138fe47a77aae75c74093bee10a1c943.ppt
- Количество слайдов: 26



Pediatric Lymphomas Dr. Hussein Alatabi MBCh. B, DCH, FICMS, CABP

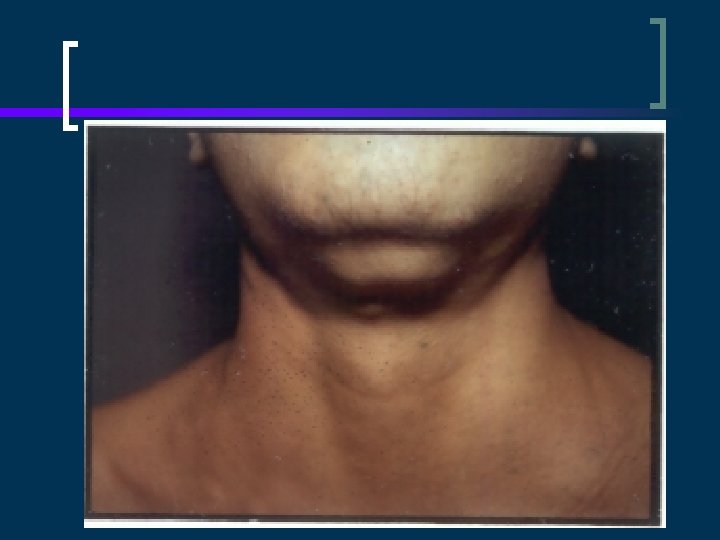
Cervical adenopathy

Concerns in enlarged LN n n Size >1 -2 cm Increasing size over 2 -4 weeks Matted or fixed Supraclavicular LN n n n Fevers >38. 5 for 2 -4 weeks Constitutional symptoms HSM

When to biopsy n n Supraclavicular node Increasing size over 2 -4 weeks Constitutional symptoms Asymptomatic enlarged nodenot decreasing in size over 6 weeks or not normal after 8 -12 weeks

Staging Evaluation Laboratory -CBC with smear -Chem profile LHD, uric acid n Disease specific -ESR, IL 2 R for HD -LP if head/neck NHL -BMA/Bx for all NHL, only IIB or higher HD n Radiology -CXR (PA & Lat) -CT scans neck, chest, abdomen -Gallium, bone scan -PET scan n

Lymphoma Staging n n n n Murphy Ann Arbor I: tumor at one site (nodal or extranodal -- “E”) II: two or more sites; same side of body (or resectable GI primary) III: both sides of body but not IV (& unresec. GI & mediastinal for NHL) IV: CNS or marrow involvement (Murphy); lung, liver, marrow, or bone for Ann Arbor (< 25% marrow) “B” sxs are defined for HD, as is “bulky disease” Head and neck (possibility of CNS involvement) is a further consideration for NHL PET or gallium
 LARGE CELL LYMPHOMA (<15%) (60%) LYMPHOBLASTIC LYMPHOMA (30 -40%) IMMUNOBLASTIC")
LYMPHOMA HODGKINS NON-HODGKINS (40%) LARGE CELL LYMPHOMA (<15%) (60%) LYMPHOBLASTIC LYMPHOMA (30 -40%) IMMUNOBLASTIC ANAPLASTIC (50%) BURKITT’S LYMPHOMA (40 -50%)

Non-Hodgkin’s Lymphoma u u u u Malignant solid tumor of immune system Undifferentiated lymphoid cells Spread: aggressive, diffuse, unpredictable Lymphoid tissue; BM and CNS infiltration High growth fraction and doubling time Dx and Rx ASAP Rapid CTX response; tumor lysis concern

Incidence/Etiology - NHL u u u 6% childhood cancer 60% of childhood lymphomas Peak age of 5 -15; M: F ratio of 2. 5: 1 Increased with u u SCIDS, HIV, EBV post t-cell depleted BMT post solid organ transplant Geographic, viral, genetic & immunologic factors
 ¡ 90 % immature T cells (very similar")
Types of NHL Lymphoblastic (30 -35%) ¡ 90 % immature T cells (very similar to T-ALL) n ¡ ¡ ¡ remainder pre-B phenotype (as in ALL) 50 -70% anterior mediastinum neck, supraclavicular, axillary adenopathy Classic: older child with intussusception
 --Mature B-cell phenotype --Burkitt's and non-Burkitt's --90% abdomen --Ascites")
Small non-cleaved cell (40 -50%) --Mature B-cell phenotype --Burkitt's and non-Burkitt's --90% abdomen --Ascites and intusussception --Endemic in Africa (Burkitt's), with EBV 97%

Burkitt Facts n n n 100 new cases/year in US, 2 -3: 1 male: female; mean age 11 years (in non-endemic form) small, noncleaved cell; mature B phenotype; intraabdominal (sporadic) or jaw (endemic) most common primary site 90% have t(8; 14) ¡ n others are 8; 2 or 8; 22 ¡ n (8 ~ c-myc; 14 ~ heavy chains) (2, 22 ~ light chains) Extremely rapidly-growing; tumor lysis issues
 - Anaplastic (Ki-1) lymphoma – ALK fusion protein - Diffuse")
Large-cell lymphoma (15 -20%) - Anaplastic (Ki-1) lymphoma – ALK fusion protein - Diffuse Large B-cell lymphoma (DLBCL) - - frequent Mediastinal involvement More like Hodgkin lymphoma than other NHLs “Peripheral T-cell” lymphoma Often involves skin, CNS, lymph nodes, lung, testes, muscles, and GI tract

n “low grade” lymphomas – rare in children ¡ ¡ Follicular marginal zone/MALT primary CNS (often seen with HIV infection) peripheral cutaneous (mycosis fungoides)
: pain, distention, jaundice, GI problems, mass Head/neck (13%):")
Clinical Presentations u u Abdomen: (35%): pain, distention, jaundice, GI problems, mass Head/neck (13%): lymphadenopathy, jaw swelling, single enlarged tonsil, nasal obstruction, rhinorrhea, cranial nerve palsies Mediastinum (26%): SVC syndrome CNS (rare): HA, V, irritability, papilledema +Fever, malaise, night sweats, wt. loss,

Prognosis affected by… u u u Incomplete remission in first 2 mos. Rx Large tumor burden (LDH >1000) Stages III and IV: CNS or BM involvement Delay in treatment Relapse **More favorable: Stage I or II, head/neck, peripheral nodes, GI tract

NHL Treatment u u Surgery for diagnostic bx or second look Radiation Therapy: emergency airway obstruction or CNS complication – may be used for local control of residual mass Chemotherapy: Combination chemo is usual, with overall cure rates 60 -80+%; high risk of tumor lysis and hyperuricemia Relapse: Re-induction, followed by BMT

Hodgkin’s Disease u u Immune system malignancy, involving B or T lymphocytes Reed-Sternberg cells Spread: slow, predictable, with extension to contiguous lymph nodes Infiltration to non-lymphoid organs is rare

Hodgkin’s disease with Reed Sternberg cell often CD 20+

Incidence and Etiology u u Hodgkin’s 5% of childhood cancers Bimodal peaks, at 15 -35 and >50; rare < 5 M: F ratio of 3: 1; variation r/t geography and SES, and type Increased in immunologic disorders, HIV, EBV
, 40 -60%, lower cervical, supraclavicular,")
Types of Hodgkin’s Lymphoma u u Nodular sclerosing (NS), 40 -60%, lower cervical, supraclavicular, mediastinal nodes Mixed cellularity (MC), 15 -30%; advanced disease with extranodal involvement Lymphocyte predominance (LP), 5 -15%, presents as localized disease Lymphocyte depletion (LD) (<5%); widespread disease
 that persists despite antibiotic therapy")
Clinical Presentation u u Painless lymph node swelling (90%) that persists despite antibiotic therapy Palpable non-tender, firm, mobile, rubbery nodes; Mediastinal adenopathy (60%); SVC Bulky: when mass is > 1/3 thorax diameter B symptoms: Fever of >38 C for 3 days, drenching night sweats, 10% weight loss

Mediastinal masses n n Risk for anesthesia (esp. if tracheal compression > 50% by CT) Least invasive diagnostic procedure therefore indicated (incl. thoracentesis) Emergent steroids or RT generally acceptable prior to biopsy HD and DLBCL tend to have areas of necrosis and therefore look more “bumpy” than T-ALL
 and Stage I non-bulky disease")
Prognosis FAVORABLE: <10, F, favorable subtypes (LP and NS) and Stage I non-bulky disease UNFAVORABLE: Persistently elevated ESR; LD histopathology; bulky disease--largest dimension >10 cm; B symptoms;

Treatment and Prognosis u u u Dependent on age, stage, and tumor burden RT alone, CTX alone RT: varies from involved field for localized disease to extended field to total nodal irradiation, inverted Y plus mantle most often multimodal therapy, with lowdose involved field RT and multi-agent CTX Combined modality 70 -90% LT cure
138fe47a77aae75c74093bee10a1c943.ppt