a5a6bc1e938928b9c7449f5827b4fded.ppt
- Количество слайдов: 30



Pediatric ED case Presented by F 2 劉品 Instructor 吳孟書醫師 Date 2008 -08 -27

Triage data Time: 2008 -8 -9 14: 26 l Age: 2 m 27 d/o l Gender: male l Weight: 6. 21 kg l l l T 36. 5 P 126 R 26 BP -/- (未測) E 4 V 5 M 6, Sp. O 2 98% 檢傷主訴: 抽搐發作後 檢傷分級: 二級
 T 36. 5 c, P 126, R 26 (3 m/o:")
Pediatric assessment triangle (PAT) T 36. 5 c, P 126, R 26 (3 m/o: P 120 -140, R 30 -50, BP 60 -70) Appearance Breathing Alert No Retraction Easy looking No Tachypnea Circulation CRT < 2 sec

Present illness l 4 days ago, while sleeping first seizure attack ¡ Reddish face Crying GTC with upward gaze for about 30 secs Post-ictal lethargy l 2 days ago, another attack (the same pattern) Seizure attacks for 2 times today No fever No diarrhea/vomiting, no cough/rhinorrhea. Good activity & appetite (150 ml q 4 h as usual) No travel or head trauma history. l DTa. P 1+ OPV 1 + Hib vaccine 7 days ago. l l l

Chief complaint l Seizure attack for 2 times today

Past and personal history l l l No previous admission or operation Normal newborn screen No regular medication Allergy: no known allergy to food or drug Birth History: G 2 P 2, NSD (39 wks), BBW: 3100 g Vaccination history 24 hr ¡ 3 d/o ¡ 1 m/o ¡ 2 m/o ¡ BCG: vaccinated Hep. B(1 st): vaccinated Hep. B(2 nd): vaccinated DTa. P 1+ OPV 1 + Hib : 7 days ago

Physical examination HEENT: Neurological examination: l Anterior fontanel: 2 f. b l Pupil: 3. 0/3. 0 (light reflex +) l Conjunctiva: Not injected. l Muscle power: l Sclera: anicteric. ¡ upper: 5/5 l Throat: no injection. ¡ lower: 5/5 l Tonsil: no exudation. ¡ symmetric l TM: no injection. l Babinski sign: bilateral Neck: no LAP. positive Chest: Clear breathing sound. HEART: regular; no murmur Abdomen: soft and normoactive. Extremities: free, CRT < 3 secs. Skin: No petechiae or ecchymosis

l Did the patient really have a seizure attack? l What are the important points for history taking and PE? l What are the most common etiologies of seizure? l How to approach a child with seizure?

Differential diagnosis of paroxysmal events Seizure disorders Pseudoseizures Head trauma l Loss of consciousness l Posttraumatic seizures Syncope l Hypovolemia l Hypoxia l Low cardiac output Sleep disorders l Nightmares l Night terrors l Narcolepsy l Sleep-apnea l Somnambulism Atypical migraines Movement disorders l Paroxysmal choreoathetosis l Tic disorders l Shudder attacks (tremor) l Benign myoclonus Psychiatric disorders l Day dreaming l ADHD l Panic attacks GI disorder l Sandifer syndrome (GERD) l Abdominal migraines l Cyclic vomiting Breath-holding spells l Pallid, cyanotic Apparent life-threatening event

History taking for children with seizure Preceding events Trauma Toxin / ingestion Fever Headache, nausea / vomiting l Diarrhea l l Associated symptoms l l l Aura Conscious disturbance Tongue biting Incontinence Postictal confusion Toxidrome Seizure pattern Generalized / focal l Duration l Past history Previous seizure / neurological problem l Anticonvulsant (changed dose or regimen, compliance) l Neurosurgery l Family history Travel history (neurocysticercosis…) Fleisher: Text book of pediatric emergency medicine. 2006

Physical exam for children with seizure Vital signs Entire body surveillance l Evidence of trauma (Head to toe) l Skin: neurocutaneous lesions / sweating / flush / cyanosis l Dysmorphism (congenital anomalies) l Evidence of hepatic, renal, or endocrine disorders Neurologic exam: l Asymmetric movements l Decerebrate or decorticate posture HEENT: l Pupils: shape, size, reactivity, and equality l Fundus exam: retinal hemorrhage / papilledema l Tympanic membranes: hemotympanum / AOM l Mouth: tongue injury Neck: l Meningeal signs Fleisher: Text book of pediatric emergency medicine. 2006

Etiology of seizures Idiopathic Infectious l l Brain abscess / CNS Parasites Encephalitis / meningitis Febrile (nonspecific) Syphilis Withdrawals l Alcohol / Anticonvulsants / BZD Toxicologic l l l Anticonvulsant / OHA / isoniazid Xanthines / TCA Phencyclidine/Sympathomimetic CO / Metals (Pb, Li) Organophosphate / Camphor Topical anesthetic / Cocaine Degenerative cerebral dz Metabolic l l Hepatic failure / Uremia Hyper: CO 2, osmolarity Hypo: Ca, Mg, Na, sugar, O 2, B 6 Inborn error Vascular l Stroke / HTN encephalopathy Oncologic l Primary/metastatic brain tumor Endocrine Addison's disease (adrenal) Hyper/hypothyroidism Obstetric (Eclampsia) l l Traumatic l l Cerebral contusion / ICH Diffuse axonal injury Hypoxic ischemic injury Congenital anomalies

Approach to seizure Obvious trauma - ATLS + Known seizure disorder? ICH or brain injury + Low serum Subtherapeutic glucose? drug level + Glucose 0. 25 -1 g/kg Fever? Breakthrough Hypoglycemic seizures - + Abnormal biochemistry? + Electrolyte (Na Ca Mg) Uremia (BUN, Cr) Hepatic failure (AST, PT) Metabolic (p. H, ammonia) Ingestion (toxiscreen) - Febrile convulsion Meningitis Occult trauma? 下頁續 Other infections
 Occult trauma? - + Focal neurological findings? - ATLS ICH")
Approach to seizure (續) Occult trauma? - + Focal neurological findings? - ATLS ICH or brain injury + Brain CT Idiopathic Mass lesion Ingestion Stroke Encephalitis Brain abscess Others Fleisher: Text book of pediatric emergency medicine. 2006
, Na, K, Ca, Cr,")
Initial order l Check CBC/DC, CRP, B/C, Blood gas (venous), Na, K, Ca, Cr, ALT, Bilirubin (T) l Finger sugar stat 113 mg/d. L l IVF: D 5 ¼ S run 25 ml/hr l Chest AP view including abdomen l Brain CT (C-) l Admit to OBN

Seizure attack at ED l Sudden onset crying and reddish face loss of consciousness, upward gaze and GTC attack l Management: ¡ Diazepam 2 mg iv stat (0. 32 mg/kg) ¡ O 2 flow by ¡ On pulse oximeter l The seizure subsided immediately after iv diazepam

l What is the emergent management of pediatric seizure in the ED?

Management of pediatric seizure Establish ABCs Lorazepam 0. 05 -0. 1 mg/kg Correct electrolytes Head trauma/IICP Tx Toxiscreen Correct anticonvulsant level Identify infectious cause Antipyretics (1 -2 times q 10 -15 min, max 4 mg) Consider diazepam PR 0. 5 mg/kg if no IV access Fosphenytoin 10 -20 mg PE/kg May give phenytoin 10 -20 mg/kg iv (< 1 mg/kg/min) Phenobarbital 10 -20 mg/kg Secure the airway Pyridoxine General anesthesia Barbiturate coma Pyridoxine: < 1 y/o refractory seizure (100 mg) Isoniazid toxicity (70 mg/kg) Fleisher: Text book of pediatric emergency medicine. 2006

Laboratory data WBC Segment Lym/At-Lym Monocyte Eos/Baso Hb/Hct MCV RDW Platelet 8000 23% 71%/2% 2% 1%/1% 10. 2/30. 1 83. 4 13. 3 369 K Creatinine ALT Na/K/Ca Sugar (F/S) Bilirubin (T) p. H CRP Pa. CO 2 Pa. O 2 HCO 3 SBE Sat% 0. 22 44 140/4. 9/9. 6 113 0. 7 7. 350 < 0. 5 48. 3 43. 2 (vein) 26. 1 0. 5 81. 4%

CXR

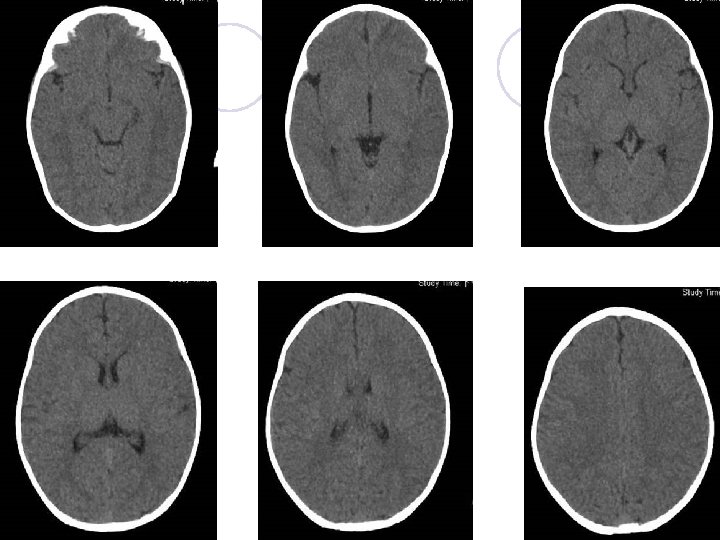
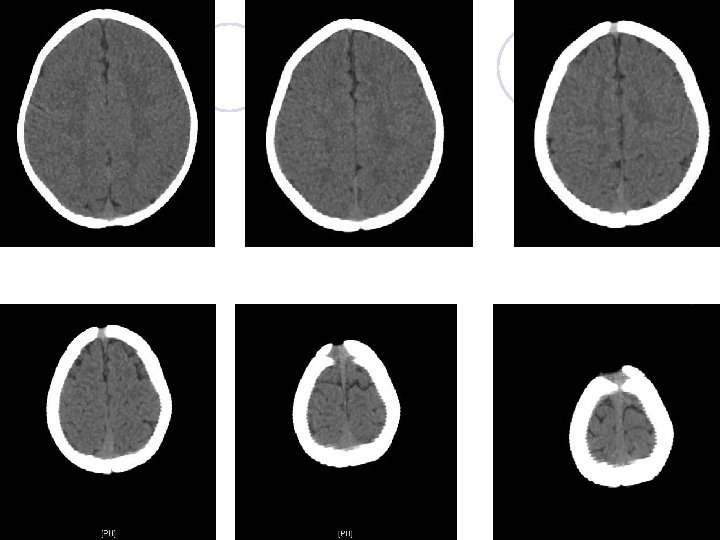
Brain CT
 l 15: 50 Admit to OBN, 加驗U/A: negative l 16:")
Hospital course (Day 1) l 15: 50 Admit to OBN, 加驗U/A: negative l 16: 25 Seizure attack again (GTC) in OBN ¡ 突然大哭,眼球上吊,雙手上舉,心跳加快 191/min,血氧由 96% 85%,臉部脹紅,隨即 雙手於胸前屈曲,全身抽搐,頭部向右抖動,持 續約1分鐘,抽搐完畢後臉色蒼白睡著 l 16: 30 Arrange CSF study ¡ 於腰椎穿刺過程中發生全身抽搐,血氧降至 85%, 臉部脹紅,頭部向右抖動,持續約1分鐘完畢, 臉色蒼白睡著 l 16: 35 Phenobarbital 90 mg ivf stat (15 mg/kg) and 15 mg ivf q 12 h (5 mg/kg/day)
![CSF study No evidence of CNS infection Appearance Protein WBC RBC Sugar [CSF/blood] Gram](https://present5.com/presentation/a5a6bc1e938928b9c7449f5827b4fded/image-25.jpg "CSF study No evidence of CNS infection Appearance Protein WBC RBC Sugar [CSF/blood] Gram")
CSF study No evidence of CNS infection Appearance Protein WBC RBC Sugar [CSF/blood] Gram stain H influenza B N. meningitidis S. pneumonia Gr. B strep. Clear/colorless 59 mg/d. L 2 /u. L (N/L = 1: 1) 27 /u. L 72/113 (mg/d. L) 0. 64 Negative Negative
 ¡ brain echo + EEG")
Hospital course l Day 3 (No more seizure attack) ¡ brain echo + EEG ¡ Ampicillin 300 mg q 6 h PCT : positive l 改Cefazolin 300 mg q 6 h ¡ Cefotaxime l Day 450 mg q 6 h 5: DC antibiotics l Day 7: shift to oral Phenobarbital 15 mg bid l Day 8: Discharge and OPD follow up
 report l No evidence of cortical dysfunction. l Few focal epileptiform activity")
EEG (sleep) report l No evidence of cortical dysfunction. l Few focal epileptiform activity over left frontocentral areas, and rarely over left middle temporal area. Brain echo l Left subependymal cyst l No midline shift. No ventricular dilatation

Final diagnosis l Infantile seizure l Left subependymal cyst

Key points l Clarify the history in children with suspected seizure attack (not always a true seizure) l Always stabilize the ABCs first in a patient with active seizure l In patients with the first episode seizure or post-trauma seizure, we should obtain proper neuroimage after initial stabilization

Thanks for your attention !
a5a6bc1e938928b9c7449f5827b4fded.ppt