

A Nimmo FARC Kazan Sept 2014.ppt
- Количество слайдов: 75
 Point of Care Testing of Haemostasis in the Operating Room - Rapid Diagnosis and Targeted Therapy Dr Alastair Nimmo Dept of Anaesthesia, Royal Infirmary of Edinburgh
Point of Care Testing of Haemostasis in the Operating Room - Rapid Diagnosis and Targeted Therapy Dr Alastair Nimmo Dept of Anaesthesia, Royal Infirmary of Edinburgh
 testing of haemostasis valuable") 1. My background 2. Why is point of care (POC) testing of haemostasis valuable in bleeding surgical, trauma and obstetric patients 3. Types of POC testing of haemostasis that are available
1. My background 2. Why is point of care (POC) testing of haemostasis valuable in bleeding surgical, trauma and obstetric patients 3. Types of POC testing of haemostasis that are available
 testing of haemostasis valuable") 1. My background 2. Why is point of care (POC) testing of haemostasis valuable in bleeding surgical, trauma and obstetric patients 3. Types of POC testing of haemostasis that are available
1. My background 2. Why is point of care (POC) testing of haemostasis valuable in bleeding surgical, trauma and obstetric patients 3. Types of POC testing of haemostasis that are available
 My background • My main job is as an anaesthesiologist • I also work for the Scottish National Blood Transfusion Service to promote blood conservation and the safe and effective use of blood products
My background • My main job is as an anaesthesiologist • I also work for the Scottish National Blood Transfusion Service to promote blood conservation and the safe and effective use of blood products
 Conflicts of interest • Travel expenses for meetings about coagulation; speaker fees – TEM International • Research funding – CSL Behring
Conflicts of interest • Travel expenses for meetings about coagulation; speaker fees – TEM International • Research funding – CSL Behring
 for •") Royal Infirmary of Edinburgh 24 operating rooms Scottish centre (5 million population) for • thoraco-abdominal aortic aneurysm surgery • liver and pancreas transplants Regional centre for • cardiac & thoracic surgery • vascular surgery • hepatobiliary surgery; renal transplants • major trauma • high risk obstetrics
Royal Infirmary of Edinburgh 24 operating rooms Scottish centre (5 million population) for • thoraco-abdominal aortic aneurysm surgery • liver and pancreas transplants Regional centre for • cardiac & thoracic surgery • vascular surgery • hepatobiliary surgery; renal transplants • major trauma • high risk obstetrics
 Royal Infirmary of Edinburgh 24 operating rooms Scottish centre for • thoraco-abdominal aortic aneurysm surgery • liver and pancreas transplants Regional centre for • cardiac & thoracic surgery • vascular surgery • hepatobiliary surgery; renal transplants • major trauma • high risk obstetrics
Royal Infirmary of Edinburgh 24 operating rooms Scottish centre for • thoraco-abdominal aortic aneurysm surgery • liver and pancreas transplants Regional centre for • cardiac & thoracic surgery • vascular surgery • hepatobiliary surgery; renal transplants • major trauma • high risk obstetrics
 testing of haemostasis valuable") 1. My background 2. Why is point of care (POC) testing of haemostasis valuable in bleeding surgical, trauma and obstetric patients 3. Types of POC testing of haemostasis that are available
1. My background 2. Why is point of care (POC) testing of haemostasis valuable in bleeding surgical, trauma and obstetric patients 3. Types of POC testing of haemostasis that are available
 Why POC tests instead of lab tests? 1. Turnaround time • Coagulation is a dynamic phenomenon great changes may occur within a few minutes in patients undergoing major surgery • Treatment given blindly or on the basis of “old” lab results - is often ineffective - may also result in potentially harmful blood products being given unnecessarily
Why POC tests instead of lab tests? 1. Turnaround time • Coagulation is a dynamic phenomenon great changes may occur within a few minutes in patients undergoing major surgery • Treatment given blindly or on the basis of “old” lab results - is often ineffective - may also result in potentially harmful blood products being given unnecessarily
 Why POC tests instead of lab tests? 2. Standard laboratory tests don’t provide important information on: • Excessive fibrinolysis (D-dimer or FDPs are indirect measures, reflecting past rather than current events) • Platelet dysfunction e. g. due to aspirin and clopidogrel
Why POC tests instead of lab tests? 2. Standard laboratory tests don’t provide important information on: • Excessive fibrinolysis (D-dimer or FDPs are indirect measures, reflecting past rather than current events) • Platelet dysfunction e. g. due to aspirin and clopidogrel
 Why I use POC testing of haemostasis • It enables me to rapidly diagnose and correct abnormalities of haemostasis in bleeding surgical and trauama patients – even with massive haemorrhage. • It enables me to give appropriate targeted treatment but avoid unnecessary transfusions.
Why I use POC testing of haemostasis • It enables me to rapidly diagnose and correct abnormalities of haemostasis in bleeding surgical and trauama patients – even with massive haemorrhage. • It enables me to give appropriate targeted treatment but avoid unnecessary transfusions.
 A clinical example AAA 02. ppt
A clinical example AAA 02. ppt
 Just after midnight • Elderly patient in the Emergency Room • Abdominal & back pain and collapse at home • Unrecordable BP & conscious level • Too obese to palpate anything on abdominal examination but presumed diagnosis is ruptured aortic aneurysm
Just after midnight • Elderly patient in the Emergency Room • Abdominal & back pain and collapse at home • Unrecordable BP & conscious level • Too obese to palpate anything on abdominal examination but presumed diagnosis is ruptured aortic aneurysm
 On arrival in operating room • • Obese patient with short thick neck Blood Pressure 40/30 No response to jaw thrust Poor veins - two small(18 G) IV cannulae in the feet
On arrival in operating room • • Obese patient with short thick neck Blood Pressure 40/30 No response to jaw thrust Poor veins - two small(18 G) IV cannulae in the feet
 Initial management • Red cells, FFP and platelets obtained • Red cells given from rapid fluid infusers via the two cannulae in the feet • Anaesthesia & start of surgery • One 18 G cannula inserted in arm • Very difficult to find and clamp aorta because of obesity • Large central venous catheter inserted
Initial management • Red cells, FFP and platelets obtained • Red cells given from rapid fluid infusers via the two cannulae in the feet • Anaesthesia & start of surgery • One 18 G cannula inserted in arm • Very difficult to find and clamp aorta because of obesity • Large central venous catheter inserted
 Hb 8. 9,") Blood results & blood loss • Emergency room (phoned during surgery) Hb 8. 9, Platelets 82 PT 26 (ratio 2. 5), Fibrinogen 0. 4 • Blood gases at start of surgery H+ 128, Base Excess -21. 2, Lactate 14. 3 • TUBE GRAFT REPAIR OF ANEURYSM • Measured blood loss 15 500 ml • Surgical assessment - “bleeding from everywhere”
Blood results & blood loss • Emergency room (phoned during surgery) Hb 8. 9, Platelets 82 PT 26 (ratio 2. 5), Fibrinogen 0. 4 • Blood gases at start of surgery H+ 128, Base Excess -21. 2, Lactate 14. 3 • TUBE GRAFT REPAIR OF ANEURYSM • Measured blood loss 15 500 ml • Surgical assessment - “bleeding from everywhere”
 After admission to ITU • BP 120/70, passing urine • H+ 50, BE -3. 6, Lactate 8. 95 (soon to 2) • Hb 8. 8, Platelets 111 PT 10 (ratio 1. 2), Fibrinogen 1. 9 • No further blood products given in the first 24 hours on ICU; one unit of red cells given on 2 nd post-op day • Full (but slow) recovery
After admission to ITU • BP 120/70, passing urine • H+ 50, BE -3. 6, Lactate 8. 95 (soon to 2) • Hb 8. 8, Platelets 111 PT 10 (ratio 1. 2), Fibrinogen 1. 9 • No further blood products given in the first 24 hours on ICU; one unit of red cells given on 2 nd post-op day • Full (but slow) recovery
 Teamwork and technology
Teamwork and technology
 After admission to ITU • BP 120/70, passing urine • H+ 50, BE -3. 6, Lactate 8. 95 ( to 2) • Hb 8. 8, Platelets 111 PT 10 (ratio 1. 2), Fibrinogen 1. 9 • There were no laboratory tests performed during surgery – only point of care testing
After admission to ITU • BP 120/70, passing urine • H+ 50, BE -3. 6, Lactate 8. 95 ( to 2) • Hb 8. 8, Platelets 111 PT 10 (ratio 1. 2), Fibrinogen 1. 9 • There were no laboratory tests performed during surgery – only point of care testing
 testing of haemostasis valuable") 1. My background 2. Why is point of care (POC) testing of haemostasis valuable in bleeding surgical, trauma and obstetric patients 3. Types of POC testing of haemostasis that are available
1. My background 2. Why is point of care (POC) testing of haemostasis valuable in bleeding surgical, trauma and obstetric patients 3. Types of POC testing of haemostasis that are available
 Point-of-care haemostasis analysers 1. Coagulation time analysers - PT, APTT, ACT 2. “Viscoelastic” whole-blood analysers - thromboelastography / thromboelastometry 3. Platelet function analysers (aspirin, clopidogrel)
Point-of-care haemostasis analysers 1. Coagulation time analysers - PT, APTT, ACT 2. “Viscoelastic” whole-blood analysers - thromboelastography / thromboelastometry 3. Platelet function analysers (aspirin, clopidogrel)

 1. Coagulation time analysers • Tube-based - ACT • Cuvette-based - ACT - APTT - PT Useful for measuring the effect of unfractionated heparin and coumarin anticoagulants
1. Coagulation time analysers • Tube-based - ACT • Cuvette-based - ACT - APTT - PT Useful for measuring the effect of unfractionated heparin and coumarin anticoagulants
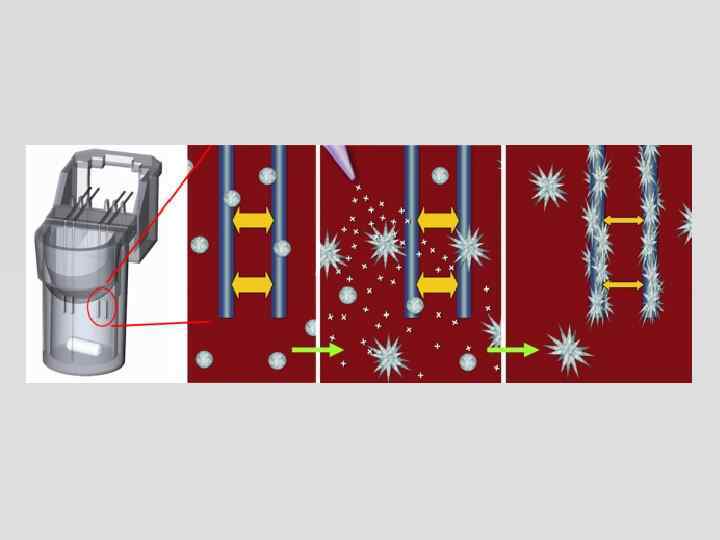
 2. thromboelastography / thromboelastometry • “viscoelastic” test of whole blood coagulation • provides information on onset of coagulation, development of clot strength, maximum clot strength and clot lysis
2. thromboelastography / thromboelastometry • “viscoelastic” test of whole blood coagulation • provides information on onset of coagulation, development of clot strength, maximum clot strength and clot lysis
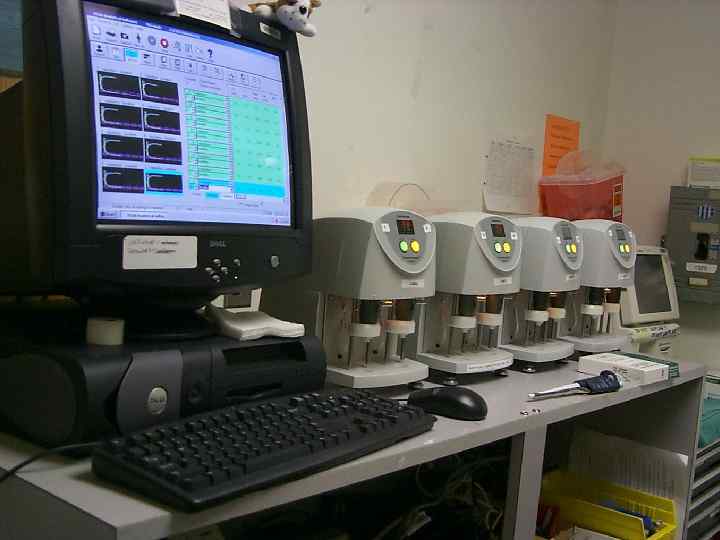
 Thromboelastography / thromboelastometry • Two analysers based on the same principle from two different companies TEG® Haemonetics, Braintree, MA, USA ROTEM ® TEM International, Munich, Germany
Thromboelastography / thromboelastometry • Two analysers based on the same principle from two different companies TEG® Haemonetics, Braintree, MA, USA ROTEM ® TEM International, Munich, Germany
 thromboelastography / thromboelastometry • provides information on onset of coagulation, development of clot strength, maximum clot strength and clot lysis • permits rapid identification of: - thrombocytopenia / platelet dysfunction* - low fibrinogen / impaired fibrin polymerisation - low coagulation factor levels - heparin effect - hyperfibrinolysis Useful for measuring the cause of acquired disorders of haemostasis during surgery, after trauma, after childbirth *but standard tests don’t show aspirin / clopidogrel effects
thromboelastography / thromboelastometry • provides information on onset of coagulation, development of clot strength, maximum clot strength and clot lysis • permits rapid identification of: - thrombocytopenia / platelet dysfunction* - low fibrinogen / impaired fibrin polymerisation - low coagulation factor levels - heparin effect - hyperfibrinolysis Useful for measuring the cause of acquired disorders of haemostasis during surgery, after trauma, after childbirth *but standard tests don’t show aspirin / clopidogrel effects
 3. Platelet function analysers Use anticoagulated whole blood samples. Measure platelet aggregation in response to agonists: • Light transmittance aggregometry -Verify. Now® • Impedance aggregometry - Multiplate®, ROTEM platelet®) • Platelet count before & after agonist-Plateletworks® • Thromboelastography –TEG® Platelet. Mapping ® • Time taken for platelets to block an aperture in a membrane - PFA-100® Useful for measuring the effect of antiplatelet drugs e. g. aspirin, clopidogrel
3. Platelet function analysers Use anticoagulated whole blood samples. Measure platelet aggregation in response to agonists: • Light transmittance aggregometry -Verify. Now® • Impedance aggregometry - Multiplate®, ROTEM platelet®) • Platelet count before & after agonist-Plateletworks® • Thromboelastography –TEG® Platelet. Mapping ® • Time taken for platelets to block an aperture in a membrane - PFA-100® Useful for measuring the effect of antiplatelet drugs e. g. aspirin, clopidogrel
 Point-of-care haemostasis analysers 1. Coagulation time analysers - PT, APTT, ACT anticoagulants 2. “Viscoelastic” whole-blood analysers - thromboelastography / thromboelastometry most causes of impaired haemostasis that occur during surgery, and after trauma and childbirth 3. Platelet function analysers (aspirin, clopidogrel) antiplatelet drugs
Point-of-care haemostasis analysers 1. Coagulation time analysers - PT, APTT, ACT anticoagulants 2. “Viscoelastic” whole-blood analysers - thromboelastography / thromboelastometry most causes of impaired haemostasis that occur during surgery, and after trauma and childbirth 3. Platelet function analysers (aspirin, clopidogrel) antiplatelet drugs
 Thromboelastography / thromboelastometry • Two analysers based on the same principle from two different companies TEG® Haemonetics, Braintree, MA, USA ROTEM ® TEM International, Munich, Germany
Thromboelastography / thromboelastometry • Two analysers based on the same principle from two different companies TEG® Haemonetics, Braintree, MA, USA ROTEM ® TEM International, Munich, Germany
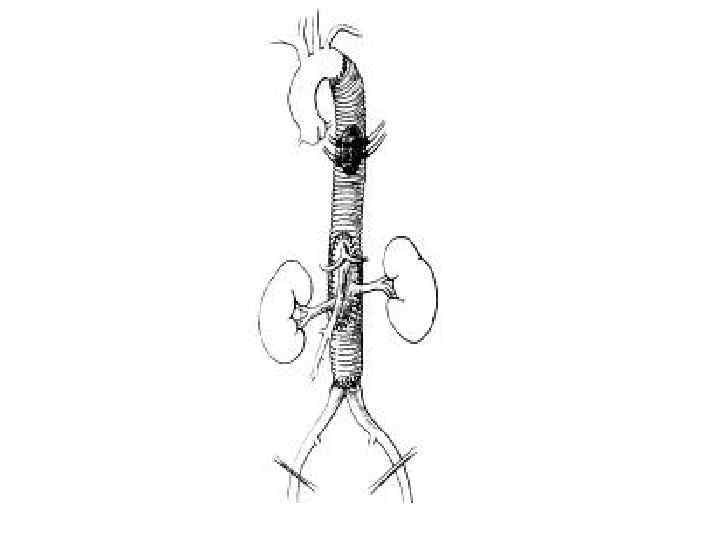
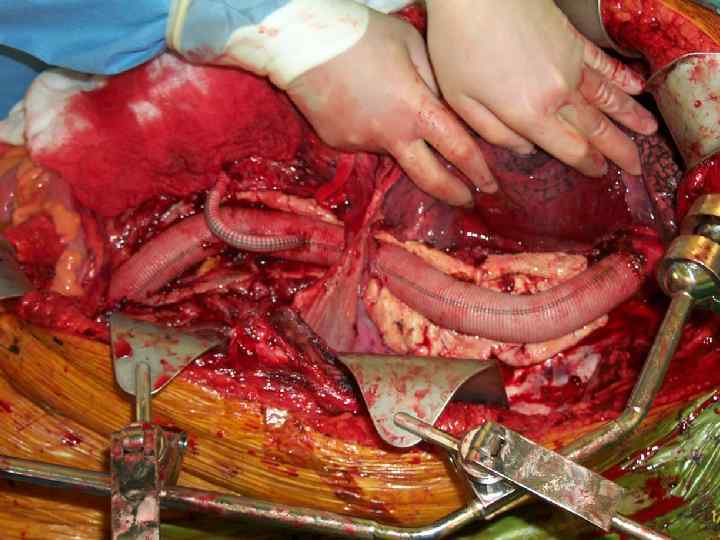
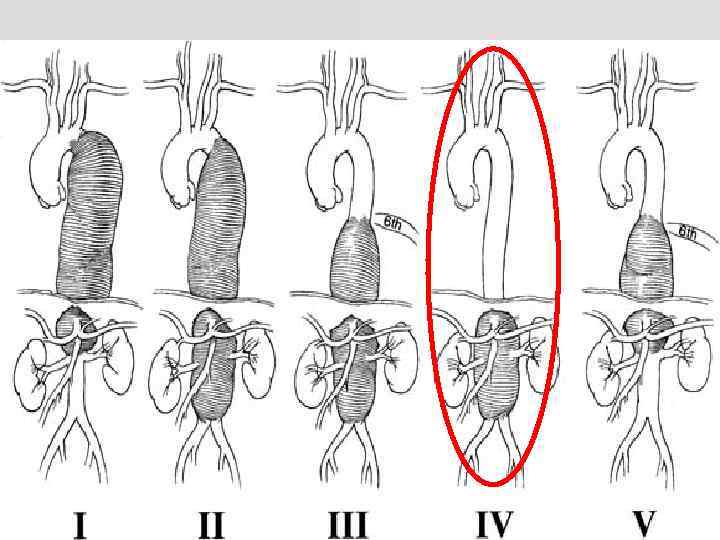
") Thoraco-abdominal aortic aneurysms (TAAA)
Thoraco-abdominal aortic aneurysms (TAAA)

 35
35
 Management of haemostasis during TAAA repair Until 2001 • Use of standard laboratory tests and clinical judgement • Major difficulties with correcting haemostasis and with continued postoperative bleeding Since 2001 • Point of care testing with ROTEM® • Impaired haemostasis at the end of surgery rare “Like night and day”
Management of haemostasis during TAAA repair Until 2001 • Use of standard laboratory tests and clinical judgement • Major difficulties with correcting haemostasis and with continued postoperative bleeding Since 2001 • Point of care testing with ROTEM® • Impaired haemostasis at the end of surgery rare “Like night and day”
 10 consecutive Extent 4 TAAA repairs* Case Blood Given during surgery loss Red Platelets FFP Hb (ml) cells (pools) (units) Post-op blood results Platelet count Fibrinogen PT APTT (g/l) ratio (units) 1 11 300 2 1 8 105 89 1. 4 1. 2 0. 8 2 5 500 5 0 4 98 100 1. 6 1. 2 3 4 3 200 13 600 6 6 0 2 4 16 90 87 76 58 1. 4 1. 2 1. 3 1. 1 1. 0 5 11 800 5 3 8 78 71 1. 4 1. 1 6 7 200 6 3 12 93 70 1. 7 1. 2 1. 0 7 16 000 7 5 12 108 104 1. 8 1. 2 8 9 10 4 300 8 000 6 2 4 0 0 0 8 6 8 90 53 83 93 1. 6 1. 4 1. 6 1. 2 1. 4 1. 2 1. 0 1. 2 1. 0 86 83 *no laboratory tests were performed during surgery
10 consecutive Extent 4 TAAA repairs* Case Blood Given during surgery loss Red Platelets FFP Hb (ml) cells (pools) (units) Post-op blood results Platelet count Fibrinogen PT APTT (g/l) ratio (units) 1 11 300 2 1 8 105 89 1. 4 1. 2 0. 8 2 5 500 5 0 4 98 100 1. 6 1. 2 3 4 3 200 13 600 6 6 0 2 4 16 90 87 76 58 1. 4 1. 2 1. 3 1. 1 1. 0 5 11 800 5 3 8 78 71 1. 4 1. 1 6 7 200 6 3 12 93 70 1. 7 1. 2 1. 0 7 16 000 7 5 12 108 104 1. 8 1. 2 8 9 10 4 300 8 000 6 2 4 0 0 0 8 6 8 90 53 83 93 1. 6 1. 4 1. 6 1. 2 1. 4 1. 2 1. 0 1. 2 1. 0 86 83 *no laboratory tests were performed during surgery
 Extent 4 TAAA Repair – 19 consecutive cases
Extent 4 TAAA Repair – 19 consecutive cases
 Expansion of ROTEM® use in my hospital 2001 – Vascular surgery 2002 – Emergency and trauma surgery 2005 – Liver transplants and major hepatic surgery 2009 – Obstetrics – postpartum haemorrhage 2010 – Major orthopaedic surgery (scoliosis) 2011 – Cardiac surgery Now 11 ROTEM analysers and over 30 of the anaesthetic nurses are trained to use them.
Expansion of ROTEM® use in my hospital 2001 – Vascular surgery 2002 – Emergency and trauma surgery 2005 – Liver transplants and major hepatic surgery 2009 – Obstetrics – postpartum haemorrhage 2010 – Major orthopaedic surgery (scoliosis) 2011 – Cardiac surgery Now 11 ROTEM analysers and over 30 of the anaesthetic nurses are trained to use them.
 H. Hartet 1948") Thromboelastography (TEG®) H. Hartet 1948
Thromboelastography (TEG®) H. Hartet 1948
 ROTEM® A. Calatzis 1996") Rotational thromboelastometry (rotational thromboelastography) ROTEM® A. Calatzis 1996
Rotational thromboelastometry (rotational thromboelastography) ROTEM® A. Calatzis 1996
 ROTEM® - samples & tests • • activator of coagulation + inhibitor of heparin + inhibitor of platelet aggregation + inhibitor of fibrinolysis
ROTEM® - samples & tests • • activator of coagulation + inhibitor of heparin + inhibitor of platelet aggregation + inhibitor of fibrinolysis
 4 different tests on one blood sample Normal
4 different tests on one blood sample Normal
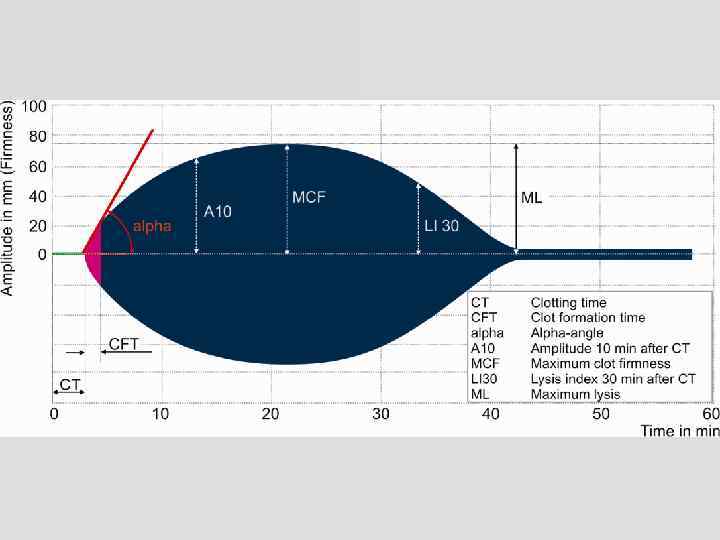
 ROTEM® interpretation made easy! You only have to look at two numbers 1. MCF or A 10 2. CT Ignore the other numbers!
ROTEM® interpretation made easy! You only have to look at two numbers 1. MCF or A 10 2. CT Ignore the other numbers!
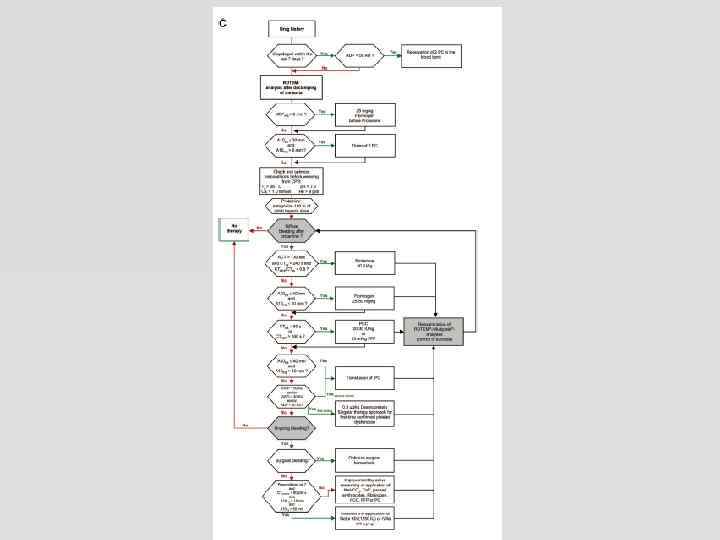
 ROTEM® - interpretation 3 questions 1. Is the firmness / strength of the clot reduced (middle of trace) platelets and fibrinogen 2. Does it take too long for detectable clot to form (first part of trace) coagulation factors & anticoagulants 3. Does the clot break down after it has formed (latter part of trace) excessive fibrinolysis
ROTEM® - interpretation 3 questions 1. Is the firmness / strength of the clot reduced (middle of trace) platelets and fibrinogen 2. Does it take too long for detectable clot to form (first part of trace) coagulation factors & anticoagulants 3. Does the clot break down after it has formed (latter part of trace) excessive fibrinolysis
 Veklich Y, Weisel JW. NATURE 2001; 413: 6855
Veklich Y, Weisel JW. NATURE 2001; 413: 6855
") FIBTEM EXTEM activator plus Cytochalasin D (inhibitor of platelet aggregation)
FIBTEM EXTEM activator plus Cytochalasin D (inhibitor of platelet aggregation)
 CLOT FIRMNESS <5 mm 5 -7 A 10 in FIBTEM mm >8 mm A 10 in EXTEM / INTEM / HEPTEM / APTEM < 22 mm 22 -38 mm > 39 mm Low fibrinogen Low platelets Low fibrinogen (*platelets - see below) Low platelets Low fibrinogen Clot firmness appears satisfactory * Typically fibrinogen < 1. 5 g/l & platelets 50 -100. Also consider giving platelets if ongoing bleeding From: ROTEM® guidelines: surgery, trauma & obstetrics Author: Alastair Nimmo Version 2. 2 Modified 24
CLOT FIRMNESS <5 mm 5 -7 A 10 in FIBTEM mm >8 mm A 10 in EXTEM / INTEM / HEPTEM / APTEM < 22 mm 22 -38 mm > 39 mm Low fibrinogen Low platelets Low fibrinogen (*platelets - see below) Low platelets Low fibrinogen Clot firmness appears satisfactory * Typically fibrinogen < 1. 5 g/l & platelets 50 -100. Also consider giving platelets if ongoing bleeding From: ROTEM® guidelines: surgery, trauma & obstetrics Author: Alastair Nimmo Version 2. 2 Modified 24
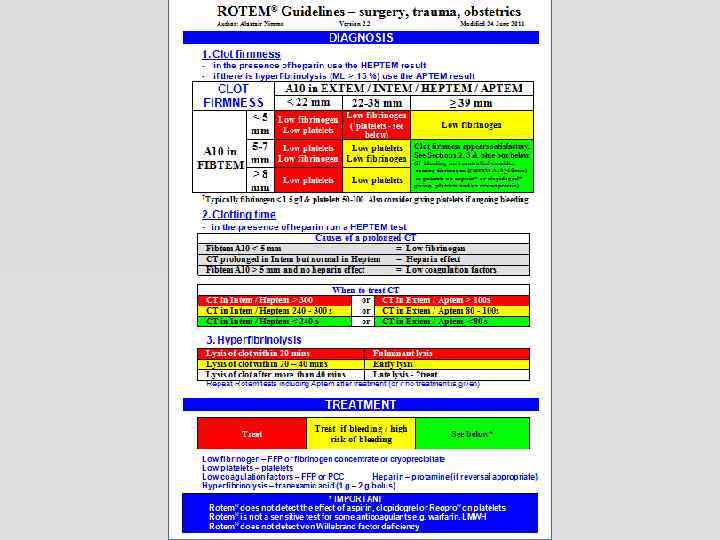
 Latter part of the trace – clot stability Measures fibrinolysis
Latter part of the trace – clot stability Measures fibrinolysis
 Another ruptured AAA - pre-op sample
Another ruptured AAA - pre-op sample
 5 minutes after aortic clamping
5 minutes after aortic clamping
 After aprotinin
After aprotinin
 Post-partum haemorrhage Ex. TEM CT = 161 A 10 = 0 In. TEM CFT = -MCF = 12 CT = 275 A 10 = 0 ML = 100 Ap. TEM Fib. TEM CT = *2506 A 10 = -- CFT = -MCF = -ML = -- CFT = -MCF = 8 CT = 181 A 10 = 28 CFT = 352 MCF = *40 ML = *0
Post-partum haemorrhage Ex. TEM CT = 161 A 10 = 0 In. TEM CFT = -MCF = 12 CT = 275 A 10 = 0 ML = 100 Ap. TEM Fib. TEM CT = *2506 A 10 = -- CFT = -MCF = -ML = -- CFT = -MCF = 8 CT = 181 A 10 = 28 CFT = 352 MCF = *40 ML = *0
 After tranexamic acid Ex. TEM CT = 244 A 10 = 18 In. TEM CFT = 720 MCF = *28 CT = 309 A 10 = 21 ML = *0 Ap. TEM Fib. TEM CT = 494 A 10 = 3 CFT = -MCF = 3 ML = *15 CFT = 524 MCF = *29 CT = 238 A 10 = 18 CFT = 725 MCF = *27 ML = *0
After tranexamic acid Ex. TEM CT = 244 A 10 = 18 In. TEM CFT = 720 MCF = *28 CT = 309 A 10 = 21 ML = *0 Ap. TEM Fib. TEM CT = 494 A 10 = 3 CFT = -MCF = 3 ML = *15 CFT = 524 MCF = *29 CT = 238 A 10 = 18 CFT = 725 MCF = *27 ML = *0
 CLOT FIRMNESS <5 mm 5 -7 A 10 in FIBTEM mm >8 mm A 10 in EXTEM / INTEM / HEPTEM / APTEM < 22 mm 22 -38 mm > 39 mm Low fibrinogen Low platelets Low fibrinogen (*platelets - see below) Low platelets Low fibrinogen Clot firmness appears satisfactory * Typically fibrinogen < 1. 5 g/l & platelets 50 -100. Also consider giving platelets if ongoing bleeding From: ROTEM® guidelines: surgery, trauma & obstetrics Author: Alastair Nimmo Version 2. 2 Modified 24
CLOT FIRMNESS <5 mm 5 -7 A 10 in FIBTEM mm >8 mm A 10 in EXTEM / INTEM / HEPTEM / APTEM < 22 mm 22 -38 mm > 39 mm Low fibrinogen Low platelets Low fibrinogen (*platelets - see below) Low platelets Low fibrinogen Clot firmness appears satisfactory * Typically fibrinogen < 1. 5 g/l & platelets 50 -100. Also consider giving platelets if ongoing bleeding From: ROTEM® guidelines: surgery, trauma & obstetrics Author: Alastair Nimmo Version 2. 2 Modified 24
 Ex. TEM CT = 41 A 10 = 33 In. TEM CFT = 284 MCF = 47 CT = 212 A 10 = 33 ML = *0 ML = *1 Ap. TEM Fib. TEM CT = 50 A 10 = 10 CFT = -MCF = 11 ML = *3 CFT = 230 MCF = 45 CT = 47 A 10 = 32 CFT = 293 MCF = 47 ML = *1
Ex. TEM CT = 41 A 10 = 33 In. TEM CFT = 284 MCF = 47 CT = 212 A 10 = 33 ML = *0 ML = *1 Ap. TEM Fib. TEM CT = 50 A 10 = 10 CFT = -MCF = 11 ML = *3 CFT = 230 MCF = 45 CT = 47 A 10 = 32 CFT = 293 MCF = 47 ML = *1
 CLOT FIRMNESS <5 mm 5 -7 A 10 in FIBTEM mm >8 mm A 10 in EXTEM / INTEM / HEPTEM / APTEM < 22 mm 22 -38 mm > 39 mm Low fibrinogen Low platelets Low fibrinogen (*platelets - see below) Low platelets Low fibrinogen Clot firmness appears satisfactory * Typically fibrinogen < 1. 5 g/l & platelets 50 -100. Also consider giving platelets if ongoing bleeding From: ROTEM® guidelines: surgery, trauma & obstetrics Author: Alastair Nimmo Version 2. 2 Modified 24
CLOT FIRMNESS <5 mm 5 -7 A 10 in FIBTEM mm >8 mm A 10 in EXTEM / INTEM / HEPTEM / APTEM < 22 mm 22 -38 mm > 39 mm Low fibrinogen Low platelets Low fibrinogen (*platelets - see below) Low platelets Low fibrinogen Clot firmness appears satisfactory * Typically fibrinogen < 1. 5 g/l & platelets 50 -100. Also consider giving platelets if ongoing bleeding From: ROTEM® guidelines: surgery, trauma & obstetrics Author: Alastair Nimmo Version 2. 2 Modified 24
 3. Platelet function analysers Use anticoagulated whole blood samples. Measure platelet aggregation in response to agonists: • Light transmittance aggregometry -Verify. Now® • Impedance aggregometry - Multiplate®, ROTEM platelet®) • Platelet count before & after agonist-Plateletworks® • Thromboelastography –TEG® Platelet. Mapping ® • Time taken for platelets to block an aperture in a membrane - PFA-100® Useful for measuring the effect of antiplatelet drugs e. g. aspirin, clopidogrel
3. Platelet function analysers Use anticoagulated whole blood samples. Measure platelet aggregation in response to agonists: • Light transmittance aggregometry -Verify. Now® • Impedance aggregometry - Multiplate®, ROTEM platelet®) • Platelet count before & after agonist-Plateletworks® • Thromboelastography –TEG® Platelet. Mapping ® • Time taken for platelets to block an aperture in a membrane - PFA-100® Useful for measuring the effect of antiplatelet drugs e. g. aspirin, clopidogrel
 Multiplate® analyser multiple platelet function analyzer § Impedance aggregometry § 5 independent channels
Multiplate® analyser multiple platelet function analyzer § Impedance aggregometry § 5 independent channels
 TRAPtest ASPItest ADPtest HS normal aggregation 113 U 102 U 89 U 81 U 134 U 112 U 31 U 18 U 17 U 3 U 3 U 2 U 17 U 100 mg aspirin qd 139 U 75 mg clopidogrel qd 100 mg aspirin+ 75 mg clopidogrel qd 98 U 88 U 7 U Tirofiban i. v. 89 U
TRAPtest ASPItest ADPtest HS normal aggregation 113 U 102 U 89 U 81 U 134 U 112 U 31 U 18 U 17 U 3 U 3 U 2 U 17 U 100 mg aspirin qd 139 U 75 mg clopidogrel qd 100 mg aspirin+ 75 mg clopidogrel qd 98 U 88 U 7 U Tirofiban i. v. 89 U
 Preoperative Multiplate results in 100 patients having vascular surgery
Preoperative Multiplate results in 100 patients having vascular surgery
 Multiplate results in 100 patients having elective vascular surgery
Multiplate results in 100 patients having elective vascular surgery
 Pre-procedure Multiplate® results and bleeding in patients undergoing PCI Sibbing D, et al. J Thromb Haemost. 2010; 8: 250 -256.
Pre-procedure Multiplate® results and bleeding in patients undergoing PCI Sibbing D, et al. J Thromb Haemost. 2010; 8: 250 -256.
 Pre-op Multiplate® results and bleeding in patients undergoing cardiac surgery Ranucci M, et al. Ann Thorac Surg 2011; 91: 123– 30 Units for aggregation have been converted from those in the original paper by multiplying by 10.
Pre-op Multiplate® results and bleeding in patients undergoing cardiac surgery Ranucci M, et al. Ann Thorac Surg 2011; 91: 123– 30 Units for aggregation have been converted from those in the original paper by multiplying by 10.
 Suggested scheme for interpreting pre-op Multiplate® results in vascular surgery patients on clopidogrel ADP test result Platelet inhibition by clopidogrel Risk of excessive bleeding because of clopidogrel effect < 300 - 600 >600 High Marked Some Little or none Low Assumptions: • normal platelet count • hirudin anticoagulant used for the Multiplate®
Suggested scheme for interpreting pre-op Multiplate® results in vascular surgery patients on clopidogrel ADP test result Platelet inhibition by clopidogrel Risk of excessive bleeding because of clopidogrel effect < 300 - 600 >600 High Marked Some Little or none Low Assumptions: • normal platelet count • hirudin anticoagulant used for the Multiplate®
: 531 -47 • • • ROTEM® and Multiplate ® were") Anesthesiology. 2012 Sep; 117(3): 531 -47 • • • ROTEM® and Multiplate ® were used Fewer red cell transfusions Less postoperative bleeding Fewer FFP and platelet transfusions Fewer r. FVIIa administrations Better clinical outcomes
Anesthesiology. 2012 Sep; 117(3): 531 -47 • • • ROTEM® and Multiplate ® were used Fewer red cell transfusions Less postoperative bleeding Fewer FFP and platelet transfusions Fewer r. FVIIa administrations Better clinical outcomes
 Point of Care Testing of Haemostasis in the Operating Room - Rapid Diagnosis and Targeted Therapy Dr Alastair Nimmo Dept of Anaesthesia, Royal Infirmary of Edinburgh
Point of Care Testing of Haemostasis in the Operating Room - Rapid Diagnosis and Targeted Therapy Dr Alastair Nimmo Dept of Anaesthesia, Royal Infirmary of Edinburgh