facility. Services may be provided in a community setting if security needs can be met through intensive case management and extensive wraparound support.

Level Five - Sample Service Residential Sex Offender Treatment Service Definition Residential sex offender treatment is a facility or program in a facility that specifically treats sex offenders through an approach including a safe milieu (one in which they can not offend or being offended on), cognitive behavioral treatment, and a psychopharmacology intervention. The core of the treatment process for sex offenders involves the engagement of the resident and family in treatment, helping residents face up to their sexually harmful behavior, identifying the effects of previous trauma, and then developing and practicing a plan for eliminating harmful behavior. Clinical Profile of Child & Youth Profile: • Child or youth charged and/or adjudicated for a sex offense in the state of Alaska • Child/youth may or may not have a mental health or substance abuse diagnosis Medical Necessity Criteria: • Youth with a history of a lower LOC that was community based and reoffends; or • Youth who is adjudicated meets the Alaska criteria of a sex offender; or • Youth who participates in sex offender treatment through weekly outpatient group treatment lasting 8 to 28 months; or • Youth who has motivation to participate in all treatment parameters to include mental health and substance abuse services; or • Youth or child who is a danger to self or other; or • Co-occurring diagnosis
 Instrument § LOC instrument is")
C. The Introduction of a Level of Care (LOC) Instrument § LOC instrument is a tool that can be completed by the child or youth, parent, teacher, counselor, case manager, residential and foster care staff, etc. § Goal of the LOC instrument is to document functional behavior exhibited by the child or youth § Provides a systemic base for decision-making about the necessary level of care for a child or youth
 Instrument (cont. ) § Provides")
C. The Introduction of a Level of Care (LOC) Instrument (cont. ) § Provides information to support the level of care necessary to assist the child or youth and the family § Provides a common language across the SOC § Identifies needs for the child or youth that may or may not be available in the SOC § Compiles data – both individual and aggregate - to support SOC funding and innovation
 Instrument (cont. ) LOC instrument")
C. The Introduction of a Level of Care (LOC) Instrument (cont. ) LOC instrument is not the sole decision-making tool in a SOC § The instrument provides a common language § Supports the identification of services at the appropriate level of care that may support the child or youth and the family §

LOC Instrument Options § § § § § Child & Adolescent Functional Assessment Scale (CAFAS) Child & Adolescent Needs & Strengths (CANS) for children and adolescents, including CANS-CW, CANS-DD, CANSJJ, CANS-MH, and CANS-SD Child Behavior Checklist (CBCL) Child and Adolescent Service Intensity Instrument (CASII) Strengths and Difficulties Questionnaire (SDQ) INTERQUAL Ohio Youth Problems (Ohio Scale) Diagnostic Interview Schedule for Children (DISC) Behavioral Assessment System for Children (BASC) ASAM

LOC Instrument Survey Question #1

LOC Instrument Survey Question #2

LOC Instrument Survey Question #3

LOC Instrument Survey Question #4

LOC Instrument Survey Question #5

LOC Instrument Survey Question #6

LOC Instrument Survey Question #7

LOC Instrument Survey Question #8

LOC Instrument Survey Question #9

LOC Instrument Survey Question #10

D. The Building Blocks of the System of Care § A community partnership among families, youth, schools, and public and private organizations to provide coordinated mental health services Level Five Children Youth Level Four Culturally/Linguistic Competent Level Three Individualized Level Two Level One Social Services Child Welfare Families Community Based Decision-making Coordinated Education Health Strengths-Based Behavioral Health Vocational Community Child-Centered & Family Focus Care Accessible Juvenile Justice Community Supports

D. The Building Blocks of the System of Care Layers One and Two § Offer a diverse array of mental health and non-mental health services and supports: ü social service ü educational ü mental health ü juvenile justice ü recreational ü vocational ü health ü substance abuse ü ‘informal’ community supports
 Layer Three Characteristics")
D. The Building Blocks of the System of Care (cont. ) Layer Three Characteristics of services provided are individually designed for and tailored to the particular strengths and needs of individual families § Family Team will devise a detailed and highly individualized service plan with specific, achievable, strengths-based behavior and treatment goals § Ensure services are accessible to families § Coordination of services through agreed-upon eligibility criteria and shared intake processes, systematic information sharing, routine updates and recording of all services received, and the institutionalization of sharing the service plan across agencies and DHSS divisions §
 Layer Three (cont.")
D. The Building Blocks of the System of Care (cont. ) Layer Three (cont. ) § State Collaborative & Policy Performa Group will need to: ü Provide the leadership necessary to marshal resources, reduce barriers, blend or ‘braid’ funding streams, integrate and alter policies and procedures needed to promote implementation ü Go beyond memoranda of agreement among child-serving agencies at the State and be put into State of Alaska statute ensuring accountability and longevity to the roles of each ü Assist in clarifying roles, responsibilities and ensure coordination and accountability in the SOC ü Craft mechanisms in policy to provide a source of de-categorized funds to Family Teams which are essential to facilitate wraparound approaches necessary to fill in gaps between formal services and fully individualize care in the SOC
 Level Four §")
D. The Building Blocks of the System of Care (cont. ) Level Four § Represents how all services and service delivery practices are influenced by the core values of the Alaska SOC ü Incorporates the family as the service provision unit and uses a broad definition of ‘family’ so that non-custodial caregivers are involved in services and service decision-making ü Family voice in the SOC decisions is represented in decisionmaking bodies, with voting rights when relevant ü SOC promotes the development of family advocacy capacity and family empowerment ü Cultural and linguistic competence will be formalized throughout the system
 Level Four (cont.")
D. The Building Blocks of the System of Care (cont. ) Level Four (cont. ) § Policy Performa Group and State Collaborative, DHSS divisions, and service providers will develop statements of practice and standards with training § SOC utilizes a locus of decision-making at a local (community/village) level which can be accomplished through the development of local advisory councils (LAC) on children’s services § LACs will need to work with DBH to obtain needed resources, identifying and making decisions about service gaps, blending funds to maximize resources, identifying and addressing training needs to build local capacity, and ultimately, by holding each other accountable to meet the needs of their children and families
 Layer Five")
D. The Building Blocks of the System of Care Works (cont. ) Layer Five § Represents the relational model described involving the SOC stakeholders, DHSS divisions, State Collaborative, Policy Performa Group, and LACs Department of Health & Social Services Divisions (DBH, DJJ, OCS, & SDSD) System of Care Stakeholders Children, Youth, Families, & Community or Village State Collaborative (child serving agencies, families, advocates) Policy Performa Group Local Advisory Councils on Children’s Services

E. Coordinated and Sequenced Transition to the New SOC “The Future is something which everyone reaches at the rate of sixty minutes an hour, whatever he does, whoever he is. ” ~C. S. Lewis
 Division of Behavioral")
E. Coordinated and Sequenced Transition to the New SOC (cont. ) Division of Behavioral Health will take the lead role in the implementation of the children’s behavioral health system of care for Alaska § The OPEN MINDS team recommends a three year transition plan for the implementation of the proposed Alaska SOC § ü Year One - Education and training, governance transition, and development of SOC framework ü Year Two - Development of the infrastructure changes in the Department of Health and Social Service’s divisions, building of funding planning committee, and implementation of changes in the AKAIMS ü Year Three - Development of the on-the-ground implications for children, youth and their families; SOC providers; and community stakeholders
 Year One Activities")
E. Coordinated and Sequenced Transition to the New SOC (cont. ) Year One Activities § § § Implement the Education/Training Plan Transition the Division of Behavioral Health to take the lead role in governance of SOC model and operationalizing the transition plan Develop a Policy Performa Group to replace the JMT Transition the residential services from the Office of Children’s Services division to the Division of Behavioral Health Continue support from DBH for the Alaska National Accreditation initiative
 Year Two Activities")
E. Coordinated and Sequenced Transition to the New SOC (cont. ) Year Two Activities Develop the full framework of SOC stakeholders § Develop statements for cultural and linguistic competence practice standards and training § Develop and adopt common standards of practice with specialty treatment needs such as youth sex offenders, MR/DD children or youth with behavioral health concerns, children or youth diagnosed with FASD, children or youth diagnosed with traumatic brain disorders, autism spectrum disorders, etc… § Establish a funding pool advisory team to begin develop process of effectively bundling and braiding funding resources §
 Year Two Activities")
E. Coordinated and Sequenced Transition to the New SOC (cont. ) Year Two Activities (cont. ) § Initiate an informed development of evidence-based practices (EBP) group 1. Collect relevant information about target population to inform development of services – Define population and needs 5. Evaluate the input on critical system issues and make modifications 2. Identify critical system issues (e. g. too many youth in high and out-ofhome care, too many youth out-ofstate ·Service Standards and clinical guidelines ·Reimbursement rates that cover costs ·Program certification standards ·Automatic adaptation to unique care and populations ·Workforce analysis retention and recruitment ·Training and skill development ·Supervisory structures ·Assessment and referral processes ·Fidelity monitoring ·Utilization management structures ·Outcome monitoring ·Information management and reporting requirements 4. Develop evidence-based services and infrastructure to ensure their success 3. Select services with empirical support to address specific needs of target population
 Year Three Evaluate")
E. Coordinated and Sequenced Transition to the New SOC (cont. ) Year Three Evaluate the services within the five levels of the proposed Alaska SOC and determine which services meet the vision of the SOC, the needs of the community or village, and the availability of resources to activate the services § Develop a five year plan to maintain and build the service base § DBH, DJJ, OCS, and SDSD to blend and braid funding into a pool for the SOC to include federal, state, and foundation grants §
 Year Three (cont.")
E. Coordinated and Sequenced Transition to the New SOC (cont. ) Year Three (cont. ) Integrate the proposed Alaska SOC into the AKAIMs initiative to include both the clinical electronic health record and the billing component of the information system, performance measures are adopted, and outcome data is gathered for regular use in SOC maintenance and new service development § On going evaluation of the system with the use of the LACs, State Collaborative, DBH, Policy Performa Group, Family Teams, and the Children, Youth and Families utilizing the SOC §

VI. Sources of Funding Methods 92 OPEN MINDS © 2009. All rights reserved.

A. Sources of Funding Methods Medicaid is the most important driver of children’s mental health fiscal policy § States across the country fund the services in their SOCs with a diverse pool of funds but all have a heavy investment in Medicaid § Complexities of the finance system for children’s behavioral health are in-part related to both the purchasers of services and deliverers of the services §
 SOC Funding Sources State and local general")
A. Sources of Funding Methods (cont. ) SOC Funding Sources State and local general revenue (including those from tribal jurisdictions) § Federal discretionary funds, entitlements and formula and block grants: § ü Medicaid and the State Children’s Health Insurance ü Program (SCHIP) ü Temporary Assistance to Needy Families (TANF) ü Social Services Block Grant (SSBG) ü Federal categorical revenue allocated toward specific health and human service agencies, in particular but not limited to the federal Departments of Health and Human Services (DHHS), which includes SAMHSA Education and Justice;
 SOC Funding Sources (cont. ) Indian Health")
A. Sources of Funding Methods (cont. ) SOC Funding Sources (cont. ) Indian Health Service § A host of private payers including insurers and employers § For substance abuse, it also includes: § ü Substance Abuse Prevention and Treatment Block Grant ü Medicaid and EPSDT ü SCHIP ü Indian Health Service ü State general funds
")
A. Sources of Funding Methods (cont. )
 Elements of service that typify state fiscal")
A. Sources of Funding Methods (cont. ) Elements of service that typify state fiscal policy: § § § Over-reliance on residential treatment Lack of access to, or the availability of, community-based treatment alternatives Fiscal practices, particularly through Medicaid, are inconsistent with the knowledge base about effective children’s behavioral health services Insensitivity to prevention and early intervention Limited incentives to plan strategically and to support leadership informed by children’s behavioral health knowledge
 Elements of service typify state fiscal policy")
A. Sources of Funding Methods (cont. ) Elements of service typify state fiscal policy (cont. ): § § § State-based service inequities driven by variation in the use of available Medicaid provisions Fiscal policies that are often out of sync with the developmental needs of children and youth Poor information technology Inadequate alignment of fiscal policy with quality initiatives Missed opportunities to seize the initiative at the federal level to embed best fiscal practices
")
A. Sources of Funding Methods (cont. )

B. Alaska SOC Financing Seven areas must be addressed in a strategic financing plan for the proposed SOC: 1. Identifying spending and utilization patterns across agencies through the AK-AIMs 2. Realigning funding streams and structures through the use of the SOC Performa Policy Group 3. Financing appropriate services and supports identified by the Performa Policy Group and State Collaborative

B. Alaska SOC Financing Seven areas must be addressed in a strategic financing plan for the propose SOC: 4. Financing to support family and youth partnerships identified by the State Collaborative 5. Financing to improve cultural and linguistic competence and reduce disparities in care identified by the Performa Policy Group 6. Financing to improve the workforce and provider network 7. Financing for accountability

B. Alaska SOC Financing Strategies to Successfully Fund the Proposed SOC: 1. Set up an extensive provider network with performance based contracts demonstrating: ü Outcomes with children, youth, and families ü Continuous improvement processes typically associated with national accreditation ü Flexible systems for children and youth to move through services and levels Implement shared-risk contracts between the state of Alaska and Grantees with a focus on flexibility, creative collaboration, and risk management in regards to immediate needs of the SOC. 3. Implement a model ‘one care plan’ model that is coordinated through a single accountable entity but funded with resources from various programs. 2.
: 4.")
B. Alaska SOC Financing Strategies to Successfully Fund the Proposed SOC (cont. ): 4. Establish a blended or braided model of funding or a combination of both ü Blended funding can allow systems to fund activities that are not reimbursable through specific categorical programs ü Braided funding allows resources to be tracked more closely for the purpose of accounting to federal program administrators ü Combination funding requires the funding management to be put under the structure of one division and in the case of the Alaska SOC, DBH would be the logical choice
: 5.")
B. Alaska SOC Financing Strategies to Successfully Fund the Proposed SOC (cont. ): 5. Establish a SOC planning team made up of DBH, OCS, & DJJ to provide oversight of funding for the SOC and determine different ways of using two categories of federal funding : ü Ongoing funding streams such as block grants or entitlement programs that provide resources year after year in a reliable fashion ü Discretionary grants, which are time-limited and often require state or local matching funds

B. Alaska SOC Financing

B. Alaska SOC Financing

VII. Outcome Measure Recommendation 10 7 OPEN MINDS © 2009. All rights reserved.

Recommendations § Recommendation One: Develop points of accountability for all groups (LACs, State Collaborative, DBH, PPG, and Children, Youth and Families) within the proposed framework in Figure Five § Recommendation Two: Invest in community voice and buyin through the development of Local Advisory Councils on Children’s Services in communities and villages across Alaska. Develop this model in the form of a state statute to ensure the model has a state and SOC value that is reported on in the Legislative process
 § Recommendation Three: Promote fidelity to the proposed Alaska SOC model")
Recommendations (cont. ) § Recommendation Three: Promote fidelity to the proposed Alaska SOC model through the Policy Performa Group to provide SOC fidelity monitoring § Recommendation Four: Establish a cross-division training initiative which encourages and promotes understanding of the goals of the divisions under DHSS, the funding models utilized to support service delivery, and develop potential future leadership for DHSS § Recommendation Five: Enhance the utilization of AK-AIMs throughout the proposed Alaska SOC. Mobilize the clinical and financial components to AK-AIMs to establish a data driven decision-making SOC
 § Recommendation Six: Continue to sponsor the Change Agent Conferences for")
Recommendations (cont. ) § Recommendation Six: Continue to sponsor the Change Agent Conferences for SOC stakeholders to promote the SOC and enhance the effectiveness of the SOC § Recommendation Seven: Identify spending and utilization patterns across agencies in the SOC to develop performance based standards § Recommendation Eight: Develop shared risk and performance based contracts with SOC stakeholders
 § Recommendation Nine: Establish a plan to adopt and develop informed")
Recommendations (cont. ) § Recommendation Nine: Establish a plan to adopt and develop informed evidence-based practices within the SOC. § Recommendation Ten: Establish twice a year meetings to review and assess the progress in the implementation of the proposed Alaska SOC through DBH and the Policy Performa Group

VIII. Sustaining the Behavioral Health System of Care for Children 11 2 OPEN MINDS © 2009. All rights reserved.

Recommendations for sustainability of the Alaska SOC 1. Strengthen organizational partnerships across traditional child-serving service sectors. ü ü Cross-agency Partnerships Provider Relationships Shared System Management School-Based Mental Health OPEN MINDS © 2009. All rights reserved.

Recommendations for sustainability of the Alaska SOC 2. Make use of key system stabilizers such as relationships with community and family organizations. ü Revitalize Community Voice through Local Advisory Councils on Children Services. ü Strengthen Partnerships with Children, Youth, and Families particularly in community/village wellbeing initiatives 11 4 OPEN MINDS © 2009. All rights reserved.

Recommendations for sustainability of the Alaska SOC 3. Support Care Coordination function ü Case load limitations ü Administrative support ü Statewide training • • • 11 5 Introduction to case management Case management supervision Advanced case management strategies OPEN MINDS © 2009. All rights reserved.

Recommendations for sustainability of the Alaska SOC Conclusion - the sustainability of the Alaska System of Care requires a single division with accountability for the SOC governance. The framework of the proposed Alaska SOC is built on the development of the Performa Policy Group, State Collaborative, LACs for Children Services, and the Family teams. The SOC also requires a commitment to a level of care instrument that provides for common language about the SOC, the SOC resources, and the needs of children, youth, and families. 11 6 OPEN MINDS © 2009. All rights reserved.

Questions & Discussion 11 7 OPEN MINDS © 2009 All rights reserved.

Proposed Alaska Children’s Behavioral Health System of Care www. openminds. com openminds@openminds. com 717 -334 -1329 163 York Street, Gettysburg, Pennsylvania 17325 OPEN MINDS © 2009. All rights reserved.
b5eea7aa42ff56a466a6f7b6bebc0ef5.ppt