daa43a5bf562b86c5417784fdfcde119.ppt
- Количество слайдов: 19



Population Health and Policy review for Republic of Kazakhstan Madina Takenova Kazakhstan School of Public Health Kazakhstan APACPH conference Early career networkshop November 19 -23, 2005 Taipei

Republic of Kazakhstan Population – 15, 072 million Territory – 2724. 9 thousand km 2 Capital –Astana 57% urban population, 43% rural
, 1965 -2004 Life expectancy at birth, Kazakhstan, 1965")
Demographic situation in Kazakhstan (per 1000), 1965 -2004 Life expectancy at birth, Kazakhstan, 1965 -2004

Leading causes of morbidity and mortality in Kazakhstan • Overall morbidity – 99 627, 7 per 100 000 in 2004 • Morbidity incidence : I place- Diseases of respiratory system, CV diseases; III – Urogenital diseases • Mortality: Cardiovascular diseases, Neoplasms, Trauma & poisoning

Reproductive health • Infant mortality – 14, 5 per 1000 newborns • MMR is highest among CA countries – 36. 9 per 100, 000 livebirths • High rate of pregnancy and delivery complications – 60% • Contraceptive prevalence rate on rise – 50. 7 (Mo. H, 2002) • During 10 years the absolute amount of abortions in RK decreased by 2. 3 times • Unmet need for family planning – 8. 7% (DHS, 1999) • Access and quality of reproductive health services poor in rural areas
 15, 5 15, 01")
Main health and socio-economic indicators 1998 2004 Total population (million) 15, 5 15, 01 0, 742 0. 76 Life expectancy at birth 65 66, 14 Population growth rate 4, 4 7, 9 Birth rate per 1000 14. 8 18, 1 Death rate per 1000 10, 2 Live births per 1000 population 14, 8 15, 3 Infant mortality Rate per 1000 live births 21, 4 14, 5 Total Fertility rate 2 2, 2 Maternal mortality (per 100000 live births) 59 36. 9 Under-5 mortality rate (BUCEN) per 1000 live births 35, 2 69, 6 TB incidence per 100 000 (all forms) 118. 8 154, 3 299 698 Human development Index (HDI) HIV prevalence GDP per capita, $US 1497, 2 1995, 4 total allocations for health care, % of GDP 2 2, 61 correlation btw highest income h/hold and lowest income quintile 6 8

Trends of Tuberculosis in Kazakhstan

TB urgent issues • Social factor – interrupted treatment, – MDR TB (1500 cases in 2003; 56. 4% previously treated resistant for 2 or >) • TB in prisons, amnesty (incidence 30 times higher, mortality 9 times higher among imprisoned population); 8726 detainees with TB in KZ, 452 with MDR TB • TB and HIV/AIDS – 99 per 100000 cases of TB HIV+ • Young TB – 15 -18 years of age (yearly 1300 teenagers get infected by TB, 60% in families); 1990 - 57. 1 – 2000 -162. 2 per 100000 population
, including 272")
HIV/AIDS in Kazakhstan • June 2005 - officially 5008 HIV+ (699 cases), including 272 with AIDS. Men -76% (3823) Women - 24% (1185) • Estimated number of HIV+ people is 13, 000 (according to Sentinel Surveillance data) • Registered drug users – 45000; alleged IVDU -250 000 • AIDS death rate 31. 3 (220) • Transmission way: 76. 6% - parenteral; 14. 6% - sexual • Trends • HIV/AIDS epidemics is at concentrated stage - prevalence rate among risk groups (IVDUs and CSWs) is steadily above 5%. • There is a trend of sexual transmission rate increase : 2001 - 5%, 2002 - 16, 7%, 2003 - 21, 0%, 2004 - 29, 3%.

HIV transmission patterns dynamic

Prognosis for HIV infection in case of untimely activities Sanigest Internacional 2004

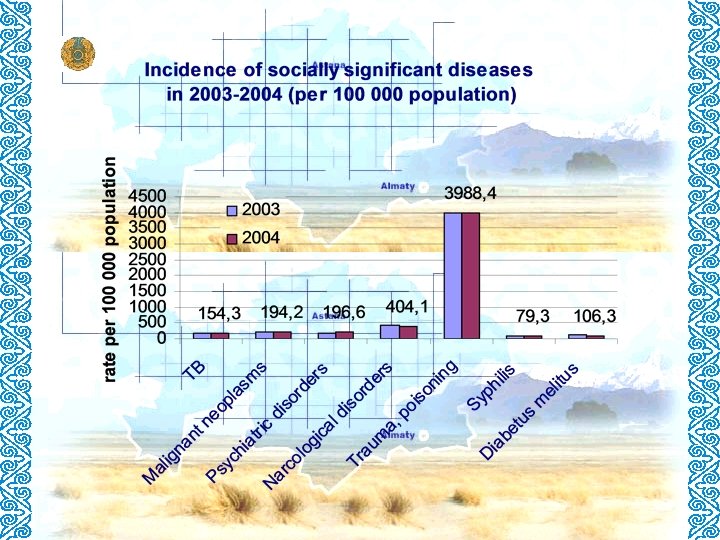
Emerging issues of population health 1. Increase of socially significant diseases 1. TB morbidity increased more than twice 2. STD 3. HIV/AIDS 2. Risk factors -smoking (for 1/3 of population); alcohol consumption, drug use 3. Unhealthy lifestyle, lack of health education and self motivation, 4. Reproductive health 5. Environmental pollution; 6. Lack of financing of medical institutions

Causes of unfavorable health status of population • Weak preventive activities of PH policy • Poor attitude & lake of skills toward own health • Ineffective intersectoral collaboration on PH issues • Social and economical troubles of transition period

National policy on population health & development • • • Developmental strategy “Kazakhstan-2030” “National Program of Health Sector Reform and Development in the Republic of Kazakhstan for 20052010” Program & Law “On health care system of the Republic of Kazakhstan” State programme “Population health” -November 1998 National network on health protection and (1998)

National Program of Health Sector Reform and Development in the Republic of Kazakhstan for 2005 -2010 • Developer: Ministry of Health • Timeframe: 2005 -2010 – 2 steps of implementation : 2005 -2007; 2008 -2010 • Required resources and sources of funds: – Central and local budgets, as well as other resources allowed by Law of the Republic of Kazakhstan; – In 2008 -2010 there will be an annual increase in health care financing and by 2010 it will increase to 4% of GDP

National Program of Health Sector Reform and Development in the Republic of Kazakhstan for 2005 -2010 • Objective • to create an effective health care delivery system based on the principles of solidarity of the state and individuals assuming responsibility for health protection, priority development of primary health care aimed at improving the health of population.

National Program of Health Sector Reform and Development in the Republic of Kazakhstan for 2005 -2010 • • Priority tasks: Real shift of focus to Primary health care; shift of emphasis from inpatient to outpatient care; Systemic transition to international standards, new technologies, advanced treatment methods and medical service; Strengthening of maternal/ child health; Creating a system of independent expertise involving independent experts; Training of health care system, health resource and finance managers; Prevention, diagnosis and treatment of socially significant diseases; Strengthening the technical/ material base of health facilities;

Expected outcomes of Programme • As a result of Program implementation, the optimal health care model satisfying needs of the people, the sector and the state will be created…
daa43a5bf562b86c5417784fdfcde119.ppt