5d14b87c0479f95167ff0714f408c2e8.ppt
- Количество слайдов: 67



Pediatric Neurologic Emergencies Leybie Ang July 31 2008

Objectives l Febrile Seizures l Status Epilepticus l Encephalitis

FEBRILE SEIZURE

Case Presentation l 16 month old, former 38 weeker l Previously healthy l Brought in by EMS l Seizure activity at home l Lasting 1 -2 minutes l Arms and legs twitching l 3 days hx of URI symptoms

Febrile Seizure – Definition l NIH definition ¡ An event in infancy or childhood usually occurring between 3 month and 5 year of age, associated with fever but without evidence of intracranial infection or defined cause of seizure

Febrile Seizure - Incidence l 2 -5% ¡ Up in children < 5 yo to 15% l Majority between 12 -18 mo l One parent – 4. 4 x l Both parents – 20 x l Sibling – 3. 6 x l Second degree relative – 2. 7 x

Simple Febrile Seizure l Most common l Seizure < 15 minutes l No focal features l Only once in 24 hr time period

Complex Febrile Seizure l Episodes lasting > 15 minutes l Focal features or postical paresis l > 1 episode in 24 hrs l Seizure in a series with total duration > 30 minutes
 l")
Risk Factors For Recurrence l Low fever at time of first sz (<40) l Young age (<12 month old) l Family hx of febrile sz l Short period of time between fever and sz (<24 hr) l ? male

Risk Factors For Developing Epilepsy l Family Hx of epilepsy l Complex features l Presence of early onset neurodevelopmental abnormalies

Febrile Seizure - Immunization l Risk of febrile seizure increases l By 1. 5 fold on day of DTP immunization ¡ Risk now reduced if DTa. P ¡ Acellular pertussis instead of whole cell pertussis l By 3. 0 fold with the peak occurring 1 -2 weeks after MMR vaccination

Differential Diagnosis l Shaking/Chills l Trauma l Toxins l Metabolic disorder l Meningitis/Encephalitis


Febrile Seizure - Management l. A l. B l. C

Febrile Seizure - Management l Antipyretics l Sponging l Antiepileptic

Febrile Seizures – Antipyretics l Uhari et al J peds 1995 126: 991 180 kids RDBPC (plac + plac, plac + acet, diaz + plac) no difference in recurrence x 2 yrs l Schnaiderman et al Eur J Peds 1993 152: 747 104 kids RCT acet q 4 h scheduled or prn, no difference l Van Stuijvenberg et al Peds 1998 102: 1 230 kids RDBPC ibuprofen to plac no diff X 1 yr

Febrile Seizure - Antipyretics l Meremikwa et al Cochrane Database 2002 ¡ Systematic review of 12 trials acetaminophen vs placebo +/-sponging l Insufficient evidence

Febrile Seizure - Diazepam l Dose ¡ ¡ ¡ given when: when child is febrile before start seizing or as soon as start seizing l Oral dosage given at time of fever – 44% reduction in the risk of febrile seizure person-year with diazepam

Febrile Seizure - Phenobarbital l Effective in preventing recurrence of simple febrile seizure l Daily therapy reduced the rate of subsequent febrile seizure from 25% to 5% l Adverse effect : ¡ hyperactivity, hypersensitivity reaction (SJS), loss of cognitive function

Febrile Seizure – Valproic Acid l As effective as phenobarbital in preventing recurrent simple febrile seizure l More l Side effective than placebo effect : ¡ Fatal hepatotoxicity (esp <3 yo at greatest risk)

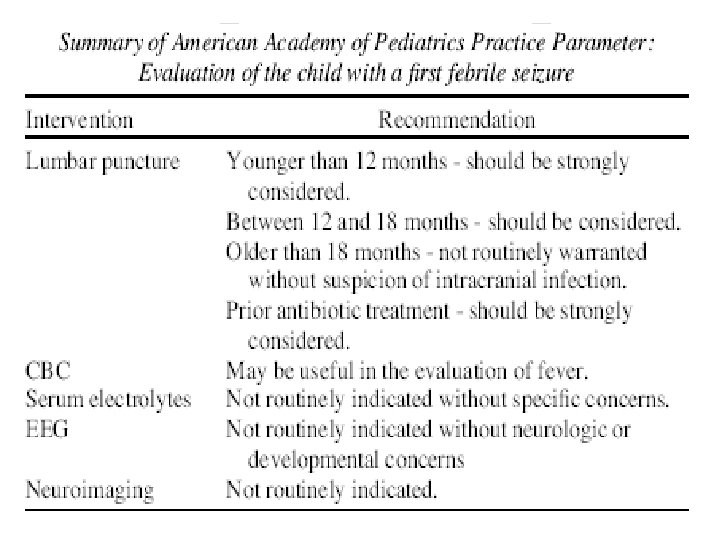
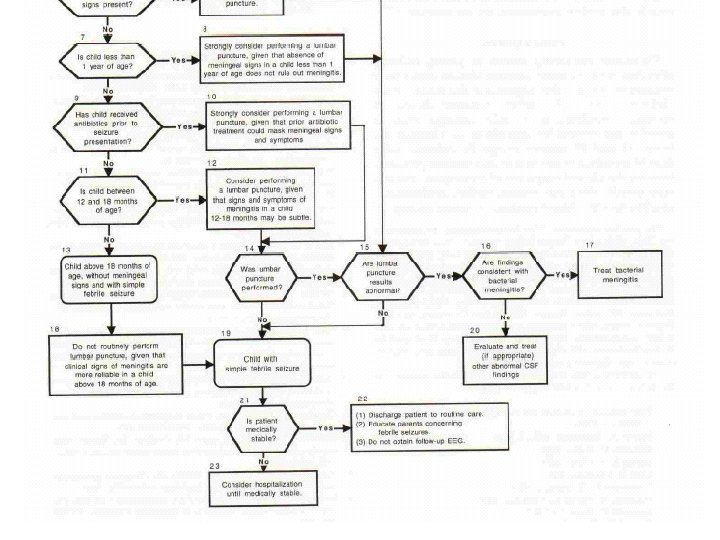
Febrile Seizure - Prevention Committee on Quality Improvement Subcommittee on Febrile Seizure of the AAP 1999 l “Based on the risk and benefits of effective therapies, neither continuous nor intermittent anticonvulsant therapy is recommended for children with one or more simple febrile seizures. AAP recognises that recurrent episodes of febrile seizures can create anxiety in some parents and their children and as such appropriate educational and emotional support should be provided”

Question #1 l In the emergency department, you are talking with the parents of a 17 month old boy who was evaluated for a first generalised seizure that lasted 7 minutes and followed by a fever 102. 9 F (39. 4 C). Other than OM, findings on the physical examination were normal, and the child was discharged home. The child is developmentally normal. Upon examination, the child now appears well.

l l l Of the following, your MOST likely statement to the parents is that A. antipyretic agents are effective in preventing future febrile seizures B. CT head is preferred to MRI brain for evaluation of this child C. EEG is not indicated D. The chance of another febrile sz is ~50% E. The child has a 5% chance of developing epilepsy

STATUS EPILEPTICUS

Status Epilepticus - Introduction l EFA ¡ Two or more sequential seizures without full recovery of consciousness between seizures, or more than 30 minutes of continuous seizure activity l 10 -58 per 100, 000 per year for children 1 to 19 year old l More common in in children with epilepsy 9 -27%

Status Epilepticus - Etiology l 26% acute ¡ Bleed ¡ Trauma ¡ Infection CNS insult l 20% underlying seizure disorder ¡ Sudden discontinuation of meds ¡ Drug interaction ¡ Fever l 53% unknown

Status Epilepticus

Status Epilepticus – Blood Culture l Should blood culture be routinely done in children in SE? l Six Class III studies, total 357 children, BC positive in 2. 5% l Insufficient data to support or refute in children whether blood cultures should be done routine basis in children whom there is no clinical suspicious for infection

Status Epilepticus – Lumbar Puncture l Should LP be routinely done in children with SE? l Class III studies – out of 1, 859 children 12. 8% has documented CNS infection l Insufficient data to support or refute in children whether lumbar puncture should be done routine basis in children whom there is no clinical suspicious for infection

Status Epilepticus – AED Levels l Should AED levels be routinely obtained in children taking AED who develop SE? l Class II data showed that low AED levels in 32% of children on AEDs l AED levels should be considered when a child with epilepsy on AED prophylaxis develops SE

Status Epilepticus – Toxicology Testing l Should toxicology testing be routinely ordered in children with SE? l Class III studies showed that a diagnosis of ingestion in 3. 6% l Toxicology testing maybe considered in children with SE, when no apparent etiology is immediately identified. l Specific serum toxicology level is required

Status Epilepticus - EEG l Should an EEG be routinely performed in the evaluation of a child with SE? l Class III studies reported that abnormal brain activity on 43. 1% of EEG done on SE l EEG may be considered in a child with new onset SE

Status Epilepticus – Imaging l Neuroimaging may be considered for the evaluation of the child with SE if there are clinical indications or if the etiology is appropriately stabilised and the seizure activity controlled

Imaging - CT vs. MRI l MRI useful for: ¡ More detailed view of brain anatomy ¡ Better screen for CNS malformations and dysplastic lesions, temporal lobe (esp. hippocampus) l CT useful for: ¡ Larger neoplasms, old infarctions, major malformative processes ¡ Assessment of the critically ill child

Status Epilepticus - Managemnet l. A l. B l. C

SE treatment l 1 st line anticonvulsants ¡ IV l l l ¡ Rectal diazepam l l l ¡ Lorazepam 0. 1 mg/kg Diazepam 0. 2 mg/kg Midazolam 0. 2 mg/kg 2 -5 yrs – 0. 5 mg/kg 6 -11 yrs – 0. 3 mg/kg >12 yrs – 0. 2 mg/kg IM, intranasal, buccal midazolam

SE treatment l 2 nd line agents ¡ ¡ l Phenytoin 20 mg/kg @ 1 mg/kg/min (upto 50 mg/min) Fosphenytoin 15 -20 PE/kg @ 3 mg/kg/min (upto 150 mg/min) 3 rd line agents ¡ ¡ ¡ Phenobarbital 20 mg/kg @ 100 mg/min Repeat prn 5 -10 mg/kg Maximum 40 mg/kg or 1 gram

Refractory SE treatment l Consider midazolam ¡ ¡ l Induce barbiturate coma ¡ ¡ l 0. 2 mg/kg bolus 1 -10 mcg/kg/min infusion Pentobarbital 5 -15 mg/kg @ 25 mg/min Then 1 -5 mg/kg/hour Others ¡ ¡ Valproic acid Paraldehyde, chloral hydrate Propofol, inhalational anesthesia, paralysis lidocaine

Status Epilepticus - Complications l Hypoxia ¡ Impaired ventilation ¡ Increased secretions ¡ Increased O 2 consumption ¡ Impaired O 2 delivery ¡ Metabolic and respiratory acidosis l Brain injury ¡ Hypoxia and hypoperfusion ¡ MR, behaviour changes, neuro deficits

Status Epilepticus - Complications l Morbidity l< 1 yo - 30% l > 3 yo – 6% l Mortality ¡ 3%

Question #2 l. A 8 month old girl is brought into the emergency department in status epilepticus. She has had diarrhea for the past 4 days. The infant had received bottled water for the past 3 days of her illness and cola for the past 24 hr.

l Of the following, the MOST likely cause of her status epilepticus is l A. Hypocalcemia l B. Hypoglycemia l C. Hypokalemia l D. Hypomagnesemia l E. Hyponatremia

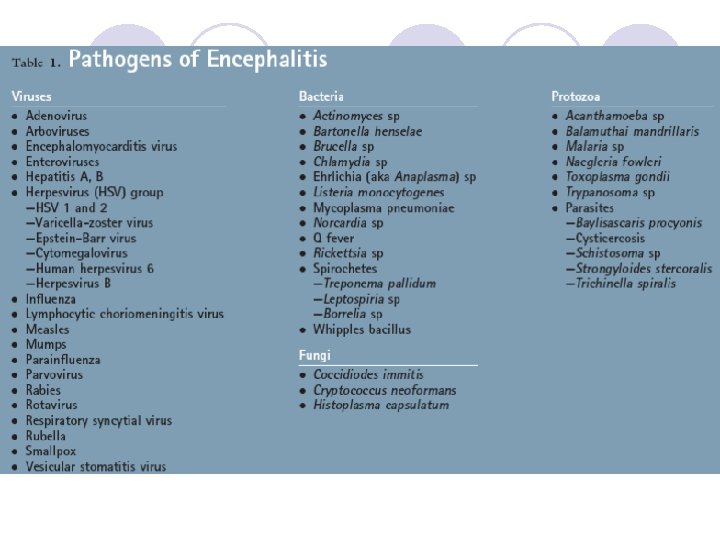
ENCEPHALITIS

Case Presentation l 16 yo old female presents with fever, headache, neck stiffness, swallowing difficulties and altered mental status l Symptoms have worsened over past 2 days. l Roommate noted a change in behaviour for the past week l 2 weeks ago had a bad URTI- missed 2 days of school

Encephalitis l Defined as acute CNS dysfunction with radiographic or laboratory evidence of brain inflammation l 1. Primary Encephalitis ¡ l cause bloodstream infection, then enter the CNS 2. Post- or Parainfectious ¡ ¡ not caused by direct CNS infection consequence of the host’s immune response

Encephalitis l HSV - typically infects neurons in the temporal lobe l Rabies - predominantly affects the pons, medulla, cerebellum, and hippocampus l Japanese encephalitis virus affects the brainstem and basal ganglia.

Post- Parainfectious Encephalitis l occurs days to weeks after the onset of an infection l hypothesized to be caused by an aberrant immune response against brain antigens such as myelin basic protein l Subsequent demyelination causes focal or global CNS dysfunction

Encephalitis - Epidemiology l overall incidence of hospitalization was 7. 3 cases/100, 000 annually l Children < 1 yo - 13. 7 cases/100, 000 per yr l Adults >65 yo - 10. 6 cases/100, 000 per yr

Clinical presentation l Fever l Headache l Altered mental status l Focal neurologic signs l spectrum of clinical evolution during encephalitis varies widely



Encephalitis l CT scan – nml at the onset of encephalitis. l MRI – much more sensitive for acute changes l EEG - helpful adjunct +/- localize the region of encephalitic involvement ¡ considerably more sensitive

Management l Appropriate antiviral, antimicrobial or antifungal therapies l Intravenous immune globulin, corticosteroids, or other immune system modulators.

Herpes Simplex Virus Encephalitis l Most common encephalitis diagnosed l Fever l Personality change l Autonomic dysfunction l Dysphagia l Seizures l Headache l Altered level of consciousness
 and CSF protein l CT")
HSV l Mildly elevated CSF WBC counts (lymphocyte predominant) and CSF protein l CT and MRI studies - normal if obtained early in the course of illness ¡ l Unilateral or bilateral temporal lobe involvement (most common finding) Diagnostic test - HSV DNA detection by PCR on the CSF ¡ ¡ both highly sensitive and specific If initial result negative, test should be repeated on a second CSF specimen.

Treatment l IV acyclovir 10 mg/kg per dose every 8 hours for 2 to 3 weeks. l Better ¡ age outcomes if: < 30 yo ¡ shorter duration of symptoms before initiation of treatment ¡ GCS >10 at the time of presentation.

Investigations l CT head l LP l CBC, Blood culture l Lytes l Glucose l ESR, CRP

l Back to our patient

Question #3 l For a patient who is suspected of having acute encephalitis, which of the following studies is most likely tobe helpful? l A. Cerebrospinal fluid glucose level. l B. Computed tomography scan. l C. Electroencephalography. l D. Magnetic resonance imaging. l E. Viral culture

Any Questions?

References C Waruiru and R Appleton Febrile seizures: an update Arch Dis Child. 2004 August; 89(8): 751– 756. l Jones T. Jacobsen SJ. Childhood febrile seizures: overview and implications International Journal of Medical Sciences. 4(2): 110 -4, 2007. l Baumann RJ. Duffner PK. Treatment of children with simple febrile seizures: the AAP practice parameter. American Academy of Pediatrics. Pediatric Neurology. 23(1): 11 -7, 2000 Jul. l AAP Practice Parameter: Long Term Treatment of the Child With Simple Febrile Seizure Pediatrics. 103(6) June 1999 l

References l Appleton R. Choonara I. Martland T. Phillips B. Scott R. Whitehouse W. The treatment of convulsive status epilepticus in children. Archives of Disease in Childhood. 83(5): 415 -9, 2000 Nov. l Riviello JJ Jr. Ashwal S. Hirtz D. Glauser T. Ballaban-Gil K. Kelley K. Morton LD. Phillips S. Sloan E. Shinnar S. American Academy of Neurology Subcommittee. Practice Committee of the Child Neurology Society. Practice parameter: diagnostic assessment of the child with status epilepticus Neurology. 67(9): 1542 -50, 2006 Nov 14.
5d14b87c0479f95167ff0714f408c2e8.ppt