

4b9b1671c558a9d13834baefe119e29e.ppt
- Количество слайдов: 25
 Preoperative Pulmonary Evaluation Chang Shim, MD Professor of Medicine Jacobi Medical Center
Preoperative Pulmonary Evaluation Chang Shim, MD Professor of Medicine Jacobi Medical Center
 Postoperative Complications Pulmonary Pneumonia/atelectasis: abnormal CXR, fever, leukocytosis, ABG Respiratory failure/mechanical ventilation Pulmonary embolism Cardiovascular CHF Arrhythmias Ischemia/MI Hypotension/hypertension Neurological Stroke Psychosis Infection, sepsis Wound, lines, others GI Renal
Postoperative Complications Pulmonary Pneumonia/atelectasis: abnormal CXR, fever, leukocytosis, ABG Respiratory failure/mechanical ventilation Pulmonary embolism Cardiovascular CHF Arrhythmias Ischemia/MI Hypotension/hypertension Neurological Stroke Psychosis Infection, sepsis Wound, lines, others GI Renal
 Non-pulmonary Risk Factors for Post-op Pulmonary Complications Extent and Location of Surgery Duration of Anesthesia Age Gender Weight, BMI ASA (American Society of Anesthesiology) Score 1 A normal healthy person 2 Mild systemic disease 3 Systemic disease that is not incapacitating. 4 Incapacitating systemic disease that is threatening to life 5 Moribund, not expected to survive 24 hours with or without operation.
Non-pulmonary Risk Factors for Post-op Pulmonary Complications Extent and Location of Surgery Duration of Anesthesia Age Gender Weight, BMI ASA (American Society of Anesthesiology) Score 1 A normal healthy person 2 Mild systemic disease 3 Systemic disease that is not incapacitating. 4 Incapacitating systemic disease that is threatening to life 5 Moribund, not expected to survive 24 hours with or without operation.
 Risk Assessment for and Strategies to Reduce Perioperative Pulmonary Complications for Patients Undergoing Noncardiothoracic Surgery (ACP) Annals Intern Med April 2006 1. 2. 3. 4. 5. 6. All should be evaluated for the presence of COPD, age >60 yrs, ASA class II or greater, functionally dependent, & CHF. Obesity and mild or mod asthma: not significant risk factors Higher risk for complications: prolonged surgery (>3 H), abdominal surgery, thoracic surgery, neurosurgery, head and neck surgery, vascular surgery, aortic aneurysm repair, emergency surgery, and general anesthesia. Low serum albumin level <35 g/L. All those suspected to have low albumin or those with 1 or more risk factors. Those who have higher risk for complications should have deep breathing exercise or incentive spirometry and selective use of nasogastric tube post op. Preoperative spirometry and chest radiography should not be used routinely for predicting risk for postop complications. Right heart cath and total parenteral nutrition should not be used to reduce pulmonary complications.
Risk Assessment for and Strategies to Reduce Perioperative Pulmonary Complications for Patients Undergoing Noncardiothoracic Surgery (ACP) Annals Intern Med April 2006 1. 2. 3. 4. 5. 6. All should be evaluated for the presence of COPD, age >60 yrs, ASA class II or greater, functionally dependent, & CHF. Obesity and mild or mod asthma: not significant risk factors Higher risk for complications: prolonged surgery (>3 H), abdominal surgery, thoracic surgery, neurosurgery, head and neck surgery, vascular surgery, aortic aneurysm repair, emergency surgery, and general anesthesia. Low serum albumin level <35 g/L. All those suspected to have low albumin or those with 1 or more risk factors. Those who have higher risk for complications should have deep breathing exercise or incentive spirometry and selective use of nasogastric tube post op. Preoperative spirometry and chest radiography should not be used routinely for predicting risk for postop complications. Right heart cath and total parenteral nutrition should not be used to reduce pulmonary complications.
 Patient-Related Risk Factors • • • Age: odds ratio 1 for <60, 1. 79 for 60 -69, 3. 04 for 70 -79. COPD: odds ratio 1. 79 Cigarette Use: OR 1. 26 CHF: OR 2. 93 Functional Dependence: OR 2. 51 for total, 1. 65 for partial dependence ASA Classification I 1. 2%, II 5. 4%, III 11. 4%, IV 10. 9%, IV not available Obesity: not a risk factor Asthma: not a risk factor OSA: airway management issues but not pulmonary complication Impaired sensorium, abn chest examination, alcohol use, wt loss: inc
Patient-Related Risk Factors • • • Age: odds ratio 1 for <60, 1. 79 for 60 -69, 3. 04 for 70 -79. COPD: odds ratio 1. 79 Cigarette Use: OR 1. 26 CHF: OR 2. 93 Functional Dependence: OR 2. 51 for total, 1. 65 for partial dependence ASA Classification I 1. 2%, II 5. 4%, III 11. 4%, IV 10. 9%, IV not available Obesity: not a risk factor Asthma: not a risk factor OSA: airway management issues but not pulmonary complication Impaired sensorium, abn chest examination, alcohol use, wt loss: inc
 Procedure Related Risk Factors • Surgical Site: inc risk for aortic aneurysm repair, thoracic surgery, abdominal surgery, upper abd surgery, neurosurgery, prolonged surgery, head and neck surgery, emergency surgery, vascular sur • Duration of Surgery: 3 -4 hours increase risks • Anesthetic Technique: general vs local or regional • Emergency Surgery: OR 2. 21
Procedure Related Risk Factors • Surgical Site: inc risk for aortic aneurysm repair, thoracic surgery, abdominal surgery, upper abd surgery, neurosurgery, prolonged surgery, head and neck surgery, emergency surgery, vascular sur • Duration of Surgery: 3 -4 hours increase risks • Anesthetic Technique: general vs local or regional • Emergency Surgery: OR 2. 21
 Laboratory Testing to Estimate Risk • Spirometry: value unproven except in lung resection and coronary bypass graft • Chest Radiographs: 23% abn, 3% clin important • Blood Urea Nitrogen: >21 risk factor, magnitude? • Oro-pharyngeal Culture: ? • Serum Albumin Measurement: 36 g/L 27. 6% v 7% – 35 g/L threshold value is one of the most powerful risk factor.
Laboratory Testing to Estimate Risk • Spirometry: value unproven except in lung resection and coronary bypass graft • Chest Radiographs: 23% abn, 3% clin important • Blood Urea Nitrogen: >21 risk factor, magnitude? • Oro-pharyngeal Culture: ? • Serum Albumin Measurement: 36 g/L 27. 6% v 7% – 35 g/L threshold value is one of the most powerful risk factor.
 Strategies to Reduce Postoperative Pulmonary Complications • • • Preoperative Smoking Cessation Lung Expansion Modalities Neuromuscular Blockade: avoid pancuronium Anesthesia and Analgesia: neuraxial blockade Surgical Techniques: laparoscopic vs open? Perioperative Care – Nutritional Support, Pulmonary Artery Catheterization, Selective Nasogastric Decompression after Abdominal Surgery
Strategies to Reduce Postoperative Pulmonary Complications • • • Preoperative Smoking Cessation Lung Expansion Modalities Neuromuscular Blockade: avoid pancuronium Anesthesia and Analgesia: neuraxial blockade Surgical Techniques: laparoscopic vs open? Perioperative Care – Nutritional Support, Pulmonary Artery Catheterization, Selective Nasogastric Decompression after Abdominal Surgery
 Predictors of Post-operative Pulmonary Complications Mc. Alister FA, et al. Am J Respir Crit Care Med 2003; 167: 741 • 22 general internists and pulmonologists in 10 groups, a Canadian study • 272 patients referred for pre-op evaluation • Exclusion: on ventilator, sleep apnea, known neuromuscular disease, cognitive impairment, intrathoracic or severe orthopedic surgery. • Pulmonary complication before discharge or 7 days post • Outcome: respiratory failure requiring mechanical vent, pneumonia, lung or lobar atelectasis requiring bronchoscop
Predictors of Post-operative Pulmonary Complications Mc. Alister FA, et al. Am J Respir Crit Care Med 2003; 167: 741 • 22 general internists and pulmonologists in 10 groups, a Canadian study • 272 patients referred for pre-op evaluation • Exclusion: on ventilator, sleep apnea, known neuromuscular disease, cognitive impairment, intrathoracic or severe orthopedic surgery. • Pulmonary complication before discharge or 7 days post • Outcome: respiratory failure requiring mechanical vent, pneumonia, lung or lobar atelectasis requiring bronchoscop
 Predictors of Postoperative Pulmonary Risk Ma. Alister FA , et al Am J Repir Crit Care Med 2003; 167: 741 • 272 referred for evaluation before nonthoracic surgery— 22 (8%) had postop pulm complications: 6 respir failure, 9 pneumonia, 7 atelectasis. • Hypercapnea, p. CO 2 =>45 mm. Hg, odds ratio 66 • FVC less than 1. 5 liters, OR 11. 1 • Maximal laryngeal height =<4 cm, OR 6. 9 • Forced expiratory time =>9 seconds, OR 5. 7 • Smoking =>40 pack-years, OR 1. 9 • BMI =>30, OR 4. 1 • Multiple regression analysis: age =>65 OR 1. 8, smoking 40 pk-yrs, OR 1. 9, laryngeal height =<4 cm, OR 2. 0
Predictors of Postoperative Pulmonary Risk Ma. Alister FA , et al Am J Repir Crit Care Med 2003; 167: 741 • 272 referred for evaluation before nonthoracic surgery— 22 (8%) had postop pulm complications: 6 respir failure, 9 pneumonia, 7 atelectasis. • Hypercapnea, p. CO 2 =>45 mm. Hg, odds ratio 66 • FVC less than 1. 5 liters, OR 11. 1 • Maximal laryngeal height =<4 cm, OR 6. 9 • Forced expiratory time =>9 seconds, OR 5. 7 • Smoking =>40 pack-years, OR 1. 9 • BMI =>30, OR 4. 1 • Multiple regression analysis: age =>65 OR 1. 8, smoking 40 pk-yrs, OR 1. 9, laryngeal height =<4 cm, OR 2. 0
 Postoperative Pneumonia Risk Index Arozullah, AM et al Multifactorial Risk Index for postop pneumonia. Ann Intern Med 2001; 135: 847 -57 • 100 VA Hosp 160, 805 major non-cardiac surgery 9/97 to 8/99— 2466 cases (1. 5%) developed pneumonia. • Developed risk index to predict post-op pneumonia and validated it by using cases 1995 -97. • Type of surgery: abd aortic aneurysm, thor, up abd, neck, vasc, neuro • Age =>80, 70 -79, 60 -69, 50 -59 • Functional status: total dependent, partial dependent • Wt loss >10% in 6 months • Hx COPD • Others: General anesthesia, impaired sensorium, Hx CVA, BUN <8 mg/dl, Transfusion >4 units, emergency surgery, chronic steroid use, current smoker, alcohol >2 drinks/d • Risk point system used to categorize risk class 1 -5, 0 -15 risk points, 16 -25, 26 -40, 41 -55, >55, Pneumonia rates were 0. 24% to 15. 9%.
Postoperative Pneumonia Risk Index Arozullah, AM et al Multifactorial Risk Index for postop pneumonia. Ann Intern Med 2001; 135: 847 -57 • 100 VA Hosp 160, 805 major non-cardiac surgery 9/97 to 8/99— 2466 cases (1. 5%) developed pneumonia. • Developed risk index to predict post-op pneumonia and validated it by using cases 1995 -97. • Type of surgery: abd aortic aneurysm, thor, up abd, neck, vasc, neuro • Age =>80, 70 -79, 60 -69, 50 -59 • Functional status: total dependent, partial dependent • Wt loss >10% in 6 months • Hx COPD • Others: General anesthesia, impaired sensorium, Hx CVA, BUN <8 mg/dl, Transfusion >4 units, emergency surgery, chronic steroid use, current smoker, alcohol >2 drinks/d • Risk point system used to categorize risk class 1 -5, 0 -15 risk points, 16 -25, 26 -40, 41 -55, >55, Pneumonia rates were 0. 24% to 15. 9%.
 Respiratory Effects of General Anesthesia Control of Ventilation CO 2, Hypoxia, Pattern COPD FRC, Airways closure Diaphragm movement Atelectasis Respiratory pattern, O 2 Ventilation/perfusion matching Dead space, shunt Bronchomotor tone Mucociliary clearance
Respiratory Effects of General Anesthesia Control of Ventilation CO 2, Hypoxia, Pattern COPD FRC, Airways closure Diaphragm movement Atelectasis Respiratory pattern, O 2 Ventilation/perfusion matching Dead space, shunt Bronchomotor tone Mucociliary clearance
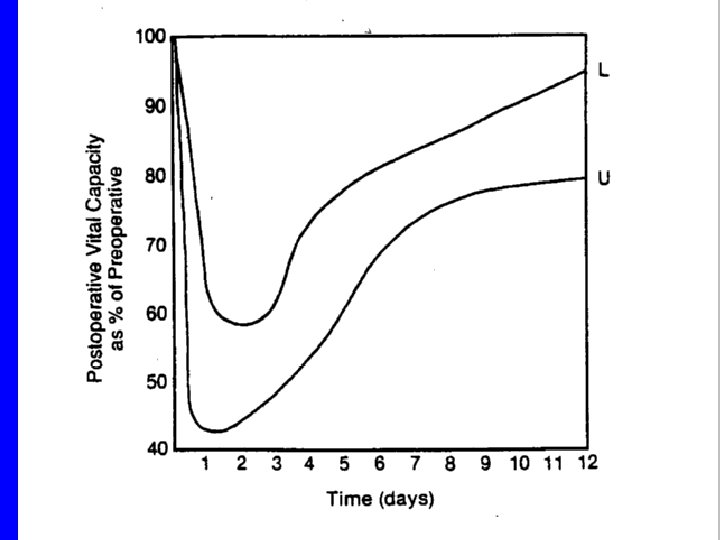
 Postoperative Decline in Lung Function • TLC and VC declined similarly • FRC decreased half as much as VC • RV decreased less than FRC
Postoperative Decline in Lung Function • TLC and VC declined similarly • FRC decreased half as much as VC • RV decreased less than FRC
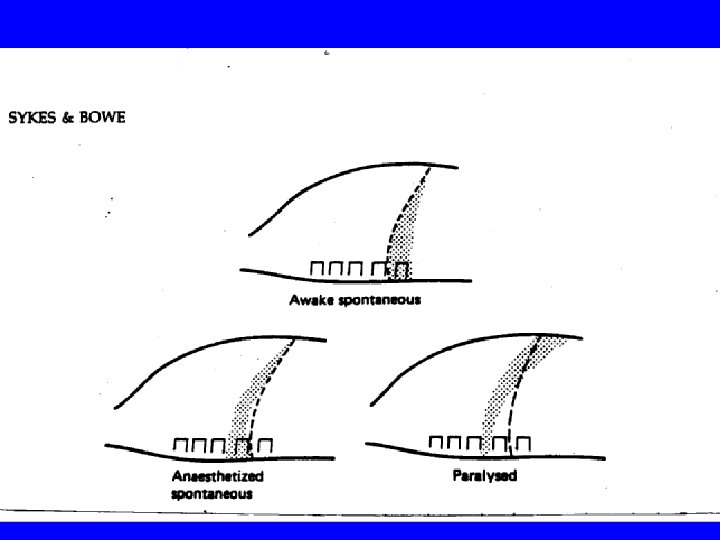
 Diaphragmatic Function Descends during inspiration pushing down abdominal content. Lifts up thoracic cage, using inertia of abdominal content as a fulcrum Anesthesia, spontaneous respiration Neuromuscular block Mechanical ventilation
Diaphragmatic Function Descends during inspiration pushing down abdominal content. Lifts up thoracic cage, using inertia of abdominal content as a fulcrum Anesthesia, spontaneous respiration Neuromuscular block Mechanical ventilation
 Who should have pre-op PFT evaluation? Known pulmonary disease Planned lung resection Smoker or heavy smoker? Tests: Match test: FEV 1 of 1. 8 liters Spirometry (FVC, FEV 1), PEFR Diffusion capacity ABGs
Who should have pre-op PFT evaluation? Known pulmonary disease Planned lung resection Smoker or heavy smoker? Tests: Match test: FEV 1 of 1. 8 liters Spirometry (FVC, FEV 1), PEFR Diffusion capacity ABGs
 Types of Anesthesia General vs spinal Regional
Types of Anesthesia General vs spinal Regional
 Atelectasis and Pneumonia Anesthesia and Surgery Mucociliary Clearance Muscle Weakness Ventilatory Pain Drive Narcotics Shallow breathing Cough Atelectasis V/Q mismatch Hypoxia/infection
Atelectasis and Pneumonia Anesthesia and Surgery Mucociliary Clearance Muscle Weakness Ventilatory Pain Drive Narcotics Shallow breathing Cough Atelectasis V/Q mismatch Hypoxia/infection
 Lung Hyperinflation Maneuvers Adequate analgesia and motivation are necessary. Cough and deep breathing: preferably trained preoperatively. Incentive spirometer: excellent device rarely used efficiently. Would pre-op training help? CPAP or Bi. PAP for a few minutes every 2 -4 hours (10 to 20 cm water pressure) is more effective.
Lung Hyperinflation Maneuvers Adequate analgesia and motivation are necessary. Cough and deep breathing: preferably trained preoperatively. Incentive spirometer: excellent device rarely used efficiently. Would pre-op training help? CPAP or Bi. PAP for a few minutes every 2 -4 hours (10 to 20 cm water pressure) is more effective.
 COPD Complications Atelectasis/pneumonia Respiratory failure/mechanical ventilation History Airflow obstruction/exercise capacity Smoking Cough and sputum production Assessment and intervention PFTs, ABGs: FEV 1 of 0. 7 liter, p. CO 2 of >45 mm. Hg Smoking cessation Antibiotics for those who have sputum production, 3 -5 days pre-op Systemic corticosteroids: prednisone 40 mg daily x 3 days Bronchodilators: beta agonists, anticholinergics, theophylline Cough and Hyperinflation maneuvers
COPD Complications Atelectasis/pneumonia Respiratory failure/mechanical ventilation History Airflow obstruction/exercise capacity Smoking Cough and sputum production Assessment and intervention PFTs, ABGs: FEV 1 of 0. 7 liter, p. CO 2 of >45 mm. Hg Smoking cessation Antibiotics for those who have sputum production, 3 -5 days pre-op Systemic corticosteroids: prednisone 40 mg daily x 3 days Bronchodilators: beta agonists, anticholinergics, theophylline Cough and Hyperinflation maneuvers
 Asthma History and PEFR Completely asymptomatic for 6 months or longer PEFR is normal Treatment: bronchodilator only peri-operatively Symptoms present within 6 months PEFR abnormal <80% predicted Prednisone 40 mg daily x 3 pre-op and x 3 post-op If patient is well post-operatively, discontinue it. If not well, continue prednisone until well.
Asthma History and PEFR Completely asymptomatic for 6 months or longer PEFR is normal Treatment: bronchodilator only peri-operatively Symptoms present within 6 months PEFR abnormal <80% predicted Prednisone 40 mg daily x 3 pre-op and x 3 post-op If patient is well post-operatively, discontinue it. If not well, continue prednisone until well.
 Obesity Independent risk factor for pulmonary complications particularly atelectasis Risk of hypoventilation, hypercapnea Hypoxia Obstructive Sleep Apnea (OSA) Interventions Upright positioning Oxygen used sparingly CPAP, Bi. PAP, Incentive spirometry
Obesity Independent risk factor for pulmonary complications particularly atelectasis Risk of hypoventilation, hypercapnea Hypoxia Obstructive Sleep Apnea (OSA) Interventions Upright positioning Oxygen used sparingly CPAP, Bi. PAP, Incentive spirometry
") Lung Resection Candidate Goal: adequate remaining lung to sustain independent breathing (free of ventilator) Residual FEV 1 of at least 800 ml, VC of 1 liter Possibility of unexpected pneumonectomy Perfusion scan to estimate lung function loss FEV 1 value x % residual function= FEV 1 estimate ABGs: PCO 2 >45 mm. Hg: high risk Pulmonary artery hypertension mean >25 mm. Hg Exercise test: stair climbing, 6 minute walk test: excellent prognosticator
Lung Resection Candidate Goal: adequate remaining lung to sustain independent breathing (free of ventilator) Residual FEV 1 of at least 800 ml, VC of 1 liter Possibility of unexpected pneumonectomy Perfusion scan to estimate lung function loss FEV 1 value x % residual function= FEV 1 estimate ABGs: PCO 2 >45 mm. Hg: high risk Pulmonary artery hypertension mean >25 mm. Hg Exercise test: stair climbing, 6 minute walk test: excellent prognosticator