

34a7472e7f720cd9fa6caa46b7e33d90.ppt
- Количество слайдов: 25
 Practical Aspects of Nutrition Support in the ICU John W. Drover, MD, FRCSC, FACS Associate Professor Queen’s University Kingston, ON Canada www. criticalcarenutrition. com
Practical Aspects of Nutrition Support in the ICU John W. Drover, MD, FRCSC, FACS Associate Professor Queen’s University Kingston, ON Canada www. criticalcarenutrition. com
 Disclosure Information • None www. criticalcarenutrition. com
Disclosure Information • None www. criticalcarenutrition. com

 Objectives At the end of the session the participant will be able to: • List 3 strategies to maximize the benefits of enteral nutrition. • List 2 advantages of post-pyloric enteral feeding. • Identify 1 method of gaining post-pyloric access at the bedside in the ICU.
Objectives At the end of the session the participant will be able to: • List 3 strategies to maximize the benefits of enteral nutrition. • List 2 advantages of post-pyloric enteral feeding. • Identify 1 method of gaining post-pyloric access at the bedside in the ICU.
 Outline • Review the rationale for enteral feeding. • Focus on the data regarding post-pyloric feeding. – Specifically RCT’s – Clinically important outcomes • Review the risks of and obstacles to post -pyloric feeding. • Develop a recommendation www. criticalcarenutrition. com
Outline • Review the rationale for enteral feeding. • Focus on the data regarding post-pyloric feeding. – Specifically RCT’s – Clinically important outcomes • Review the risks of and obstacles to post -pyloric feeding. • Develop a recommendation www. criticalcarenutrition. com
 Case #1 • • Day #1 50 yo female COPD with CAP Intubated, resuscitated Who would start EN within 24 hours of admission? • Who would attempt to place a post -pyloric feeding tube?
Case #1 • • Day #1 50 yo female COPD with CAP Intubated, resuscitated Who would start EN within 24 hours of admission? • Who would attempt to place a post -pyloric feeding tube?
 Case #2 • • • Day #5 50 yo female COPD with CAP Intubated, resuscitated feeding tube in stomach Receiving metoclopromide Achieving <30% of goal; GRV >400 ml • Who would recommend placement of a post-pyloric feeding tube?
Case #2 • • • Day #5 50 yo female COPD with CAP Intubated, resuscitated feeding tube in stomach Receiving metoclopromide Achieving <30% of goal; GRV >400 ml • Who would recommend placement of a post-pyloric feeding tube?
 Nutrition in the Critically ill • Enteral nutrition strongly recommended • Early enteral nutrition recommended • Optimize the benefits and minimize risks – Use of feeding protocols – Motility agents for gastric feeding – Small bowel feeding
Nutrition in the Critically ill • Enteral nutrition strongly recommended • Early enteral nutrition recommended • Optimize the benefits and minimize risks – Use of feeding protocols – Motility agents for gastric feeding – Small bowel feeding
 Intra-gastric feeding The good: • Easy access • Early initiation • Often tolerated well The bad: • Gastric residual volumes (GRV’s) • Gastro-pharyngeal reflux • Respiratory aspiration • Unrealized nutritional goals
Intra-gastric feeding The good: • Easy access • Early initiation • Often tolerated well The bad: • Gastric residual volumes (GRV’s) • Gastro-pharyngeal reflux • Respiratory aspiration • Unrealized nutritional goals
 Post-pyloric feeding 2 RCT’s that have evaluated aspiration • 33 patients, 1 st 3 days – GE regurg 24. 9% vs. 39. 8% (p=0. 04) – Further into small bowel less aspiration Heyland et al, CCM, 2001 • 54 patients, twice weekly – Low rate of aspiration – 7% vs 13% aspiration Esparaza et al, Int Care Med, 2001
Post-pyloric feeding 2 RCT’s that have evaluated aspiration • 33 patients, 1 st 3 days – GE regurg 24. 9% vs. 39. 8% (p=0. 04) – Further into small bowel less aspiration Heyland et al, CCM, 2001 • 54 patients, twice weekly – Low rate of aspiration – 7% vs 13% aspiration Esparaza et al, Int Care Med, 2001
, Med") Post-pyloric feeding • 11 RCT’s of SB vs Gastric feeding – Med/Surg (4), Med (3), Trauma (2), Neuro (2) – N=664 – One study used arginine containing diets – Variable design for selection – Different methods of enteral access • Outcomes – No difference in mortality, LOS, vent days Heyland et al, JPEN 2002
Post-pyloric feeding • 11 RCT’s of SB vs Gastric feeding – Med/Surg (4), Med (3), Trauma (2), Neuro (2) – N=664 – One study used arginine containing diets – Variable design for selection – Different methods of enteral access • Outcomes – No difference in mortality, LOS, vent days Heyland et al, JPEN 2002
 Post-pyloric feeding • Taylor et al. CCM, 1999 – Neurotrauma, n=82 • Standard gastric feeding – 15 ml/h increase Q 8 h • Aggressive SB feeding (when feasible) – SB access only 34% – Start at target rate and adjust • Outcomes – Pneumonia 44% vs 63%(NS)
Post-pyloric feeding • Taylor et al. CCM, 1999 – Neurotrauma, n=82 • Standard gastric feeding – 15 ml/h increase Q 8 h • Aggressive SB feeding (when feasible) – SB access only 34% – Start at target rate and adjust • Outcomes – Pneumonia 44% vs 63%(NS)
 Post-pyloric feeding Nutritional outcomes • Small bowel feeding associated with – Reaching nutritional goals sooner – Better success at meeting goals • Meta-analysis not possible – Variable gastric feeding strategies – Goals and success reported in different ways
Post-pyloric feeding Nutritional outcomes • Small bowel feeding associated with – Reaching nutritional goals sooner – Better success at meeting goals • Meta-analysis not possible – Variable gastric feeding strategies – Goals and success reported in different ways
 • 8 clinical criteria; 1 bronchoscopy") Post-pyloric feeding • Infections – pneumonia (9 studies) • 8 clinical criteria; 1 bronchoscopy • SB feeding associated with reduced pneumonia – RR=0. 77(0. 60 -1. 0), p=0. 05 – 23% risk reduction • With Taylor study removed – RR=0. 83(0. 6 -1. 15), p=0. 3
Post-pyloric feeding • Infections – pneumonia (9 studies) • 8 clinical criteria; 1 bronchoscopy • SB feeding associated with reduced pneumonia – RR=0. 77(0. 60 -1. 0), p=0. 05 – 23% risk reduction • With Taylor study removed – RR=0. 83(0. 6 -1. 15), p=0. 3
 Post-pyloric feeding
Post-pyloric feeding
 Post-pyloric feeding
Post-pyloric feeding
 Controversy “A comparison of early gastric feeding in critically ill patients: a meta-analysis” • No difference in outcomes • Same RCT’s • Exclude Taylor • Use studies of reflux • Didn’t count all pneumonia in Montecalvo study Ho et al, ICM 2006
Controversy “A comparison of early gastric feeding in critically ill patients: a meta-analysis” • No difference in outcomes • Same RCT’s • Exclude Taylor • Use studies of reflux • Didn’t count all pneumonia in Montecalvo study Ho et al, ICM 2006
 Post-pyloric feeding • Problems associated with: – Difficult to achieve – Once achieved may move – Doesn’t overcome all issues Canadian survey says 10% • (eg. ACS, short bowel, enteric fistula) • Bowel necrosis – rare event not clearly associated with enteral nutrition Zaloga: Nutrition Week 2005
Post-pyloric feeding • Problems associated with: – Difficult to achieve – Once achieved may move – Doesn’t overcome all issues Canadian survey says 10% • (eg. ACS, short bowel, enteric fistula) • Bowel necrosis – rare event not clearly associated with enteral nutrition Zaloga: Nutrition Week 2005
 The ENTERIC Study The Early Nasojejunal Tube To Meet Energy Requirements In Intensive Care Study Investigators: Andrew R Davies Rinaldo Bellomo D Jamie Cooper Gordon S Doig Simon R Finfer Daren K Heyland For the ANZICS Clinical Trials Group
The ENTERIC Study The Early Nasojejunal Tube To Meet Energy Requirements In Intensive Care Study Investigators: Andrew R Davies Rinaldo Bellomo D Jamie Cooper Gordon S Doig Simon R Finfer Daren K Heyland For the ANZICS Clinical Trials Group
 Conclusions • SB feeding improves – time to reach target goals – success at achieving target goals • SB feeding may be associated with less pneumonia
Conclusions • SB feeding improves – time to reach target goals – success at achieving target goals • SB feeding may be associated with less pneumonia
 Discussion • Routine use: – Difficulties of SB access • Blind • Endoscopic • Flouroscopic • Patients with gastric intolerance • Patients with other risk factors – GERD – unable to nurse semi-recumbent • (eg. C-spine injury)
Discussion • Routine use: – Difficulties of SB access • Blind • Endoscopic • Flouroscopic • Patients with gastric intolerance • Patients with other risk factors – GERD – unable to nurse semi-recumbent • (eg. C-spine injury)
 Discussion • If your unit has feasible access – Go for it • If your unit has ability with effort – Use it for patients at risk • i. e. inotropes, sedatives, paralytics, high GRV’s • If your unit has great difficulty – Use in patients who do not tolerate gastric feeding
Discussion • If your unit has feasible access – Go for it • If your unit has ability with effort – Use it for patients at risk • i. e. inotropes, sedatives, paralytics, high GRV’s • If your unit has great difficulty – Use in patients who do not tolerate gastric feeding
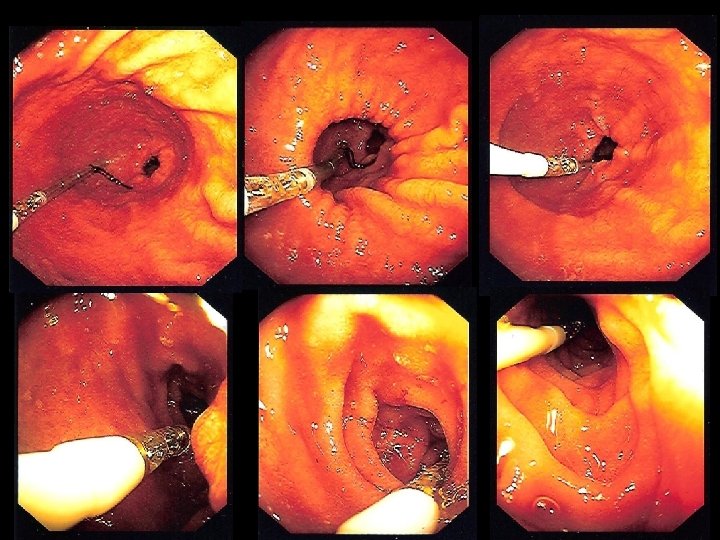
 Bedside placement into SB • Feeding tube in stomach • Wire with 30 o bend, 3 cm from end • Zaloga, Chest 1991 • Insufflate stomach with ~500 ml • Salasidis, CCM 1998 • Rotate while advancing • Samis and Drover, ICM 2004
Bedside placement into SB • Feeding tube in stomach • Wire with 30 o bend, 3 cm from end • Zaloga, Chest 1991 • Insufflate stomach with ~500 ml • Salasidis, CCM 1998 • Rotate while advancing • Samis and Drover, ICM 2004
 Thank You! • Choosing an approach to: • MAXIMIZE BENEFIT • Minimize risk
Thank You! • Choosing an approach to: • MAXIMIZE BENEFIT • Minimize risk