a1cc3583860f854e49214a0905aae37e.ppt
- Количество слайдов: 87



Pediatric Board Review Endocrinology

Calcium

An otherwise healthy 6 -week infant presents with a generalized seizure. She is exclusively breast fed. The child is somewhat sleepy with a non focal examination. Glucose 88; Na 141, Ca 5. 1, Phos 9. 1, Mag 2. 1 The most likely diagnosis is: 1. 2. 3. 4. Pseudohypoparathyroidis m Hypoparathyroidism Vitamin D deficiency Albright’s hereditary osteodystrophy

Actions of PTH Ca 1. 2. 3. 25 OH Vit D 1 hydroxylase 1, 25 (OH)2 Vit D Gut NET EFFECT PO 4

This same 6 -week infant with hypoparathyroidism (Glucose 88; Na 141, Ca 5. 1, Phos 9. 1, Mag 2. 1) What is an important diagnostic consideration (i. e. what is the underling disorder causing the hypoparathyroidism)? Di. George syndrome – thymic aplasia, congenital heart disease, immune deficiency

Biochemical changes in rickets Ca PO 4 Bone Stage 1 Stage 2 N N Urine Minimal changes Rickets Aminoaciduria Phosphaturia Glycosuria Bicarbonaturia

Initial Ca: PO 4: Alk Phos: 9. 7 3. 1 2514 2 ½ weeks 9. 8 3. 5 2185 4 months 10. 5 6. 5 518

Which is consistent with vitamin D deficiency rickets? Calcium Phos Alk Phos 1. 2. 3. 4. 5. Normal Low Low Low High Low Normal Low High 10
 C.")
Choose correct answer A. Vitamin D deficiency rickets B. Renal osteodystrophy (renal rickets) C. Both D. Neither 1. Increased phosphate level B 2. Increased PTH level C 3. Increased creatinine level B

THYROID

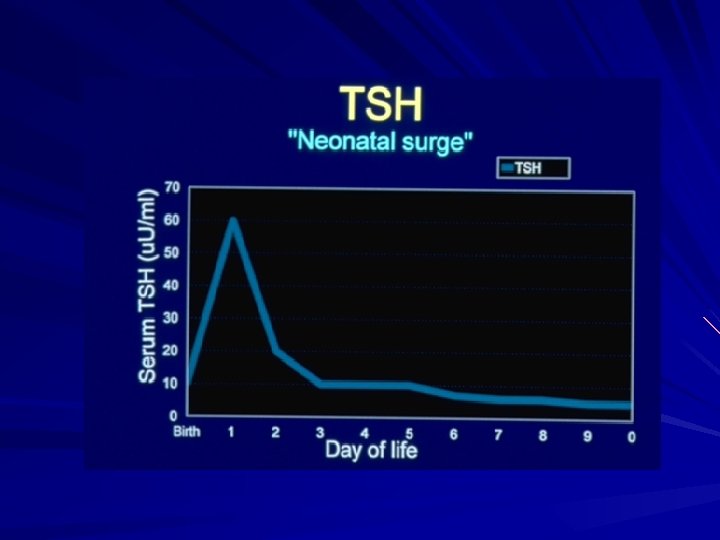
Baby A, born on 5/27/10. Newborn screening tests, performed on 5/29/10 revealed: Normal range TSH 37 µIU/ml < 20 T 4 10. 1 µg/dl 9 -19 Which statement is most accurate: 1. 2. 3. 4. Baby A has congenital hypothyroidism warranting urgent therapy Baby A will develop mental retardation if untreated Baby A likely does not have any thyroid abnormality Baby A has an altered hypothalamic set-point for T 4 10

You are contacted by your state Neonatal Thyroid Screening Program. Baby X was born on 1/4/10. His newborn screening tests, performed on 1/6/10 revealed: Initial filter paper Normal range TSH >200 IU/ml < 20 T 4 2. 1 g/dl 9 -19 Venipuncture: (1/25/10) TSH 488 IU/ml T 4 1. 2 g/dl Normal range (0. 3 -5. 5) (4. 5 -12. 5)

Congenital hypothyroidism § Thyroid dysgenesis/agenesis § Prevalence 1 in 4, 000 [Whites 1 in 2, 000; Blacks § § 1 in 32, 000] 2: 1 female to male ratio Clinical features include: hypotonia, enlarged posterior fontanelle, umbilical hernia, indirect hyperbilirubinemia Laboratory findings: Very high TSH and low T 4 Therapy: Thyroxine – keep TSH in normal range


6 month female with congenital hypothyroidism . . following 4 months therapy

A baby with gastroschisis has the following TFTs on day 5 of life: T 4 2. 1 μg/d. L (4. 5 -12. 5) TSH 2. 3 μIU/m. L (0. 3 -5. 0) The most likely diagnosis is: 1. 2. 3. 4. 5. Hypothyroidism due to thyroid dysgenesis Central hypothyroidism TBG deficiency Hypothyroidism from excess iodine exposure Normal thyroid function (as the TSH is normal) 10

Central hypothyroidism - rare vs. TBG deficiency 1: 2800
 § Major product secreted by the thyroid § Circulates bound to")
Thyroxine (T 4) § Major product secreted by the thyroid § Circulates bound to thyroid binding proteins § § - thyroid binding globulin (TBG) Only a tiny fraction (< 0. 1%) is free and diffuses into tissues When we measure T 4, we measure the T 4 that is bound to protein The level of T 4 is therefore largely dependent on the amount of TBG Changes in T 4 may reflect TBG variation rather than underlying pathology

Central hypothyroidism TBG deficiency Free T 4 Low Normal TBG level Normal Low T 3 RU Low High

Thyroid function in a 17 year old: TSH: 3. 7 µIU/ml T 4: 13. 4 µg/dl Normal range 0. 3 -5. 5 4. 5 -12 Which of the following medication could explain the thyroid function abnormality 1. INH 2. Retinoid acid 3. Ciprofloxacin 4. Ortho Tri-Cylen 5. Doxycycline 10

Conditions that cause alterations in TBG Increased TBG Infancy Estrogen - OC Pill - pregnancy Familial excess Hepatitis Tamoxifen treatment Decreased TBG Familial deficiency Androgenic steroid treatment Glucocorticoids (large dose) Nephrotic syndrome Acromegaly

A 12 -yr female has diffuse enlargement of the thyroid. She is asymptomatic. Her disorder is most likely associated with which of the following pathological processes 1. Infectious 2. Inflammatory 3. Autoimmune 4. Toxic (drug) 5. Neoplastic 10

Normal thyroid Hashimoto thyroiditis

DC u u 16 year 7 month Growth failure x 1 1/2 years §Labs: Labs TSH: T 4: 1008 µIU/ ml <1. 0 µg/dl (0. 3 -5. 0) (4 -12) Antithyro Ab. 232 U/ml A-perox Ab. 592 IU/ml (0 -1) (<0. 3) Prolactin: 29 ng/ml (2 -18) Cholesterol: 406 mg/dl (100 -170)

DC Start of thyroxine

Hashimoto thyroiditis Background: Background Autoimmune destruction of the thyroid Family history in 30 -40% Lymphocytic infiltration Clinical: Clinical Growth failure, constipation, goiter, dry skin, weight gain, slow recoil of DTR Laboratory: Laboratory High TSH Anti-thyroglobulin and anti-peroxidase antibodies Therapy: Therapy Thyroxine

15 year old female with a history of easy fatigability. Found to have an elevated pulse rate at recent MD visit Thyroid function: TSH < 0. 1 IU/ml T 4 14. 8 g/dl T 3 580 ng/dl Normal range 0. 3 -5. 5 4. 5 -12 90 -190

Eye changes Restlessness, poor attention span Goiter Tachycardia, wide pulse pressure Increased GFR - polyuria Menstrual abnormalities Myopathy Diarrhea
![Therapy for Graves disease: Antithyroid medication (Methimazole or Propylthiouracil [PTU]) Pros : 25% remission](https://present5.com/presentation/a1cc3583860f854e49214a0905aae37e/image-30.jpg "Therapy for Graves disease: Antithyroid medication (Methimazole or Propylthiouracil [PTU]) Pros : 25% remission")
Therapy for Graves disease: Antithyroid medication (Methimazole or Propylthiouracil [PTU]) Pros : 25% remission rate every 2 years Cons: Drug induced side effects - skin rashes, agranulocytosis, lupus-like reaction Radioactive iodine (131 I) Pros : Easy. Essentially free of side effects Cons: Long term hypothyroidism Surgery Blockers if markedly hyperthyroid

Sexual differentiation

Ambiguous genitalia is found in a newborn. The baby is noted to be hyperpigmented. Ultrasound demonstrates the presence of a uterus. The most useful test to aid in the diagnosis of this medical condition is: 1. 2. 3. 4. 5. Testosterone 17 -hydroxyprogesterone Serum sodium and potassium DHEAS/androstenedione ratio 10
 pregnenolone 3 -")
Cholesterol Desmolase Pregnenolone 17 -OH 3 - -HSD Progesterone 17 (OH) pregnenolone 3 - -HSD 17 -OH 21 -OH DOCA 11 -OH Corticosterone ALDOSTERONE 17 (OH) progesterone DHEA 3 - -HSD Androstenedione 21 -OH Compound S 11 -OH CORTISOL TESTOSTERONE

If she has salt wasting congenital adrenal hyperplasia, which abnormalities are likely to develop. True or False for each a) Increased serum potassium b) Decreased serum sodium T T c) Decreased bicarbonate T d) Decreased plasma cortisol T e) Increased plasma renin activity T

A 1 -year male infant has non palpable testes. Of the following, the most appropriate next step would be: 1. 2. 3. 4. 5. Re-examination in 18 months Refer the patient for an exploratory laparotomy Begin therapy with LHRH Measure the plasma testosterone after stimulation with HCG Begin therapy with testosterone enanthate, 50 mg IM monthly for 3 months. 10

History 9 day old male infant 1 day history of decrease feeding, vomiting and lethargy. Examination Ill appearing infant with poor respiratory effort Vital signs: T 99 F HR 100/min BP 61/40 RR 24/min Resp: Subcostal retractions but clear to auscultation Cardiac: Regular rate and rhythm. Normal S 1 and S 2 Abdomen: Soft, non distended. Non tender. No HSM Neuro: Lethargic. No focal deficit Genitalia: Normal male. Bilateral descended testes

Laboratory data: WBC 16. 7 Hb 16. 4 Hct 49 Plt 537 K Na 121 K 9. 3 Cl 83 CO 2 6. 7 Glucose 163 BUN/Creat 33/0. 2 CSF: Chemistry: Protein 74 Glucose Microscopy: WBC 6 RBC 82 100

Emergency therapy Fluid resuscitation: 20 ml/kg Normal saline Glucocorticoid 2 mg/kg Solucortef IV Monitor EKG

Modes of presentation Classical h. Simple virilizing h. Virilizing with salt loss “Non classical” / Late onset
 h. Monitor growth, 17 -OHP, urinary pregnanetriol")
Therapy and evaluation of therapy Glucocorticoid (Hydrocortisone) h. Monitor growth, 17 -OHP, urinary pregnanetriol Fluorocortisol (Florinef 0. 1 – 0. 45 mg/day) h. Blood pressure, plasma renin activity (PRA) Supplemental salt h. Until introduction of infant food

History 15 year female presents with primary amenorrhea Breast development began at 10 years Examination Height: 5 ft 7 in Weight 130 lb Tanner 5 breast development Scant pubic hair What is your diagnosis?

Complete androgen insensitivity XY Genotype Testosterone Androgen Receptor tase ma Aro Estradiol Estrogen Receptor

15 yr female presents with primary amenorrhea. Breast development began at 10 y Tanner 5 breasts, scant pubic hair Which of the following clinical features is the most likely to give you the correct diagnosis 1. 2. 3. 4. 5. Blood pressure in all 4 extremities Careful fundoscopic examination Rectal examination Measurement of blood pressure with postural change Cubitus valgus and shield shaped chest 10

Gonadal Primordia Female No SRY TESTIS OVARY No AMH No testosterone nor DHT Mullerian Wolfian duct regression ducts Fallopian tubes Uterus Upper vagina Sertoli cells Leydig cells Testosterone No AMH Mullerian duct regression Wolfian ducts DHT Normal female external genitalia Epidymus Normal male Vas deferens Seminal vesicles ext. genitalia

Gonadal Primordia Y Chromosome No AMH SRY TESTIS Sertoli cells No testosterone nor DHT AMH Mullerian Wolfian duct regression ducts Fallopian tubes Uterus Upper vagina Mullerian duct regression Normal female external genitalia Leydig cells Testosterone Wolfian ducts DHT Epidymus Normal male Vas deferens Seminal vesicles ext. genitalia

Gonadal Primordia Y Chromosome No AMH SRY TESTIS Sertoli cells No testosterone nor DHT AMH Mullerian Wolfian duct regression ducts Fallopian tubes Uterus Upper vagina Mullerian duct regression Normal female external genitalia Leydig cells Testosterone Wolfian ducts DHT Epidymus Normal male Vas deferens Seminal vesicles ext. genitalia

Early Puberty

The earliest sign of puberty in a male is: 1. Enlargement of 2. 3. 4. 5. the penis Enlargement of the testes Growth acceleration Pubic hair growth Axillary hair growth 5

2 year old girl with breast development. No growth acceleration. No bone age advancement No detectable estradiol, LH or FSH The most likely diagnosis is: 1. Ingestion of her 2. 3. 4. 5. mother’s OCPs Precocious puberty Premature adrenarche Premature thelarche Mc. Cune Albright Syndrome 10

Benign Premature Thelarche Isolated breast development – 80% before age 2 – Rarely after age 4 Not associated with other signs of puberty (growth acceleration, advancement of bone age) Children go on to normal timing of puberty and normal fertility Benign process Routine follow-up

5 year female with 6 months of pubic hair growth. Very fine axillary hair as well as adult odor to sweat. No breast development, no growth spurt The most likely diagnosis is: 1. 2. 3. 4. 5. Precocious puberty Benign premature adrenarche Non-classical congenital adrenal hyperplasia Adrenal tumor Pinealoma 10

Benign Premature Adrenarche Production of adrenal androgens before true pubertal development begins Presents as isolated pubic hair in mid childhood – No growth acceleration – No testicular enlargement in boys If normal growth rate, routine follow-up If accelerated growth and/or bone age advancement, screen for – CAH – Virilizing tumor (adrenal/gonadal)

Choose correct answer A. Premature theralche B. Premature adrenarche C. Both D. Neither 1. Growth acceleration D 2. Normal adolescent sexual development C 3. Onset of gonadal function usually in 3 -4 years B

You suspect a 16 year female has Turner syndrome. The most definitive diagnostic test is 1. Buccal smear 2. Chromosome analysis 3. Measuring her FSH and LH 4. Determining her bone age 5. Determining her testosterone level 5

5 year old girl with pubic hair and rapid growth. She has no breast development Possible sources of androgens: 1. Liver F 2. Adrenal T 3. Ovary T 4. Pituitary F 5. Pineal F

5 year old girl with pubic hair and rapid growth. She has no breast development Which of the following should be considered Answer T or F for each: a) Central precocious puberty F b) Congenital adrenal hyperplasia T c) Mc. Cune Albright syndrome F d) Benign premature adrenarche F e) Adrenal tumor T

When does puberty occur? Classic teaching – 8 -13 in girls (menarche ~ 2 years after onset of puberty) – 9 -14 in boys Case: Breast development: 6 years Mother had menarche: 9. 5 years

Why Reactivation of hypothalamic – pituitary –gonadal axis
 precocious puberty Clock turns on early Idiopathic > 95 % girls")
Gonadatropin dependent (central) precocious puberty Clock turns on early Idiopathic > 95 % girls ~ 50 % boys – Hypothalamic hamartoma (Gelastic seizures) – NF (optic glioma) – Head trauma – Neurosurgery – Anoxic injury – Hydrocephalus

Treatment Why – Psychosocial – Height What – Gn. RH agonist

Gonadotropin independent precocious puberty

7 year male presents with 6 month history of pubic and axillary hair growth as well as adult body odor. Mother thinks he is growing faster than his peers No exposure to androgens PM&SH – nil of note Mother had menarche at 12 yr Father had normal timing of his puberty Medications – none
 Weight 40 th percentile No")
Height 50 th percentile (last height at 25 th) Weight 40 th percentile No café au lait macules No goiter Heart and lungs: normal Abdomen: Firm hepatomegaly with irregular border Prepubertal Asymmetric Adrenal source Enlarged testicle Pubertal Precocious puberty
 Weight 40 th percentile No")
Height 50 th percentile (last height at 25 th) Weight 40 th percentile No café au lait macules No goiter Heart and lungs: normal Abdomen: Firm hepatomegaly with irregular border Genitalia: Pubic hair - Tanner 2 Scrotal thinning Testes 5 ml bilaterally (pubertal >3 ml) Rest unremarkable
 FSH")
7 year male with signs of puberty Gonadotropins LABS: Testosterone 48 ng/dl (<10) FSH <0. 1 m. IU/m. L LH <0. 1 m. IU/m. L TSH T 4 1. 0 μIU/m. L 8. 9 μg/d. L Pubertal Central precocious puberty LH G Leydig cell

Precocious puberty in the male Gonadotropins Prepubertal Pubertal Gonadotropin independent precocious puberty HCG Central precocious puberty LH * * G Mc. Cune Albright Familial male syndrome Precocious puberty (testotoxicosis) G Leydig cell 1. Gonadotropin independent PP 2. Polyostotic Fibrous Dysplasia 3. Café au lait macules

Final diagnosis: Gonadotropin independent precocious puberty secondary to an βHCG secreting hepatoblastoma
")
5 year old with breast development and growth acceleration - Estradiol 62 pg/ml (<10) - FSH <0. 1 m. IU/m. L - LH <0. 1 m. IU/m. L Gonadotropin independent precocious puberty

Mc. Cune Albright syndrome: 1. Café au lait macules 2. Gonadotropin independent precocious puberty 3. Polyostotic fibrous dysplasia

Growth disorders and delayed puberty
 Primary gonadal failure - Chromosomal - iatrogenic")
Delayed puberty Hypogonadism Hypergonadotropic Hypogonadism (↑FSH, LH) Primary gonadal failure - Chromosomal - iatrogenic (cancer therapy) - autoimmune oophoritis - galactosemia - test. biosynthetic defect Hypogonadotropic Hypogonadism ( FSH, LH) Constitutional delay Central Hypogonadism - Isolate gonad. def. - MPHD - Kallmann (anosmia) - Functional

A 15 yr boy has short stature and delayed puberty. He is now in early puberty (Tanner 2). His parents are of average stature. His height and weight are just below 3 rd percentile. All of the following are likely EXCEPT: 1. 2. 3. 4. 5. A bone age of 12 ½ years Growth hormone deficiency Adult height in the normal range Acceleration of growth and sexual maturation over the next 2 years. History of normal length and weight at birth 10

A 15 yr male has delayed puberty. He also has headaches, diplopia and increased urination. His height is < 3 rd percentile. Which of the following is the most likely diagnosis? 1. Diabetes mellitus 2. Pinealoma 3. Cerebellar tumor 4. Craniopharyngioma 5. Pituitary adenoma 10
. He is")
A 14 yr male has tender gynecomastia (3 cm in diameter bilaterally). He is in early to mid puberty. In most cases the best management for this gynecomastia is: 1. 2. 3. 4. 5. Treatment with an antiestrogen (e. g. Tamoxifen) Treatment with an aromatase inhibitor Treatment with a dopamine agonist (bromocryptine) Surgery Reassurance 10

Diabetes

A 12 year female patient presents with a 4 week history of polyuria, polydipsia, and marked weight loss. She is noted to have deep, sighing respiration. Glucose is 498 mg/d. L, p. H is 7. 06. Her electrolytes show Na 132, K 4. 8, Cl 95 CO 2 6 BUN 20 Creat 0. 9. The MOST important initial management is: 1. 2. 3. 4. insulin drip 0. 1 u/kg/hr ½ NS with 40 meq K at 2 x maintenance Bicarb 1 meq/kg slowly over 1 hour 20 ml/kg normal saline bolus IV 10
 -0109 -120188 Which")
GTT in a 16 year obese female: Time Glucose (mg/d. L) -0109 -120188 Which of the following statements are correct? This patient has: 1. 2. 3. 4. Type 2 diabetes Impaired glucose tolerance but normal fasting glucose Normal glucose tolerance Both impaired fasting glucose and impaired glucose tolerance 10

Definition of diabetes Diabetes ≥ 126 ≥ 200 < 126 < 200 Pre-diabetes ≥ 100 ≥ 140 < 100 < 140 Normal Fasting 2 hr post load

This obese patient with IFG and IGT is at risk for the development of all the following EXCEPT 1. 2. 3. 4. 5. Type 2 diabetes Metabolic syndrome Dyslipidemia Hypertension Slipped capital femoral epiphysis Hashimoto thyroiditis 10

A 13 year male has new onset type 1 diabetes mellitus. Therapy for this child may include all of the following EXCEPT: 1. Glargine (Lantus) and Lipro insulin (Humalog) 2. Detemir (Levemir) and Aspart insulin (Novolog) 3. Metformin 4. Analog insulin administered via an insulin pump 10

Miscellaneous

Side effects of corticosteroids include all of the following except 1. hypertension 2. hypoglycemia 3. decrease bone mineralization 4. myopathy 5. cataracts 10

What is the most likely diagnosis in this newborn infant? 1. 2. 3. 4. 5. Mother has SLE Anasarca from cardiac failure Systemic allergic reaction Congenital nephrotic syndrome Turner syndrome 10

5 year old male with short stature 1. 2. 3. 4. 5. Turner syndrome VATER syndrome Albright’s hereditary osteodystrophy Noonan syndrome Goldenhar syndrome 10

A moderately obese adolescent female has irregular periods, hirsutism and acne. Of the following, which is the most likely diagnosis? 1. 2. 3. 4. 5. Cushing syndrome Polycystic ovarian syndrome Virilizing adrenal tumor Non-classical CAH Hyperprolactinemia 10

Choose correct answer A. Diabetes mellitus B. Diabetes insipidus C. Both D. Neither 2 Na + BUN/2. 8 + Gluc/18 1. Osmolality of serum > 300 Osm/L 2. Osmolality of urine > 500 m. Osm/L 3. Hypernatremia

Choose correct answer A. Diabetes mellitus B. Diabetes insipidus C. Both D. Neither 2 Na + BUN/2. 8 + Gluc/18 1. Osmolality of serum > 300 Osm/L C 2. Osmolality of urine > 500 m. Osm/L A 3. Hypernatremia B
a1cc3583860f854e49214a0905aae37e.ppt