

7d9ee6a536364936c65cde9fe95b4807.ppt
- Количество слайдов: 66
 Pediatric Pain Management: Meeting the Challenges Linda Oakes RN MSN C CCNS Pain Clinical Nurse Specialist St Jude Children’s Research Hospital November 2006
Pediatric Pain Management: Meeting the Challenges Linda Oakes RN MSN C CCNS Pain Clinical Nurse Specialist St Jude Children’s Research Hospital November 2006
 Greetings from St Jude Children’s Research Hospital: Memphis, Tennessee
Greetings from St Jude Children’s Research Hospital: Memphis, Tennessee
 To advocate for a patient in regards to pain is to…… • Believe the basic assumptions about pain assessment and management • Know how to assess pain including awareness of the challenges • Demonstrate how to ask for what the patient needs, provide it safely including teaching the patient and family
To advocate for a patient in regards to pain is to…… • Believe the basic assumptions about pain assessment and management • Know how to assess pain including awareness of the challenges • Demonstrate how to ask for what the patient needs, provide it safely including teaching the patient and family
 Being A Pain Advocate • Topic of pain values within yourself and your co-workers • Even if you are clear about how to manage pain, your patients, families, and colleagues will not always have the same perceptions • Pain management is saturated with: – Misinformation – Misled intentions (“quick fixes”)
Being A Pain Advocate • Topic of pain values within yourself and your co-workers • Even if you are clear about how to manage pain, your patients, families, and colleagues will not always have the same perceptions • Pain management is saturated with: – Misinformation – Misled intentions (“quick fixes”)
 Pain • An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage • International Association of Pain (1979)
Pain • An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage • International Association of Pain (1979)
 Pain Assessment • Whatever the experiencing person says it is, existing whenever the person says it does » Mc. Caffery (1968, 1999)
Pain Assessment • Whatever the experiencing person says it is, existing whenever the person says it does » Mc. Caffery (1968, 1999)
 Assumptions • All persons with pain deserve prompt recognition and treatment • Pain should be routinely monitored, assessed, reassessed, and documented clearly to facilitate treatment and communication among health care clinicians • Nurses are well positioned as patient advocates to something about the pain – Independent interventions – Interdependent interventions
Assumptions • All persons with pain deserve prompt recognition and treatment • Pain should be routinely monitored, assessed, reassessed, and documented clearly to facilitate treatment and communication among health care clinicians • Nurses are well positioned as patient advocates to something about the pain – Independent interventions – Interdependent interventions
 Ingredients to be Advocate • Recognition of pain • Courage to be present • Ability to “do battle” using the absolute best of their interpersonal skills • Empathy more than a judgmental attitude • Willingness to become educated about pain management American Society of Pain Management Nursing (ASPMN), 2002
Ingredients to be Advocate • Recognition of pain • Courage to be present • Ability to “do battle” using the absolute best of their interpersonal skills • Empathy more than a judgmental attitude • Willingness to become educated about pain management American Society of Pain Management Nursing (ASPMN), 2002
 What are the Challenges? • What is the right method? • How do we factor in the additional challenges of caring for: – – Different developmental stages? Individuality of pain expression: verbal and nonverbal? Different types of pain? Different cultures? • How do we use the pain assessment information? • Should assessment be the same for acute and chronic pain?
What are the Challenges? • What is the right method? • How do we factor in the additional challenges of caring for: – – Different developmental stages? Individuality of pain expression: verbal and nonverbal? Different types of pain? Different cultures? • How do we use the pain assessment information? • Should assessment be the same for acute and chronic pain?
 Do patients experience pain, including infants and children? • By 24 weeks gestation the pain pathways are able to provide sensory input regarding pain • First encounter with pain is the vitamin K injection ongoing pain experiences throughout life – Pain is usually helpful serving as a warning
Do patients experience pain, including infants and children? • By 24 weeks gestation the pain pathways are able to provide sensory input regarding pain • First encounter with pain is the vitamin K injection ongoing pain experiences throughout life – Pain is usually helpful serving as a warning
 Pain Literature • Wolfe et al, 2000, NEJM – 90% of children dying of cancer experience pain or other symptoms – Less than 40% had pain relief before they died – Dying children exposed to multiple painful procedures/therapies even as they are dying – Interviewed parents of children who died between 1990 -1997 in credible teaching/children’s hospital
Pain Literature • Wolfe et al, 2000, NEJM – 90% of children dying of cancer experience pain or other symptoms – Less than 40% had pain relief before they died – Dying children exposed to multiple painful procedures/therapies even as they are dying – Interviewed parents of children who died between 1990 -1997 in credible teaching/children’s hospital
 Advocacy in Assessment • Patient is the authority on his pain – Accept the report – Take appropriate action (avoiding an adversarial relationship) • Recognize that pain thresholds and levels of thresholds are variable • Patients will creatively adapt to pain in order to cope with its intensity and interference with function • Avoid “expected responses” for interventions
Advocacy in Assessment • Patient is the authority on his pain – Accept the report – Take appropriate action (avoiding an adversarial relationship) • Recognize that pain thresholds and levels of thresholds are variable • Patients will creatively adapt to pain in order to cope with its intensity and interference with function • Avoid “expected responses” for interventions
 Assessment: What is Known? • Children experience the pain as adults…if it is painful for adult, it is painful for child • Children are at risk for under treatment of pain because they do not have verbal skills to report pain may be overlooked • Children may fear reporting pain – Results in an injection – Have to stay in hospital longer – May be reluctant to complain (“disappoint their parents”) • Discrepancies in surrogate ratings of pain Zisk, 2003
Assessment: What is Known? • Children experience the pain as adults…if it is painful for adult, it is painful for child • Children are at risk for under treatment of pain because they do not have verbal skills to report pain may be overlooked • Children may fear reporting pain – Results in an injection – Have to stay in hospital longer – May be reluctant to complain (“disappoint their parents”) • Discrepancies in surrogate ratings of pain Zisk, 2003
 Developmental Aspects of Pain Expression • Infant: intense cry, unable to sleep or eat • Toddler: verbal or physical aggression or withdrawal, guarding the site or pain • Preschooler: can verbalize but much “magical thinking”, see pain as punishment • School-age: can verbalize but very influenced by cultural behaviors associated with pain • Adolescent: can verbalize but may choose to be “tough” in front of peers; regression
Developmental Aspects of Pain Expression • Infant: intense cry, unable to sleep or eat • Toddler: verbal or physical aggression or withdrawal, guarding the site or pain • Preschooler: can verbalize but much “magical thinking”, see pain as punishment • School-age: can verbalize but very influenced by cultural behaviors associated with pain • Adolescent: can verbalize but may choose to be “tough” in front of peers; regression
 Why treat pain? • Health care providers value providing comfort “as the right thing to do” • Barriers: • Lack of education about pain medication – Need handy resources for » Dosing » Treatment of side effects • Lack of understanding that a person may not “look like” he is in pain • Misunderstanding of risks of use of opioids Fear of addiction Fear of respiratory depression
Why treat pain? • Health care providers value providing comfort “as the right thing to do” • Barriers: • Lack of education about pain medication – Need handy resources for » Dosing » Treatment of side effects • Lack of understanding that a person may not “look like” he is in pain • Misunderstanding of risks of use of opioids Fear of addiction Fear of respiratory depression
 Today…. . the Reality is Our Patients’ Pain is often…. • Untreated • Under-treated • Inappropriately Treated
Today…. . the Reality is Our Patients’ Pain is often…. • Untreated • Under-treated • Inappropriately Treated
 Assessment of Pain Needs to be comprehensive, more than a Pain Intensity Scale – Intensity: asking from 0 -10 to rate amount of pain – Location of the pain – Type of pain: describe the pain in terms of adjectives such as “burning”, “cramping” – Duration: when did it start? Patterns? – What makes pain better? Worse? – Previous/current medications – How is the pain interfering with • Normal activities (play, school, being with friends, eating, sleep) • Not adequate to just assess current pain levels…. . need to ask about what happens which children are active
Assessment of Pain Needs to be comprehensive, more than a Pain Intensity Scale – Intensity: asking from 0 -10 to rate amount of pain – Location of the pain – Type of pain: describe the pain in terms of adjectives such as “burning”, “cramping” – Duration: when did it start? Patterns? – What makes pain better? Worse? – Previous/current medications – How is the pain interfering with • Normal activities (play, school, being with friends, eating, sleep) • Not adequate to just assess current pain levels…. . need to ask about what happens which children are active
 Self-Report of Pain • The single most reliable indicator, using a valid and reliable scale when possible • Select an age-appropriate scale • Ask in trusting environment – Assumption is that the number the child reports will be believed by the health care provider
Self-Report of Pain • The single most reliable indicator, using a valid and reliable scale when possible • Select an age-appropriate scale • Ask in trusting environment – Assumption is that the number the child reports will be believed by the health care provider
 • Ask the patient (usually > age 12 years to") Numerical Pain Scale (NRS) • Ask the patient (usually > age 12 years to rate their pain from 0 to 10 • Requires the understanding that increasing ordinal numbers mean pain at a higher intensity
Numerical Pain Scale (NRS) • Ask the patient (usually > age 12 years to rate their pain from 0 to 10 • Requires the understanding that increasing ordinal numbers mean pain at a higher intensity
 Faces Pain Scale Useful for children age 5 -12 years Some children 3 -5 years of age can use it Need to ask in terms of the “worst pain you can thin Wong, 2001
Faces Pain Scale Useful for children age 5 -12 years Some children 3 -5 years of age can use it Need to ask in terms of the “worst pain you can thin Wong, 2001
 How can pain intensity be assessed in children who cannot self-report? • Random observation of factors may not indicate pain • Needed are research-based indicators of pain based on developmental stage • Observational pain scales can facilitate the quantification and evaluation of pain behaviors for clinical decision making – Do such scales only tell us whether pain is present or not?
How can pain intensity be assessed in children who cannot self-report? • Random observation of factors may not indicate pain • Needed are research-based indicators of pain based on developmental stage • Observational pain scales can facilitate the quantification and evaluation of pain behaviors for clinical decision making – Do such scales only tell us whether pain is present or not?
 Pain Behaviors • • Noisy breathing Negative vocalizations Lack of facial expression Sad facial expression Frightened facial expression Lack of relaxed body relaxation Tense body language Fidgeting
Pain Behaviors • • Noisy breathing Negative vocalizations Lack of facial expression Sad facial expression Frightened facial expression Lack of relaxed body relaxation Tense body language Fidgeting
 Pain Assessment • Under age 5 years or the patient cannot self report: need a behavioral scale • How a person expresses pain (pain behaviors) FLACC (Merkel, 1997)
Pain Assessment • Under age 5 years or the patient cannot self report: need a behavioral scale • How a person expresses pain (pain behaviors) FLACC (Merkel, 1997)
 Warning about Behavioral Pain Assessment Methods • No way we can accurately know how persons are feeling if they can not speak or report their pain level themselves • Clinicians then must use – Research-based behaviorally-based pain scales • But also must include – Critical thinking (“Does what I see make sense for this patient? ”) – Input of family members – Rational decision making (“trial of analgesic to see if behaviors of child improve”
Warning about Behavioral Pain Assessment Methods • No way we can accurately know how persons are feeling if they can not speak or report their pain level themselves • Clinicians then must use – Research-based behaviorally-based pain scales • But also must include – Critical thinking (“Does what I see make sense for this patient? ”) – Input of family members – Rational decision making (“trial of analgesic to see if behaviors of child improve”
 • What if the child cannot self-report or display pain") Assume Pain Present (APP) • What if the child cannot self-report or display pain behaviors, yet has reason to be feeling pain? Too ill or paralyzed • Implication: have patient on pain medications – Opioid infusion • Titrate with clinical signs of pain and vital signs • Use for any age when only pathology or potentially painful procedure and patient cannot self-report or move to indicate pain Credit to Margo Mc. Caffery
Assume Pain Present (APP) • What if the child cannot self-report or display pain behaviors, yet has reason to be feeling pain? Too ill or paralyzed • Implication: have patient on pain medications – Opioid infusion • Titrate with clinical signs of pain and vital signs • Use for any age when only pathology or potentially painful procedure and patient cannot self-report or move to indicate pain Credit to Margo Mc. Caffery
 Challenges in Assessment: The Gap • Development of tools for preterm and term neonates with ongoing or chronic pain • Exposure to prolonged or severe pain may increase neonatal morbidity; long term effects of neonatal pain – Longitudinal studies involving infants < 1000 grams at 10 years of age AAP, 2000
Challenges in Assessment: The Gap • Development of tools for preterm and term neonates with ongoing or chronic pain • Exposure to prolonged or severe pain may increase neonatal morbidity; long term effects of neonatal pain – Longitudinal studies involving infants < 1000 grams at 10 years of age AAP, 2000
 What is Pain Assessment? • It is NOT just a pain score. • A Pain Intensity Score is just a screening – Tells you whether the patient is having pain or not – Tells you whether further evaluation needs to be done if the patient is in pain • Assumption is that you will ask the patient if he is pain and, if so, believe the patient • Severe pain: scales may oversimplify the amount of pain the person is feeling
What is Pain Assessment? • It is NOT just a pain score. • A Pain Intensity Score is just a screening – Tells you whether the patient is having pain or not – Tells you whether further evaluation needs to be done if the patient is in pain • Assumption is that you will ask the patient if he is pain and, if so, believe the patient • Severe pain: scales may oversimplify the amount of pain the person is feeling
 Assessment of Pain Needs to be comprehensive – Location of the pain – Type of pain: describe the pain in terms of adjectives such as “burning”, “cramping” – Duration: when did it start? Patterns? – What makes pain better? Worse? – Previous/current medications – How is the pain interfering with • Normal activities (play, school, being with friends, eating, sleep) • Not adequate to just assess current pain levels…. . need to ask about what happens which children are active
Assessment of Pain Needs to be comprehensive – Location of the pain – Type of pain: describe the pain in terms of adjectives such as “burning”, “cramping” – Duration: when did it start? Patterns? – What makes pain better? Worse? – Previous/current medications – How is the pain interfering with • Normal activities (play, school, being with friends, eating, sleep) • Not adequate to just assess current pain levels…. . need to ask about what happens which children are active
 When to offer an intervention? • Assumed that acute pain, threshold for treatment is at least “moderate” level – None, mild, moderate, severe • “What is moderate? ” – Is it > 3/10? • What is severe? – Is it 5, 6, or 7/10? • Should it be individualized such as a “pain goal”? What is an “acceptable pain level? ” Cheng et al, 2003
When to offer an intervention? • Assumed that acute pain, threshold for treatment is at least “moderate” level – None, mild, moderate, severe • “What is moderate? ” – Is it > 3/10? • What is severe? – Is it 5, 6, or 7/10? • Should it be individualized such as a “pain goal”? What is an “acceptable pain level? ” Cheng et al, 2003
 What is a Meaningful Response to an Intervention? • What is tolerable? Is it 3/10? • What is pain relief? < 5/10, 50% reduction with an intervention? How to balance with the side effects of interventions? Cost of interventions? • What makes an analgesic effective?
What is a Meaningful Response to an Intervention? • What is tolerable? Is it 3/10? • What is pain relief? < 5/10, 50% reduction with an intervention? How to balance with the side effects of interventions? Cost of interventions? • What makes an analgesic effective?
 Approach to Acute & Chronic Pain Complex Problem Physiological Factors Psychological Factors Social Factors • • • MDs RNs Psychologists Pharmacists Physical therapists Social workers Chaplains Art/music therapists Child Life Specialists
Approach to Acute & Chronic Pain Complex Problem Physiological Factors Psychological Factors Social Factors • • • MDs RNs Psychologists Pharmacists Physical therapists Social workers Chaplains Art/music therapists Child Life Specialists
 Goals of Pain Management • Provide maximum pain relief with minimal side effects and maximal function • How? – Identify the cause(s) of the pain – Prevent pain (preemptive strategies) – Treat the pain: NOT JUST BY DRUGS • Provide the simplest method of analgesic delivery • If drugs, minimize the side effects
Goals of Pain Management • Provide maximum pain relief with minimal side effects and maximal function • How? – Identify the cause(s) of the pain – Prevent pain (preemptive strategies) – Treat the pain: NOT JUST BY DRUGS • Provide the simplest method of analgesic delivery • If drugs, minimize the side effects
 Savvy Pain Management • How do we ask for what the patient needs? • Know the pharmacological options including a guideline for dosages – Regimen needs to be • Least invasive • Within capability of the child/family • Consider costs of plan • Know the nonpharmacological options to “make the pain medications work better” • Have the data available to communicate to the prescribing clinician
Savvy Pain Management • How do we ask for what the patient needs? • Know the pharmacological options including a guideline for dosages – Regimen needs to be • Least invasive • Within capability of the child/family • Consider costs of plan • Know the nonpharmacological options to “make the pain medications work better” • Have the data available to communicate to the prescribing clinician
 Make immediately accessible to bedside caregivers • Pocket cards • Wall charts Need to know how to calculate the dose which is usually referenced in mg or mcg/kg Not guesswork!!!!!!!!!!!!
Make immediately accessible to bedside caregivers • Pocket cards • Wall charts Need to know how to calculate the dose which is usually referenced in mg or mcg/kg Not guesswork!!!!!!!!!!!!
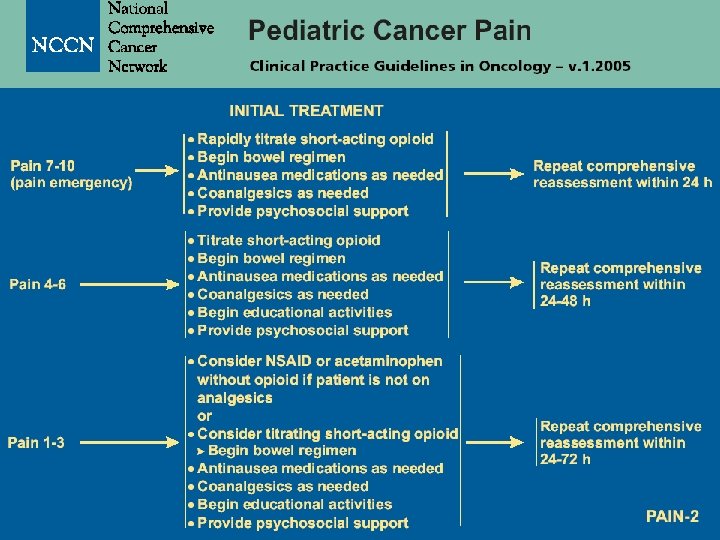
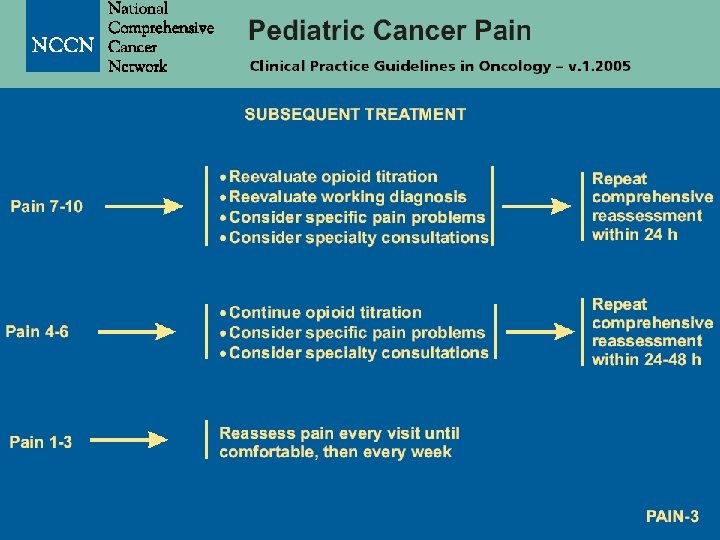
 Free at www. nccn. org
Free at www. nccn. org
 www. nccn. org
www. nccn. org
 Position Statements • ASPMN – Neonatal Circumcision Pain Relief – Pain Management at the End of Life – Use of Placeboes in Pain Management – Authorized Agent use of Analgesic Pumps – Pain Assessment in the Nonverbal Patient
Position Statements • ASPMN – Neonatal Circumcision Pain Relief – Pain Management at the End of Life – Use of Placeboes in Pain Management – Authorized Agent use of Analgesic Pumps – Pain Assessment in the Nonverbal Patient
 • Ibuprofen (Motrin®) • Naproxen (Naprosyn®) • IV Toradol (Ketoralac®)") Non-steroidal Anti-inflammatory Drugs (NSAIDS) • Ibuprofen (Motrin®) • Naproxen (Naprosyn®) • IV Toradol (Ketoralac®) • Advantages: • Effective anti-inflammatory and treatment for bone pain • Avoid side effects of opioids • Disadvantages: • Inhibit platelet function • Renal and gastrointestinal toxicity
Non-steroidal Anti-inflammatory Drugs (NSAIDS) • Ibuprofen (Motrin®) • Naproxen (Naprosyn®) • IV Toradol (Ketoralac®) • Advantages: • Effective anti-inflammatory and treatment for bone pain • Avoid side effects of opioids • Disadvantages: • Inhibit platelet function • Renal and gastrointestinal toxicity
 Acetaminophen • Advantages: • • Does not interfere with • platelet function • • No gastrointestinal • toxicity • No renal toxicity • Readily available • Inexpensive Disadvantages: Weak anti-inflammatory Liver toxicity Dose: 15 mg/kg PO q 4 h with max of 4000 mg/day
Acetaminophen • Advantages: • • Does not interfere with • platelet function • • No gastrointestinal • toxicity • No renal toxicity • Readily available • Inexpensive Disadvantages: Weak anti-inflammatory Liver toxicity Dose: 15 mg/kg PO q 4 h with max of 4000 mg/day
:") Opioids: Mainstay of Treatment • • • Morphine: PO, IV Oxycodone: PO Hydromorphone (Dilaudid®): PO and IV Fentanyl: IV and transdermal Codeine: PO • Do not give meperidine (Demerol®) in repeated doses: has metabolite that is neurotoxic
Opioids: Mainstay of Treatment • • • Morphine: PO, IV Oxycodone: PO Hydromorphone (Dilaudid®): PO and IV Fentanyl: IV and transdermal Codeine: PO • Do not give meperidine (Demerol®) in repeated doses: has metabolite that is neurotoxic
 Opioid Doses for Infants • Because of immature responses to hypoxia and hypercarbia and • Longer elimination half-life and slower clearance rates • Doses for infants < 6 months of age of opioids should be reduced by 20 -50% on a per kilogram basis relative to dosing older children
Opioid Doses for Infants • Because of immature responses to hypoxia and hypercarbia and • Longer elimination half-life and slower clearance rates • Doses for infants < 6 months of age of opioids should be reduced by 20 -50% on a per kilogram basis relative to dosing older children
 n. Methods of Opioid Administration • Oral: preferred – Long-acting for continuous pain – Short-acting/immediate release for intermittent pain or breakthrough pain while on continuous • Intramuscular: not recommended • Intravenous: – Intermittent scheduled or continuous infusion (basal) for continuous pain – PRN doses only for intermittent pain – Patient controlled analgesia (PCA)
n. Methods of Opioid Administration • Oral: preferred – Long-acting for continuous pain – Short-acting/immediate release for intermittent pain or breakthrough pain while on continuous • Intramuscular: not recommended • Intravenous: – Intermittent scheduled or continuous infusion (basal) for continuous pain – PRN doses only for intermittent pain – Patient controlled analgesia (PCA)
 Long-acting Opioids Opioid/route SR Preparation Dose frequency Morphine/PO Oramorph® Every 12 hrs Kadian® Every 12 or 24 hrs MS Contin® Every 12 hrs Oxycodone/PO Oxycontin® Every 12 hrs Fentanyl/transd Duragesic® ermal patches Every 72 hrs
Long-acting Opioids Opioid/route SR Preparation Dose frequency Morphine/PO Oramorph® Every 12 hrs Kadian® Every 12 or 24 hrs MS Contin® Every 12 hrs Oxycodone/PO Oxycontin® Every 12 hrs Fentanyl/transd Duragesic® ermal patches Every 72 hrs
 IV Oral 10 30 Hydromorphone 1.") Equianalgesic Doses Drug Morphine Equianalgesic Dose (in mg) IV Oral 10 30 Hydromorphone 1. 5 7. 5 0. 1 -0. 2 Not available 15 -30 Fentanyl Oxycodone
Equianalgesic Doses Drug Morphine Equianalgesic Dose (in mg) IV Oral 10 30 Hydromorphone 1. 5 7. 5 0. 1 -0. 2 Not available 15 -30 Fentanyl Oxycodone
 Use of Opioids • Dosages in guidelines are given as starting doses (for opioid naïve) – in mg (or mcg)/kg • All other dosing is “Titration, titration” • No maximum dose for any opioid • Always want to benefit the patient (effective analgesia) with the least amount of risk (minimize opioid side effects)
Use of Opioids • Dosages in guidelines are given as starting doses (for opioid naïve) – in mg (or mcg)/kg • All other dosing is “Titration, titration” • No maximum dose for any opioid • Always want to benefit the patient (effective analgesia) with the least amount of risk (minimize opioid side effects)
 Opioid Doses To Relieve Suffering: Boston Children’s • Retrospective review of 12 patients who required high dosages of opioids during terminal care – found that ranges from 3. 8 to 518 mg/kg/hr of morphine (or equivalent) were needed • Conclusions: standard dosing of opioids adequately treats most cancer pain in children; however, a significant group requires more extensive management. – Seen more often in solid tumors metastatic to spine and major nerves » Collins, J Pediatri, 1995
Opioid Doses To Relieve Suffering: Boston Children’s • Retrospective review of 12 patients who required high dosages of opioids during terminal care – found that ranges from 3. 8 to 518 mg/kg/hr of morphine (or equivalent) were needed • Conclusions: standard dosing of opioids adequately treats most cancer pain in children; however, a significant group requires more extensive management. – Seen more often in solid tumors metastatic to spine and major nerves » Collins, J Pediatri, 1995
 Addiction • A pattern of compulsive drug use characterized by a continued craving for a drug and the need to use it for effects other than relief of symptoms such as pain
Addiction • A pattern of compulsive drug use characterized by a continued craving for a drug and the need to use it for effects other than relief of symptoms such as pain
 Physiological Dependence • The patient has developed a physical need for the drug such that rapid withdrawal will manifest as a specific set of symptoms – yawning, tearing and rhinorrhea – sweating, restlessness and irritability – tremors, dilated pupils • May progress to: – nausea, vomiting and, diarrhea – chills, muscle spasm and increased irritability
Physiological Dependence • The patient has developed a physical need for the drug such that rapid withdrawal will manifest as a specific set of symptoms – yawning, tearing and rhinorrhea – sweating, restlessness and irritability – tremors, dilated pupils • May progress to: – nausea, vomiting and, diarrhea – chills, muscle spasm and increased irritability
 Side Effects of Opioids • Constipation – Senna or bisacodyl – Docusate (only stool softener) – Magnesium citrate – Lactulose – Miralax® (polyethalene glycol) • Pruritus: use an alternative opioids – Diphenhydramine (Benedryl): 0. 5 -1 mg/kg
Side Effects of Opioids • Constipation – Senna or bisacodyl – Docusate (only stool softener) – Magnesium citrate – Lactulose – Miralax® (polyethalene glycol) • Pruritus: use an alternative opioids – Diphenhydramine (Benedryl): 0. 5 -1 mg/kg
 Weaning of opioids • Calculate the total amount of opioid received 24 hours • Reduce this amount by 20% the first day • Wean subsequent doses by 10% per day as tolerated
Weaning of opioids • Calculate the total amount of opioid received 24 hours • Reduce this amount by 20% the first day • Wean subsequent doses by 10% per day as tolerated
 – 5 mg/kg or 100 mg TID") Neuropathic Pain Medications • Anti-convulsants: Gabapentin (Neurontin®) – 5 mg/kg or 100 mg TID up to 70 mg/kg/day or 1200 mg TID • Tri-cyclic Anti-depressants (TCAs) : Amitriptyline (Elavil®) – 0. 1 mg/kg PO or 25 mg at bedtime increased to 1 mg/kg bedtime • Need to teach patients – To give as directed (not PRN and not to skip doses) – Treatment may not be effective for several days – May need to increase dose before effective • Opioids may help especially the first few days of treatment
Neuropathic Pain Medications • Anti-convulsants: Gabapentin (Neurontin®) – 5 mg/kg or 100 mg TID up to 70 mg/kg/day or 1200 mg TID • Tri-cyclic Anti-depressants (TCAs) : Amitriptyline (Elavil®) – 0. 1 mg/kg PO or 25 mg at bedtime increased to 1 mg/kg bedtime • Need to teach patients – To give as directed (not PRN and not to skip doses) – Treatment may not be effective for several days – May need to increase dose before effective • Opioids may help especially the first few days of treatment
 What about Chronic Pain? • • Really is persistent pain “a sensory, emotion, and cognitive experience…” Cannot always promise “No Pain” Need to achieve the level of pain that is needed to be able to conduct activities with the least amount of side effects from the analgesics or other interventions • Defined as a “pain goal” Slatkin, City of Hope
What about Chronic Pain? • • Really is persistent pain “a sensory, emotion, and cognitive experience…” Cannot always promise “No Pain” Need to achieve the level of pain that is needed to be able to conduct activities with the least amount of side effects from the analgesics or other interventions • Defined as a “pain goal” Slatkin, City of Hope
 Pain Goal • Pain Goal: what number do you need to have as a maximum before the pain interferes with: – Sleep – Normal activities for developmental age and limitations of illness • • Going to school Playing Sleeping Eating
Pain Goal • Pain Goal: what number do you need to have as a maximum before the pain interferes with: – Sleep – Normal activities for developmental age and limitations of illness • • Going to school Playing Sleeping Eating
 What if the patient needs more that what is ordered? • Know the pain score and other assessment data • Know the current analgesic dosages • Know the overall medical condition of the patient including rehabilitation and discharge plan • Morphine 10 mg PO q 3 hours PRN • Took dose at 0830, asking for dose at 1030 • Yesterday used 6 doses • Could a sustained-release preparation be used?
What if the patient needs more that what is ordered? • Know the pain score and other assessment data • Know the current analgesic dosages • Know the overall medical condition of the patient including rehabilitation and discharge plan • Morphine 10 mg PO q 3 hours PRN • Took dose at 0830, asking for dose at 1030 • Yesterday used 6 doses • Could a sustained-release preparation be used?
 Advocacy = Planning • Patient is using IV morphine 3 mg every 3 hours • Discussion of the patient going home tomorrow needing months of rehabilitation for extensive surgery • Need to know 6 doses of morphine IV (18 mg) = 54 mg PO • Should Oramorph 15 mg PO BID be started the day before? • Teach the family to know how to dose for breakthrough pain (morphine 10 mg PO q 2 hours PRN)
Advocacy = Planning • Patient is using IV morphine 3 mg every 3 hours • Discussion of the patient going home tomorrow needing months of rehabilitation for extensive surgery • Need to know 6 doses of morphine IV (18 mg) = 54 mg PO • Should Oramorph 15 mg PO BID be started the day before? • Teach the family to know how to dose for breakthrough pain (morphine 10 mg PO q 2 hours PRN)
 patient who had extensive orthopedic surgery") Case Study • 6 year old (15 kg) patient who had extensive orthopedic surgery • Day of surgery: needs morphine IV available on scheduled basis – Recommendation is 0. 1 mg/kg every 2 -4 hours • Day following surgery – Pain scores < 3/10 with 10 doses of 1. 5 mg morphine IV – Consider morphine infusion of 1 mg/hr with careful reassessment
Case Study • 6 year old (15 kg) patient who had extensive orthopedic surgery • Day of surgery: needs morphine IV available on scheduled basis – Recommendation is 0. 1 mg/kg every 2 -4 hours • Day following surgery – Pain scores < 3/10 with 10 doses of 1. 5 mg morphine IV – Consider morphine infusion of 1 mg/hr with careful reassessment
 Case Study • Also complains of “burning pain” in leg • Consider gabapentin 100 mg every 8 hours • To plan for discharge: convert to oral morphine tablets using 1 mg of IV morphine = 3 mg oral morphine • Patient’s infusion = 24 mg plus the patient had additional doses of 1. 5 mg for dressing change and physical therapy (total of 6 mg) – Total of 30 mg IV = 90 mg oral
Case Study • Also complains of “burning pain” in leg • Consider gabapentin 100 mg every 8 hours • To plan for discharge: convert to oral morphine tablets using 1 mg of IV morphine = 3 mg oral morphine • Patient’s infusion = 24 mg plus the patient had additional doses of 1. 5 mg for dressing change and physical therapy (total of 6 mg) – Total of 30 mg IV = 90 mg oral
 Case Study • Then gradually reduce the opioid but still control the pain “around-the-clock” • Use long-acting morphine: – 30 mg every 12 hours – With immediate-release doses of 5 -10 mg every 2 hours as needed – Continue gabapentin and increase to 200 mg every 8 hours if neuropathic pain is still present • Return to outpatient clinic – Evaluate doses of immediate-release morphine
Case Study • Then gradually reduce the opioid but still control the pain “around-the-clock” • Use long-acting morphine: – 30 mg every 12 hours – With immediate-release doses of 5 -10 mg every 2 hours as needed – Continue gabapentin and increase to 200 mg every 8 hours if neuropathic pain is still present • Return to outpatient clinic – Evaluate doses of immediate-release morphine
 Case Study • As patient takes less immediate-release morphine, reduce the long-acting to 15 mg every 12 hours and then discontinue • Patient may need immediate-release and gabapentin for weeks, especially for physical therapy • Require parent to write down doses on “pain diary” to monitor use of all analgesics
Case Study • As patient takes less immediate-release morphine, reduce the long-acting to 15 mg every 12 hours and then discontinue • Patient may need immediate-release and gabapentin for weeks, especially for physical therapy • Require parent to write down doses on “pain diary” to monitor use of all analgesics
 Children are the living messages we send to a time we will not see. John W Whitehead, The Stealing of America, 1983
Children are the living messages we send to a time we will not see. John W Whitehead, The Stealing of America, 1983
 References 1 • Anghelescu D & Oakes L: Working toward better cancer pain management for children, Canc Prac 10(supp ): S 52 -S 57, 2002 • Anghelescu, D, Oakes, L, Popenhagen, M: Management of pain due to cancer in neonates, children, and adolescents. In: de Leon-Casasola OA, ed. Cancer Pain: Pharmacologic, Interventional, and Palliative Care Approaches, Philadelphia, Elsevier Science, 2006 • Collins JJ et al: Control of severe pain in children with terminal malignancy, J Pediatr 126: 4, 653, 1995 • Collins JJ et al: Management of pain in childhood cancer. In Schecter NL et al: Pain in Infants, Children, and Adolescents, 2 nd ed, 2003, 517 -538
References 1 • Anghelescu D & Oakes L: Working toward better cancer pain management for children, Canc Prac 10(supp ): S 52 -S 57, 2002 • Anghelescu, D, Oakes, L, Popenhagen, M: Management of pain due to cancer in neonates, children, and adolescents. In: de Leon-Casasola OA, ed. Cancer Pain: Pharmacologic, Interventional, and Palliative Care Approaches, Philadelphia, Elsevier Science, 2006 • Collins JJ et al: Control of severe pain in children with terminal malignancy, J Pediatr 126: 4, 653, 1995 • Collins JJ et al: Management of pain in childhood cancer. In Schecter NL et al: Pain in Infants, Children, and Adolescents, 2 nd ed, 2003, 517 -538
 References 2 • International Association for the Study of Pain, Subcommittee on Taxonomy: Pain terms: a list with definitions and notes on usage, Pain 6: 249252, 1979 • Mc. Caffery M et al: Pain management: problems and progress. In Mc. Caffery M & Pasero C, eds: Pain: Clinical Manual, 2 nd ed, Mosby, 1999 • Merkel et al: The FLACC: a behavioral scale for scoring postoperative pain in young children, Pediatr Nurs 23: 293 -297, 1997
References 2 • International Association for the Study of Pain, Subcommittee on Taxonomy: Pain terms: a list with definitions and notes on usage, Pain 6: 249252, 1979 • Mc. Caffery M et al: Pain management: problems and progress. In Mc. Caffery M & Pasero C, eds: Pain: Clinical Manual, 2 nd ed, Mosby, 1999 • Merkel et al: The FLACC: a behavioral scale for scoring postoperative pain in young children, Pediatr Nurs 23: 293 -297, 1997
 References 3 • Wolfe J et al: Symptoms and suffering at the end of life in children with cancer. N Engl J Med 342: 326 -333, 2000 • Wong DL et al. Essentials of Pediatric Nursing, 6 th ed, 2001 • World Health Organization: Cancer Pain Relief and Palliative Care in Children, 1998 (to order internationally, email to bookorders@who. ch)
References 3 • Wolfe J et al: Symptoms and suffering at the end of life in children with cancer. N Engl J Med 342: 326 -333, 2000 • Wong DL et al. Essentials of Pediatric Nursing, 6 th ed, 2001 • World Health Organization: Cancer Pain Relief and Palliative Care in Children, 1998 (to order internationally, email to bookorders@who. ch)